
Abstract
Background:
Asia Pacific region has the highest number of Internet users in the world. In 2013, India had 190 million Internet users, and out of these, 130 million belonged to urban areas, and 60 million belonged to rural areas. This study was conducted to estimate the prevalence of Internet addiction (IA) and determine its psychosocial factors among Indian adolescents (12–18 years) living in the urban and rural areas of India.
Methods:
A cross-sectional analytical study was conducted among 385 students of class 8th–10th aged 12–18 years in government and private schools in Chandigarh (urban) and Kangra district (rural), Himachal Pradesh, India. Young’s IA tool, Patient Health Questionnaire, Reynold’s Suicidal ideation questionnaire, and Rosenberg’s self-esteem questionnaire were used. IBM Statistical Package for Social Sciences, version 21 was used for data analysis.
Results:
IA prevalence among adolescents was significantly higher in Kangra (25.4%) than in Chandigarh (4.3%). Significant determinants of IA included adolescents aged 13–15 years studying in the 9th class (adjusted odds ratio (aOR) = 3.9, 95% confidence interval (CI) = 1.30–11.76); 14–18 years studying in the 10th class (aOR = 3.6, 95% CI = 0.87–15.18), watching Facebook (aOR = 9.7, 95% CI = 3.33–28.29) and TikTok apps (aOR = 3.3, 95% CI = 1.22–9.10); and adolescents with symptoms of depression (aOR = 6.6, 95% CI = 2.6–17.01). Living in an urban area (Chandigarh) was a protective factor for IA (aOR = 0.2, 95% CI = 0.19–0.53).
Conclusions:
One in every four adolescents living in the rural area had IA. Adolescents studying in ninth and tenth grade, having symptoms of depression, and using social media apps like Facebook and TikTok were prone to IA.
Introduction
The Asia Pacific region has the highest (53.5%) number of Internet users in the world. 1 Just like the growth rate of this region, the urge to use the Internet has also increased, which is concerning. 2 “Internet Addiction” (IA) has been described as an impulse control disorder that does not involve using intoxicating drugs but is very similar to “pathological gambling” as per Young. 3 India accounts for 755 million Internet users, the 2nd highest globally until December 2020. 4 Moreover, in 2013, India had 190 million Internet users, and out of these, 130 million belonged to urban areas, and 60 million belonged to rural areas. 5 Internet use is widespread among adolescents, 2 so the psychosocial associates and correlates of IA in this age group need to be explored, especially in India. 6 The prevalence of IA among individuals aged 12–26 years varies from 2% to 26.5% in different countries.7–9 In India, it ranges from 8% to 26%.10–12 Many studies have suggested a conceivable relationship between the surplus use of the Internet by adolescents and its corresponding adverse health outcomes such as symptoms of depression, 13 low self-esteem, attention deficit hyperactivity disorder, 14 anxiety, suicidal ideation, 13 pathological traits, poor school performance and decreased productivity. 13 In India, it is essential to further explore the multifactorial association between psychological effects and IA. 2
Adolescents are particularly vulnerable to technological dependencies due to their developmental stage, which includes social exploration and identity formation. Digital behaviors and technological dependencies are shaped by social structures, technological access, geographical and socioeconomic variations, and cultural norms. The adolescent period is an essential area of focus as behavior modification should be done in the early stages of life. 15 Comparative studies on the extent of IA and its associated psychosocial factors in rural and urban areas of North India are limited. 15 This study was conducted to estimate the prevalence and ascertain the psychosocial factors of IA in different geographical (urban and rural) and socioeconomic environments. It also aimed to find the correlations between IA and mental health so that targeted interventions for mitigating its negative effects can be guided. The results of this study highlighted the need for context-specific strategies to address the growing digital challenges faced by adolescents and provided evidence for more informed approaches to digital wellness.
Methodology
Study Area
The study was conducted in Kangra, Himachal Pradesh, and Chandigarh, North India, to represent rural and urban areas, respectively. Kangra had a total population of 1.5 million, with 94.2% of the population living in rural areas, 16 and adolescents comprising 19% of the total population, as per Census of India 2011. 16 Chandigarh, a Union Territory, had a population of 1.1 million, with 97% of the population living in urban areas in 2011. 17 The adolescents in Chandigarh constituted 20%-22% of the total population. 18
Study Design and Duration
A cross-sectional analytical study was conducted from May 2019 to June 2019.
Study Population and Settings
The adolescents studying in 8th to 10th classes ranged between 12 and 18 years of age. Adolescents selected from private (N = 367) and government schools (N = 616) from the study areas were eligible to participate in this study. The students who had Internet access, either through their parents or their mobile phones/laptops/computers, and had frequent (up to six times a week) or everyday access to cyber cafes were included. The students who had been diagnosed with chronic long-term illnesses with medical records were excluded from the study.
Sample Size
The sample size was estimated using the formula “N = 4pq/d 2 ”, 19 where, “P” = prevalence of IA (assumed to be 22%), 11 “q” = 1-p, P = .78, “d” = allowable error of estimated prevalence and assumed to be 10%. After considering the design effect of 2, the sample size was calculated as “N = 69 × 2 = 138.” Assuming a nonresponse rate of 15%, the sample size was estimated at “N = 138 + 15% = 159.” Hence, the minimum sample size was estimated to be 160 each in rural and urban areas, with a total sample size of 320.
Sampling Technique
A multistage cluster sampling technique was used to select the schools and the study participants, as shown in Figure 1. In the first stage, the list of all government and private schools was collected from the government websites of the relevant departments. In the second stage, one school was randomly chosen from the procured lists. In the third stage, one section was randomly selected from each 8th, 9th, and 10th grade. A grade was assumed as a cluster with a minimum of 30 students. The minimum cluster required per area in this study was estimated by using the following formula:
Flow Diagram of Multistage Cluster Sampling for Selection of Schools and Students.
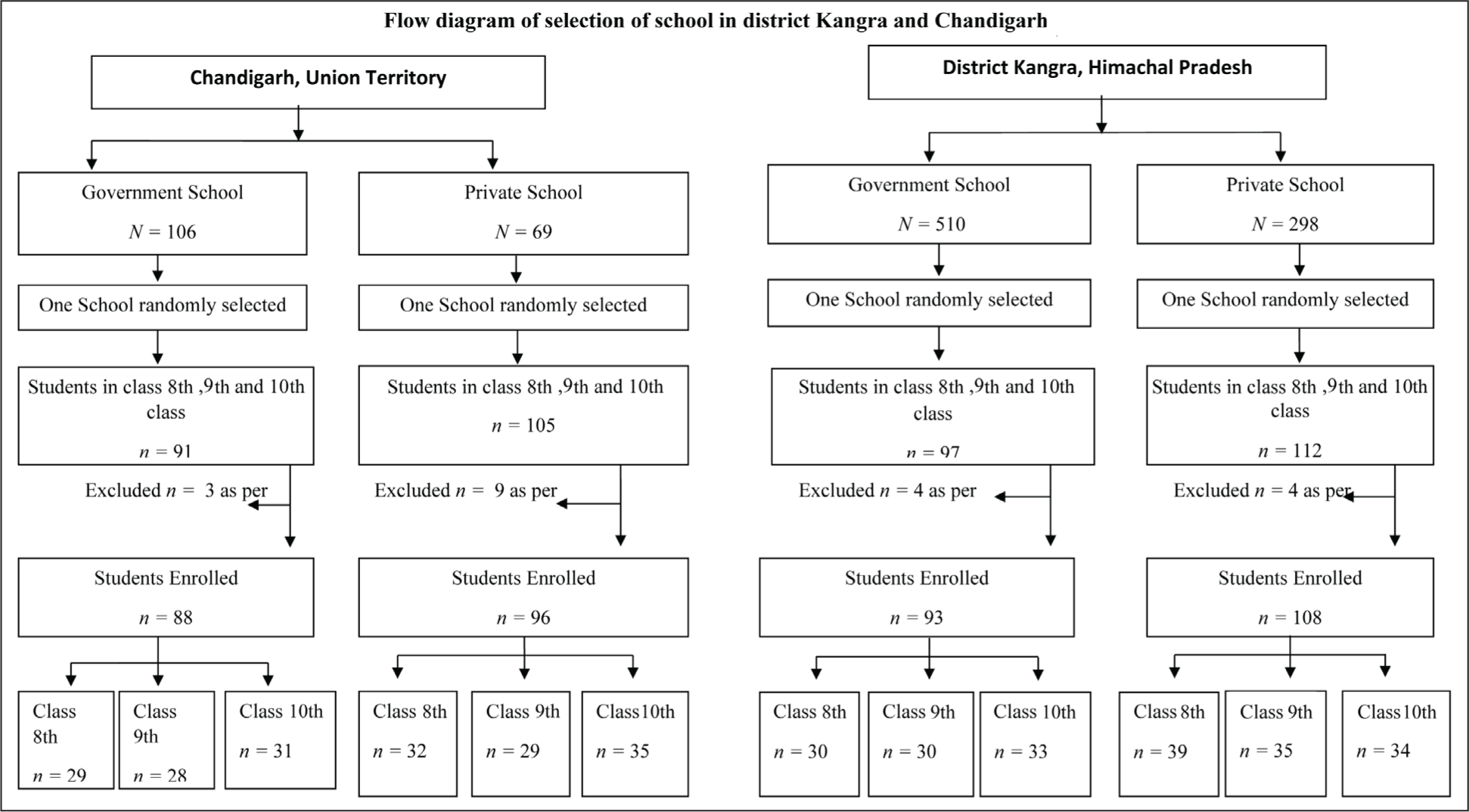
Minimum clusters required “(k) = m/n” where, “m” = sample size; “n” = minimum cluster size; 160/30 = 5.3. So, six clusters were included from each study area. Hence, three sections (one each of 8th, 9th, and 10th grade) from a government school and three sections (one each of 8th, 9th, and 10th grade) from a private school were selected in each study area. We recruited all the students from the selected section. The final study sample was 385 (Figure 1).
Data Collection Tools and Methods
The pretested bilingual (English and Hindi) tools used in the study were as follows:
The background information of adolescents regarding age, class, gender, father’s education, father’s occupation, father’s income, social media use etc., was also obtained using a pretested proforma. All the questionnaires/proforma were self-administered by the students. The lead author of the study collected the filled questionnaires. A prefixed date and day were scheduled for disseminating the questionnaires in the study schools.
Data Analysis and Management
IBM Statistical Package for Social Sciences for Windows, version 21, was used for data analysis. Descriptive statistical calculations for continuous (mean, standard deviations) and categorical variables (proportions) were done. The difference in proportions between groups was estimated using the chi-squared test. The correlations (r) between IA score and age and psychological variables like depression, self-esteem, and suicidal ideation were calculated. A binary multivariate logistic regression model was used to identify the significant predictors of the IA. Independent variables and dependent variables are given in Supplementary Table 1. The P value was considered significant at the 95% level.
Background Characteristics of Students in Government and Private Schools in Chandigarh (Urban area) and Kangra, District Himachal Pradesh (Rural Area).
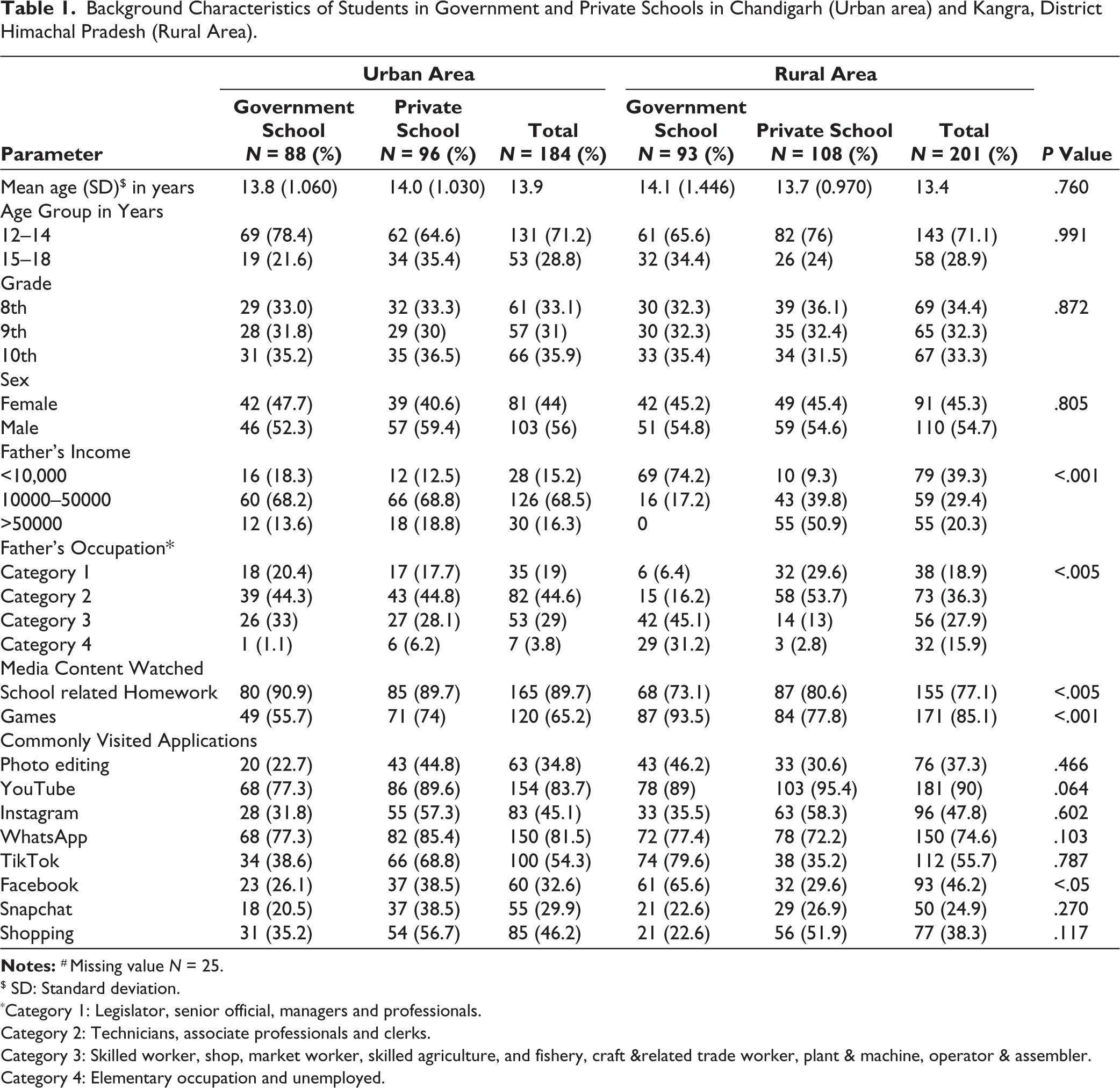
$ SD: Standard deviation.
*Category 1: Legislator, senior official, managers and professionals.
Category 2: Technicians, associate professionals and clerks.
Category 3: Skilled worker, shop, market worker, skilled agriculture, and fishery, craft & related trade worker, plant & machine, operator & assembler.
Category 4: Elementary occupation and unemployed.
Ethical Clearance
Ethical clearance was obtained from the Institute’s Intramural Ethics Committee (INT/IEC/2019/001038; dated April 29 2019). The Director of Higher Education Chandigarh (NO913-DSE-UT-S5–11(65)11; dated March 19, 2019) and Directorate of government school, Shimla (EDN-HE(21)F(11)01/2019-MISC; dated June 10, 2019) permitted us to conduct the study. A written informed consent was obtained from the parents, and assent was obtained from all the students before data collection.
Results
The total adolescents enrolled in the study were 385, with 184 (88 government and 96 private schools) in Chandigarh and 201 (93 government and 108 private schools) in Kangra district Himachal Pradesh. The mean age of the adolescents (N = 385) in the rural and urban areas was ±13.4 years and ±13.9 years, respectively. There were no significant differences in the background characteristics of the children belonging to the rural and urban areas, except for the father’s occupation and father’s income (P < .001). The adolescents who used the Internet for completing homework were significantly (P < .005) more in the rural (77.1%) as compared with the urban areas (89.7%). Playing games on electronic media devices with the Internet was also significantly (P < .001) more in the rural (85.1%) as compared with the urban areas (65.2%). Amongst all the social networking sites, the proportion of Facebook users was significantly (P < .05) higher in the rural (46.2%) as compared with the urban areas (32.6%; Table 1).
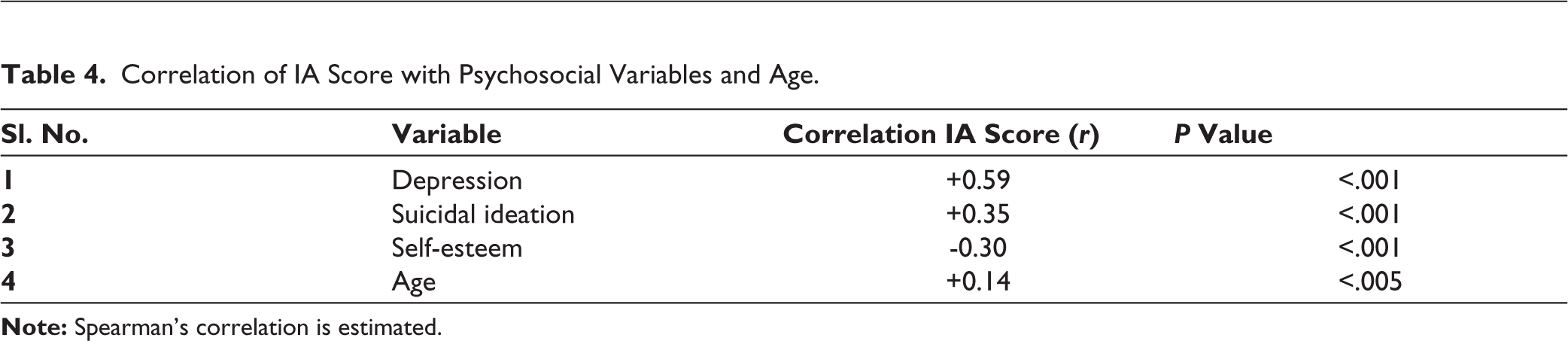
The overall prevalence of “significant IA” was significantly (P < .05) higher in rural areas (25.4%) as compared to urban areas (4.3%; Table 2). Moderate depression was significantly (P < .001) higher among the Internet addicts (30.5%) than the nonaddicts (7.1%). The propensity toward having suicidal thoughts was significantly higher (P < .001) amongst the Internet addicts (23.7%) than the nonaddicts (8%). The proportion of adolescents with lower self-esteem was significantly higher (P < .001) among the addicts (36.8%) than the nonaddicts (9.5%; Table 3). There was a positive correlation between IA scores and symptoms of depression (r = +0.59, P < .001) and suicidal ideation (r = +0.35, P < .001). Age was positively correlated (r = +0.14, P < .005) with IA, and the self-esteem of the adolescents was negatively correlated (r = –0.30, P < .001; Table 4).
Prevalence of Internet Addiction (IA) Among the Government and Private School Students in Chandigarh (Urban) and Kangra District (Rural), Himachal Pradesh.
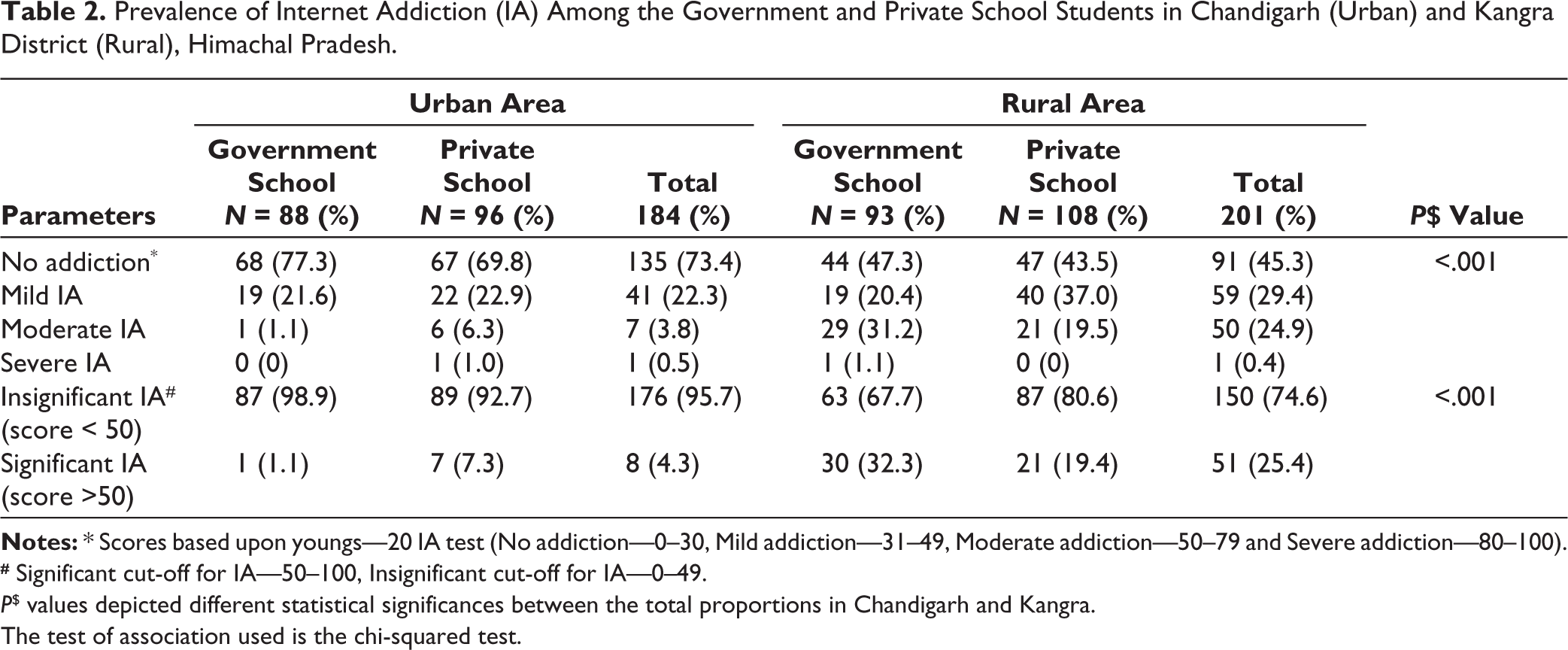
# Significant cut-off for IA—50–100, Insignificant cut-off for IA—0–49.
P$ values depicted different statistical significances between the total proportions in Chandigarh and Kangra.
The test of association used is the chi-squared test.
Association of IA with Depression, Suicidal Ideation, and Self-esteem.
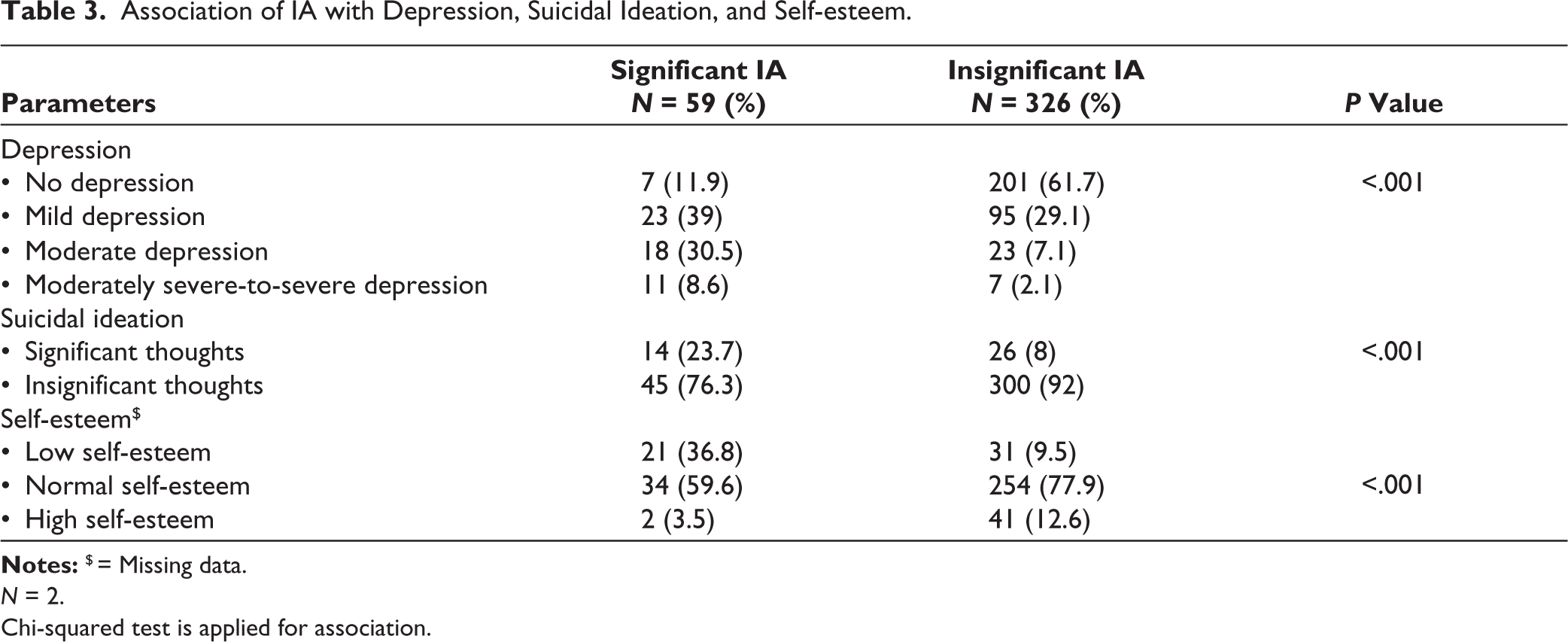
N = 2.
Chi-squared test is applied for association.
Correlation of IA Score with Psychosocial Variables and Age.
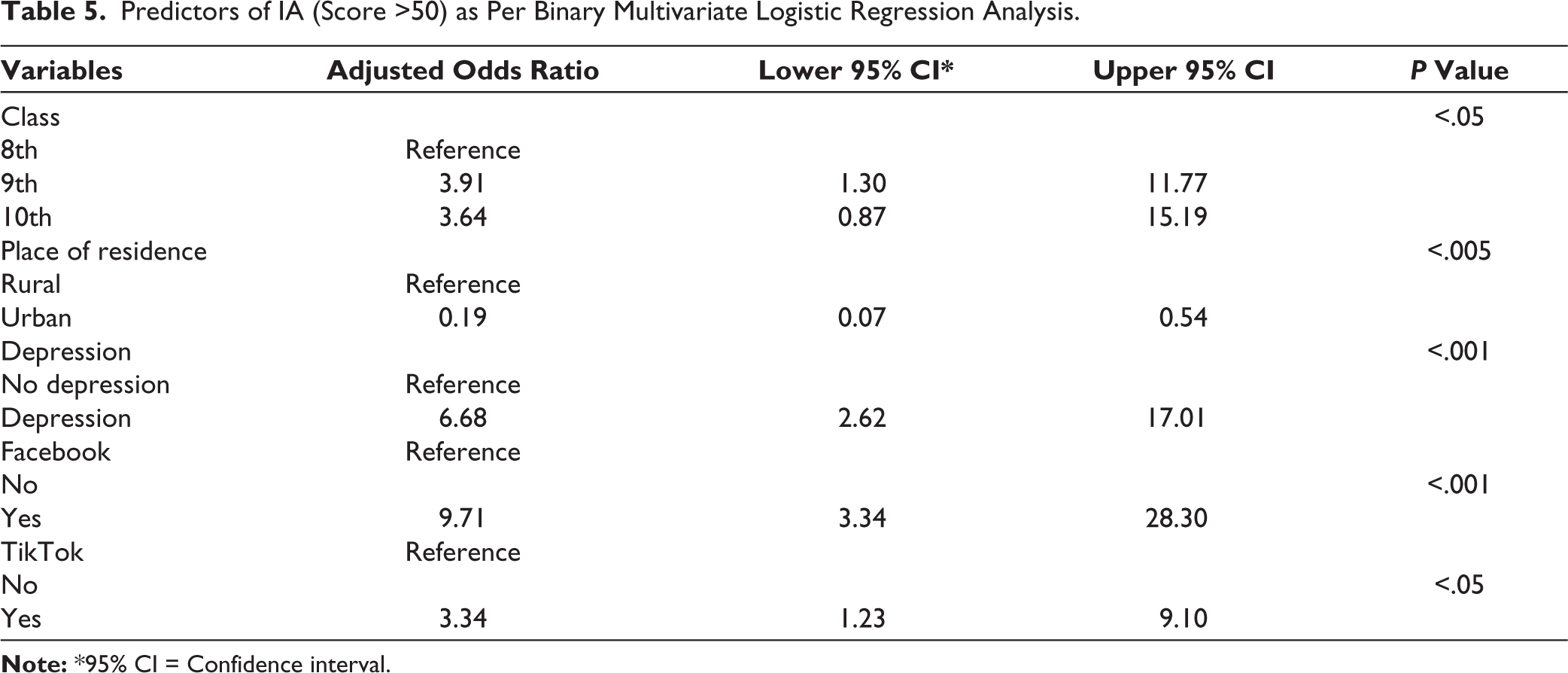
As per the multivariate logistic regression, the significant predictors of IA were adolescents aged 13–15 years studying in grade 9th (aOR = 3.9, 95% CI = 1.30–11.76), 14–18 years old adolescents studying in 10th grade (aOR = 3.6, 95% CI = .87–15.18, P < .05), social media use on Facebook (aOR = 9.7, 95% CI = 3.33–28.29, P < .001) and TikTok (aOR = 3.3, 95% CI = 1.22–9.10, P < .05), and depression (aOR = 6.6, 95% CI = 2.6–17.01, P < .001). Living in an urban area, that is, Chandigarh, was a protective factor for IA (aOR = 0.2, 95% CI = 0.07–0.53, P < .005; Table 5).
Predictors of IA (Score >50) as Per Binary Multivariate Logistic Regression Analysis.
Discussion
To the best of our knowledge, this is one of the first studies that compares the prevalence of significant IA among adolescents living in rural (25.4%) versus urban areas (4.3%) from North India. The study highlighted significant differences in Internet usage patterns, IA, and associated psychosocial outcomes among adolescents in rural and urban areas. The significant predictors of IA were living in a rural area, depression, studying in 9th and 10th classes, and using social media apps like Facebook and TikTok. The mean age of participants aligns with the developmental period where digital engagement peaks, reflecting a growing trend of Internet use for educational and recreational purposes across both settings.
A recent systematic review and meta-analysis that was conducted during the coronavirus disease 2019 (COVID-19) pandemic found that the prevalence of pooled estimate of problematic Internet usage for moderate (21.5% (95% CI: 17%-26.8%) and severe IA (2.6% (95% CI: 1.6%-4.2%) was lower than our study. 11 This can be due to newly introduced guidelines to regulate screen time in specific age groups by the Indian Paediatrics in 2019 24 and the increased focus on screen time after the pandemic. 25 Children aged 18–24 years from Bhutan 26 have a higher prevalence (34.3%) of moderate IA than this study. However, a lower prevalence (8%) of moderate IA was reported among 16–26-year-old adolescents from Bengaluru, India, as compared to this study. 10 These differences could be due to different age groups studied, reflecting other Internet usage behaviors among different age groups. The prevalence of severe IA (1%) in students from Bhutan aged 18–24 years 26 was also found in our study. Chinese students 27 aged 18 years had slightly lower severe IA (0.2%) than our study. These differences might be due to inter-country sociocultural differences among the study participants, which include variability in Internet accessibility, availability of screen time guidelines, and usage behaviors.
Further, living in a rural area was found to be a significant predictor for IA in this study. A study conducted in Poland showed similar results to ours, where problematic Internet usage was more prevalent among rural (28%) students than urban students (22%). 28 This may be due to the easy accessibility and affordability of Internet data in rural areas, which was impossible sometime back in India. Moderate IA was more prevalent in the urban setting (38%) than in the rural locations (28%) in Mangaluru, India, which is in contrast to our study. 5 It might be due to the increased dependency on online shopping, online food delivery, working with electronic media gadgets, and fewer options for playing outdoor games in an urban area than in a rural area.
IA was higher in older children aged >13 years, studying in classes 9th and 10th. Contrasting findings were observed in a study conducted in Turkey that observed a higher prevalence of IA among 9th and 10th graders than 11th graders who were approximately 16 years old. 29 A study conducted in India among 13–18 years students of class 10th to 12th observed that studying in a lower grade, that is, 10th grade was a predictor of IA. 2
Presenting with symptoms of depression was another predictor of IA in our study, similar to the study conducted in 16 years students from Turkey, 29 and 19 years olds from Delhi. 12 The reason could be that students with depressive symptoms also might have low self-esteem as it is a known predictor of IA. 30 There was a positive correlation between IA with suicidal ideation and a negative correlation with self-esteem in this study. Another study conducted among school adolescents in Kerala showed a negative correlation (r = –0.64) of self-esteem with IA. 22 Students with high self-esteem people might have good coping behavior and less dependency or addictive behavior. Similar to our findings, studies from Hong Kong (r = +0.48) 31 have also reported a positive correlation of suicidal ideation with IA.
The IA was positively correlated (r = +0.8) in a study from Bhutan in participants aged 18–24 years, 26 which is similar to our study. However, a negative correlation (r = –0.13) between age and IA was observed among 18- to 30-year-old adolescents from Saudi Arabia. 32 This difference might be due to the older age group included in the study from Saudi Arabia and the restricted participation of only girls. Additionally, the sex of the adolescents was not a predictor of IA in this study. Nevertheless, contrasting results were shown by a study conducted among high school students that observed that boys were more prone to IA. 8 The reason behind this might be boys tend to play online video games that have inappropriate, violent, and nonspecific content, which exposes them to the Internet and elaborative and sensitive information at an early age.
In our study, social networking sites like Facebook and TikTok were significant predictors of IA. Problematic Facebook usage has been by existing literature to have adverse effects on the overall well-being of people 33 Though TikTok has been banned in India now, many studies have shown that TikTok attracted very young users who were more vulnerable to the detrimental effects of social media use 34 In a qualitative study in the United Arab Emirates, parents reported that the content on TikTok was inappropriate, a threat to the safety of users, and had a depressive effect on mental health. 35
This study provided evidence of the IA prevalence and its associates across two different geographical terrains and government and private school students with academically diverse backgrounds. The limitation of the study is that no temporal association could be ascertained between psychological variables and IA. As only one government and one private school were included in the sample, hence the results might not be generalizable.
The public health implications of this study is that IA among adolescents is brought into the limelight in this era of increased Internet usage that might negatively affect the student’s mental health and academic performance. Hence, it is recommended that all the students must be screened for IA and depression, suicidal ideation, and low self-esteem as part of the school health program. The findings emphasize the pressing need for targeted interventions to address IA for adolescent children, particularly in rural areas where the prevalence is higher. There is a need for aggressive campaigning and awareness against all the outcomes of IA and psychological issues. School-based programs promoting digital literacy, parental education on responsible Internet use, and early identification and management of mental health issues could serve as effective strategies. These efforts are critical to fostering healthier digital behaviors and safeguarding the mental well-being of adolescents in the rapidly evolving digital landscape. Further, longitudinal studies should be conducted to ascertain the causal associations of factors associated with IA.
Conclusions
One in every four adolescents (aged ±14 years) living in a rural area (Kangra) had IA as compared to one in twenty adolescents in an urban area (Chandigarh) in North India. Moreover, adolescents studying in higher grades, presenting with symptoms of depression, and using recreational media content like Facebook and TikTok were prone to IA.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee Institute’s Intramural Ethics Committee and Post Graduate Institute of Medical Education and Research, Chandigarh (INT/IEC/2019/001038; dated April 29, 2019). Written consents were taken from all the participants of the study. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.