
Abstract
Background:
Long-term screen exposure negatively impacts children’s physical, psychosocial, and cognitive development. Studies reveal an association between prolonged media exposure, attention deficit hyperactivity disorder-related behaviors, and a heightened risk for the diagnosis. This study investigated the psychosocial and symptomatic impacts of screen time in children with attention deficit hyperactivity disorder.
Methods:
Children aged 6-18 years with attention deficit hyperactivity disorder recruited to the child and adolescent psychiatry outpatient clinic were included (n = 215). A sociodemographic form including information on media usage and the Conners’ Parent Rating Scale were applied. Independent groups were compared using t-tests and analysis of variance, Mann–Whitney U-test, and Kruskal–Wallis H-test. Chi-squared analysis was used for categorical variables, and Spearman correlation was used for quantitative variables.
Results:
Average media exposure was 6.27 ± 2.89 h/day. No significant differences were observed based on gender or attention deficit hyperactivity disorder subtype. Lower maternal education was associated with decreased internet and computer use, whereas television viewing and smartphone use were similar across groups. Daily smartphone use was significantly associated with low paternal education and low academic achievement. A significant relationship was found between oppositional, inattention, and Clinical Global Impression scores and daily smartphone usage. Hyperactivity scores were significantly higher in patients who watched TV for more than 2 h/day. A weak but significant positive correlation was detected between hyperactivity and TV exposure as measured by the Conners’ Parent Rating Scale (r = 0.165). A weak but significant positive correlation was also found between internet/computer use and both restless-impulsive (r = 0.188) and emotional lability scores (r = 0.219). Additionally, total media exposure showed a weak significant correlation with oppositional scores on the Conners’ Parent Rating Scale (r = 0.189). Furthermore, attention deficit hyperactivity disorder-Combined type was significantly associated with longer media exposure.
Conclusions:
Increased media exposure may contribute to attention deficit hyperactivity disorder-related behaviors. Assessing media exposure across diverse sociocultural backgrounds is essential to promote healthier habits and enhancing well-being in children with ADHD.
Introduction
Attention deficit hyperactivity disorder (ADHD) stands among the most common neurobehavioral disorders during childhood and is characterized by persistent symptoms of inattention, hyperactivity, and/or impulsivity. 1 Attention deficit hyperactivity disorder affects approximately 5%-7.2% of children and adolescents and 2.5%-6.7% of adults, with the disorder often considered a lifelong condition due to its persistence into adulthood for many individuals.2,3 Family and twin studies have shown that the development of ADHD is associated with a significant genetic predisposition, but in addition to genetic factors, a wide range of environmental influences play important roles in shaping the symptoms of the disorder. 4 Furthermore, prenatal factors, heavy metal exposure, nutritional deficiencies, and psychosocial stressors have been highlighted for their potential contributions to ADHD symptom severity.5,6
As children are spending increasing amounts of time in the presence of electronic devices, worries regarding the impact of prolonged digital exposure on children’s psychological development have grown. 7 While some studies have advocated for the advantageous effects of digital and social media platforms in facilitating learning, knowledge acquisition, and social interaction, concerns have been raised regarding their potential harm to the social and emotional well-being of children and adolescents. It has been suggested that the increased use of digital devices may interrupt the social and emotional well-being of children and adolescents and may lead to mental health problems.8,9
A recent systematic review indicated a potential association between excessive screen time and both physical and cognitive development, particularly in the area of attentional development in children. 10 Furthermore, a meta-analysis of recent literature revealed a significant correlation between digital media exposure and behavioral problems in childhood. 11 Specifically, data from the CHILD birth cohort study revealed that children who spend more than 2 h/day watching TV exhibit a notable increase in externalizing behaviors, highlighting the potential detrimental impact of excessive screen time on behavioral outcomes. 12 Additionally, exceeding 90 min of daily screen time has been linked to heightened hyperactive behaviors in children under 3 years old. 13 Another recent meta-analysis found that children exposed to more than 2 h of screen time per day had an increased risk of developing ADHD, with an odds ratio (OR) of 1.51 (95% confidence interval [CI], 1.20-1.90). 14 Notably, the content characteristics of contemporary screen media, characterized by violence, stimulation, and rapid pacing, have been implicated in the increase of ADHD diagnoses.15,16 Another meta-analysis identified a small yet statistically significant correlation between media exposure and behaviors associated with ADHD, with an effect size of (r+ = 0.12). 17
The relationship between children’s media usage and ADHD-related behaviors remains a subject of ongoing investigation, with several hypotheses proposed to elucidate the underlying mechanisms. One such hypothesis is the Differential Susceptibility to Media Effects Model, which posits that exposure to digital media can induce three distinct response states: cognitive, emotional, and excitative. 18 According to this model, the content of media can influence children’s response states, which may manifest as emotional reactions, affective reactions, or physiological arousal symptoms resembling ADHD-related behaviors in susceptible individuals.15,18
Another proposed explanation is the arousal-habituation hypothesis, which suggests that exposure to fast-paced media can disrupt attentional shifting and reorienting abilities while increasing arousal levels.17,19 This hypothesis posits that exposure to violent media content in particular can lead to short-term decreases in prosocial behaviors due to desensitization and increases in aggressive behaviors, hostile attitudes, and physiological arousal. Prolonged exposure to violent media may also diminish appropriate emotional responses and contribute to the acquisition of aggressive behavioral patterns through identification with aggressive characters and the attractiveness of a perpetrator’s behavior. 20 Over time, these response patterns may become habitual and manifest as ADHD-like symptoms. 21 Additionally, extended digital exposure during early developmental stages is considered an added risk factor for attentional problems later in development. 22 Collectively, these factors may impede the optimal development of children and exacerbate ADHD-related behaviors.
Children diagnosed with ADHD frequently exhibit deficits in emotional and cognitive self-regulation, along with challenges in inhibitory control. This heightens their risk of prolonged media exposure and subsequent problematic internet use and addiction, as highlighted by a meta-analysis on the subject. 23 Difficulties in regulating and managing their impulses and attention, particularly in the face of digital stimuli, make these individuals more susceptible to excessive media exposure. While every child is at risk for potential overuse, it is vital to determine the underlying or sustaining media-related factors that may influence the onset or severity of symptoms in children and adolescents with ADHD. As such, it is essential to investigate the specific factors of digital media usage that may have an impact on ADHD. Therefore, this research aims to contribute to the existing literature by investigating digital media exposure characteristics and symptom severity in children and adolescents who recently received a diagnosis of ADHD according to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) criteria. Understanding how different aspects of media use impact ADHD symptoms can inform the development of targeted interventions and support strategies for individuals with ADHD and their families.
Materials and Methods
According to a power analysis, a sample size of 179 was sufficient for all estimated parameters if normally distributed with a Type I error of 95% and Type II error of 80%. Considering that most values were nonparametric, we included a 15% error rate to this calculated number and set the sample size for the groups to 215. Ethical approval for the study was obtained. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committees and with the 1964 Declaration of Helsinki. Informed consent forms were obtained from the parents or caregivers of the children taking part in this research.
The study included children and adolescents who presented to the Outpatient Clinic of the Children and Adolescent Psychiatry Department at the Hospital between January and October 2023. All eligible participants were aged 6–18 years, had been diagnosed with ADHD according to the DSM-5 criteria based on a clinical interview, and were treatment-naïve. Exclusion criteria included the presence of any comorbid psychiatric conditions, any organic pathology, and refusal to participate in the research.
All patients who consecutively presented between January and October 2023 and met the inclusion criteria were enrolled in the study. All patients were first evaluated by an experienced child and adolescent psychiatry specialist. Diagnoses were made based on a clinical interview and DSM-5 criteria. Children with any other psychiatric disorders, including oppositional defiant disorder, conduct disorder, or other neurodevelopmental conditions, were excluded from the study. Routine tests, including biochemical parameter measurements and an electrocardiogram, were conducted. If necessary, interventions were initiated in accordance with established clinical guidelines.
Measures
A sociodemographic form developed by the authors was applied. It asked about a participant’s birth history, developmental stages, family structure (nuclear family, divorced parents, and/or single parent), parental educational and employment status, and primary caregiver. Additionally, the presence of domestic violence, academic history, and detailed information about media usage were assessed for the past 6 months to ensure data generalizability. Media usage characteristics were recorded as daily TV viewing, internet/computer use, and smartphone use. Each category was documented separately, and total screen time was calculated. The form was completed primarily by the clinician, who asked parents or caregivers for the necessary information. Afterwards, the participants were interviewed and diagnosed according to the DSM-5-based classification system. The participants were grouped according to digital media usage properties regarding daily TV viewing, internet use, and smartphone usage. After the examination, the necessary treatment, including medical and educational interventions, was started.
Conners’ Parent Rating Scale
The Conners’ Parent Rating Scale (CPRS) is commonly used for parents to identify and monitor the symptom severity of childhood disruptive behavioral problems in children and adolescents aged between 3 and 17 years. The scale includes 80 multiple-choice questions. Its subscales are oppositional, cognitive problems/inattention, hyperactivity, anxious/shy, perfectionism, social problems, psychosomatic, ADHD index, and global index (restless-impulsive and emotional lability). 24 It is a useful instrument for evaluating behavioral problems in children and adolescents. The Turkish validity and reliability study was conducted by Kaner et al. and has been shown to have good internal consistency in the Turkish population. 25
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) Version 22.00 was used for statistical analyses (SPSS Inc., Chicago, IL, USA). The suitability of quantitative variables for normal distribution was examined using the Kolmogorov–Smirnov test. Independent groups were compared using independent samples t-tests and one-way analysis of variance for normally distributed variables. Mann–Whitney U-test and Kruskal–Wallis H-test were used for non-normally distributed variables. The relationships between qualitative variables were investigated using chi-squared tests. Spearman correlation analysis was applied to examine the relationships between quantitative variables, and Bonferroni-adjusted P values were reported. Descriptive statistics of quantitative variables that are suitable for a normal distribution are shown as means ± standard deviations, and descriptive statistics of quantitative variables that are not normally distributed are shown as medians (25th-75th percentile). Descriptive statistics for qualitative variables are expressed as frequencies (%). Statistical significance was determined at P < .05.
Results
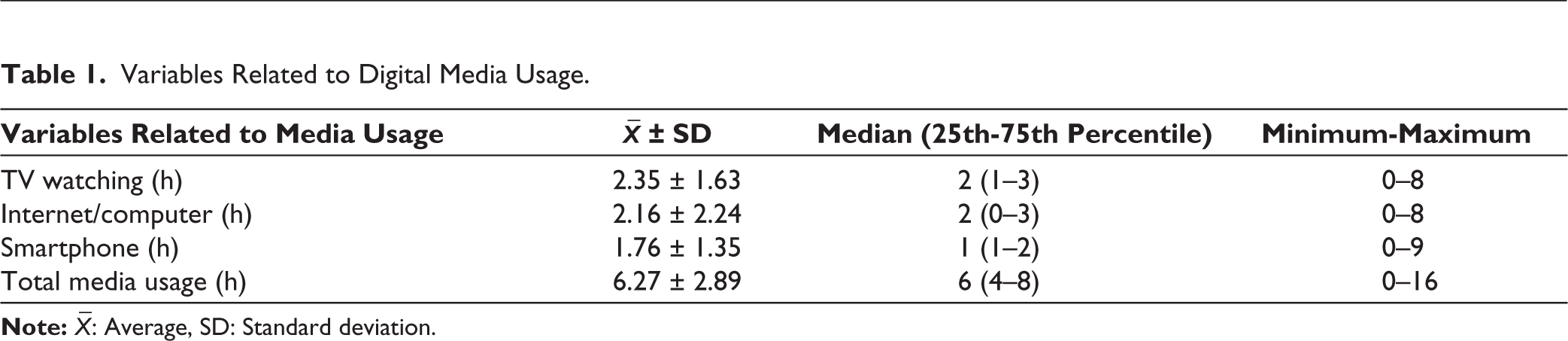
The study involved 215 patients; 88 (40.9%) were female and 127 (59.1%) were male. The mean age of the participants was 12 ± 3.24 years. Variables related to media use are given in Table 1.
Variables Related to Digital Media Usage.
Sociodemographic characteristics were analyzed according to the total time spent viewing media. No significant associations were found between gender, parental education, employment, and family structure (P > .05). However, the rate of intimate partner violence (IPV) was significantly higher among parents of children (19.4%) who used media for ≥8 h compared to 4-6 h (7.1%) and 6-8 h (3.8%) (P = .035).
Using the sociodemographic form, data were collected on daily TV viewing, internet/computer use, and smartphone usage. According to the American Academy of Pediatrics (AAP), media exposure for children aged 6 years or older should be individualized, focusing on a balance between screen time and other essential activities such as physical activity, sleep, and family interactions. Rather than enforcing a strict screen time limit, the AAP emphasizes the importance of this balance. 26 Therefore, in this study, a limit of 2 h/day for TV and computer use, and 1 h/day for smartphone use, was established to ensure a balanced distribution of participants across the two groups.
Patients were divided into two groups according to daily TV viewing time: children who watched TV for less than 2 h/day (n = 129) and more than 2 h/day (n = 86). According to the sociodemographic data, no statistically significant difference was observed between daily TV exposure and gender, parental education, employment status, family structure, and academic achievement (P > .05). However, according to the CPRS, there was a statistically significant difference in hyperactivity and DSM-hyperactivity scores between the groups that watched TV for ≤ 2 h and >2 h (P < .05).
Patients were divided into two groups according to daily internet/computer exposure time. The number of children who spent less than 2 h/day on the computer was n = 138, whereas n = 77 children were exposed to a computer more than 2 h/day. No significant difference was detected in terms of gender, maternal employment, paternal education and employment status, and family structure. No significant associations were observed in relation to most sociodemographic variables, except that children with mothers who were primary school graduates were more likely to spend less than 2 h on the computer daily (50.7% and 33.8%, respectively, P = .035). No significant differences were detected between measure scores for these children in any setting.
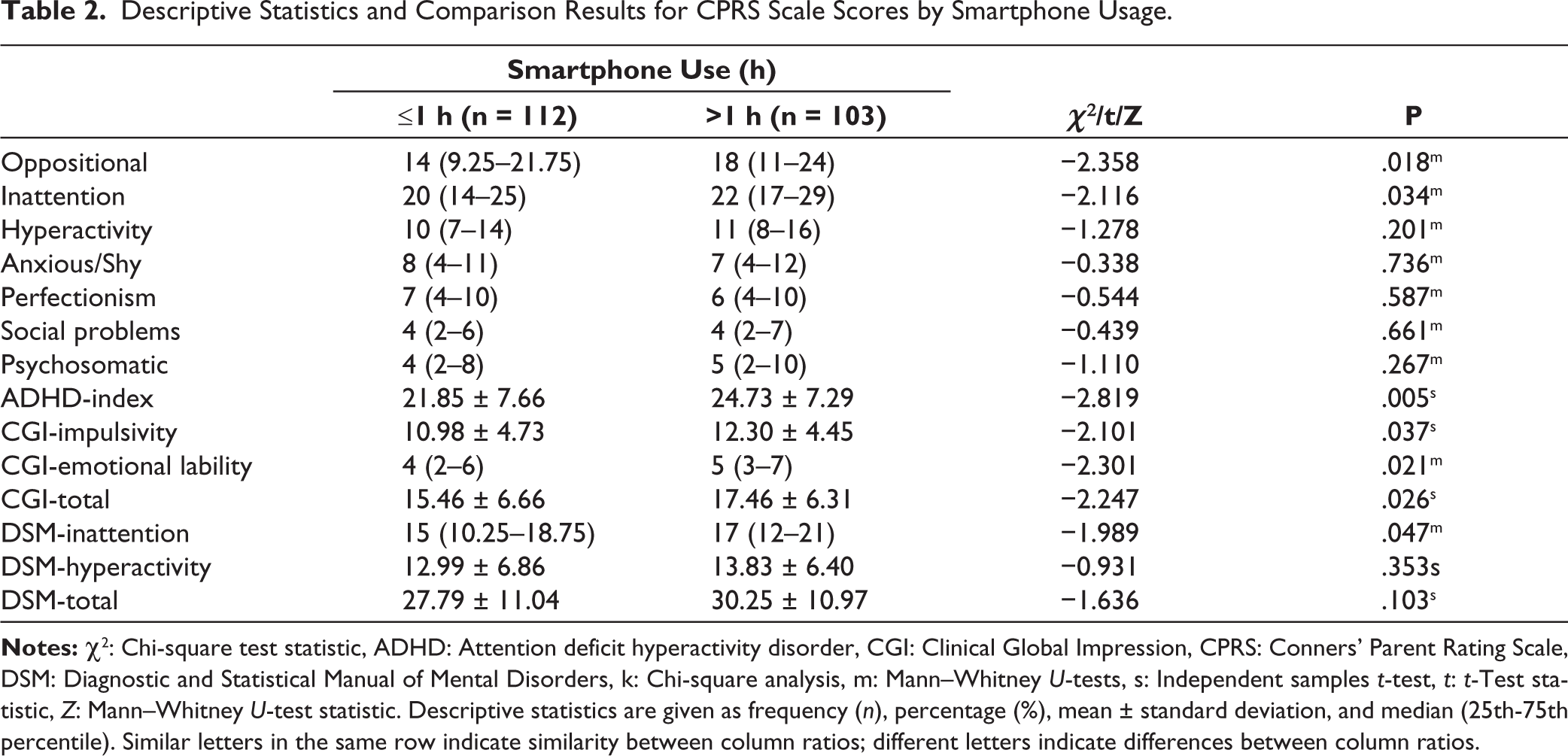
Children were divided into two groups according to daily smartphone usage; n = 112 children reported less than 1 h/day of exposure, whereas n = 103 children reported more than 1 h/day of usage. No significant differences were detected regarding gender, maternal educational and employment status, paternal employment, and family structure (P > .05). However, the rate of having a college graduate father (17.9%) was significantly higher among children who used a smartphone less than 1 h/day. Descriptive statistics and comparison results regarding CPRS scale scores according to smartphone usage time are given in Table 2.
Descriptive Statistics and Comparison Results for CPRS Scale Scores by Smartphone Usage.
Two correlation analyses were conducted for TV viewing time, three for internet usage time, five for phone usage time, and three for media usage time. Following the initial analysis, the original P values were replaced with Bonferroni-corrected P values (Padj). Findings regarding the correlation analysis between the times spent on TV, internet/computer, smartphone, and media and scale scores are given below:
There is a weak positive relationship between TV viewing time and hyperactivity (HA) and DSM-HA (r = 0.165, Padj = .030; r = 0.192, Padj = .010) by CPRS.
There is a weak positive relationship between the duration of internet/computer use and Clinical Global Impression (CGI)-Restless-impulsive, CGI-Emotional Lability (r = 0.188, Padj = .027; r = 0.219, Padj = .006) by CPRS.
There is no significant correlation between smartphone usage time and oppositional, ADHD-Index, CGI-Restless-impulsive, CGI-Emotional Lability, and CGI-Total scores by CPRS (r = 0.175, Padj = .050; r = 0.158, Padj = .105; r = 0.158, Padj = .100; r = 0.144, Padj = .170; r = 0.170, Padj = .060).
There is a weak positive relationship between media usage time and oppositional (r = 0.189, Padj = .018) scores, but no significant correlation with hyperactivity by CPRS (r = 0.136, Padj = .138).
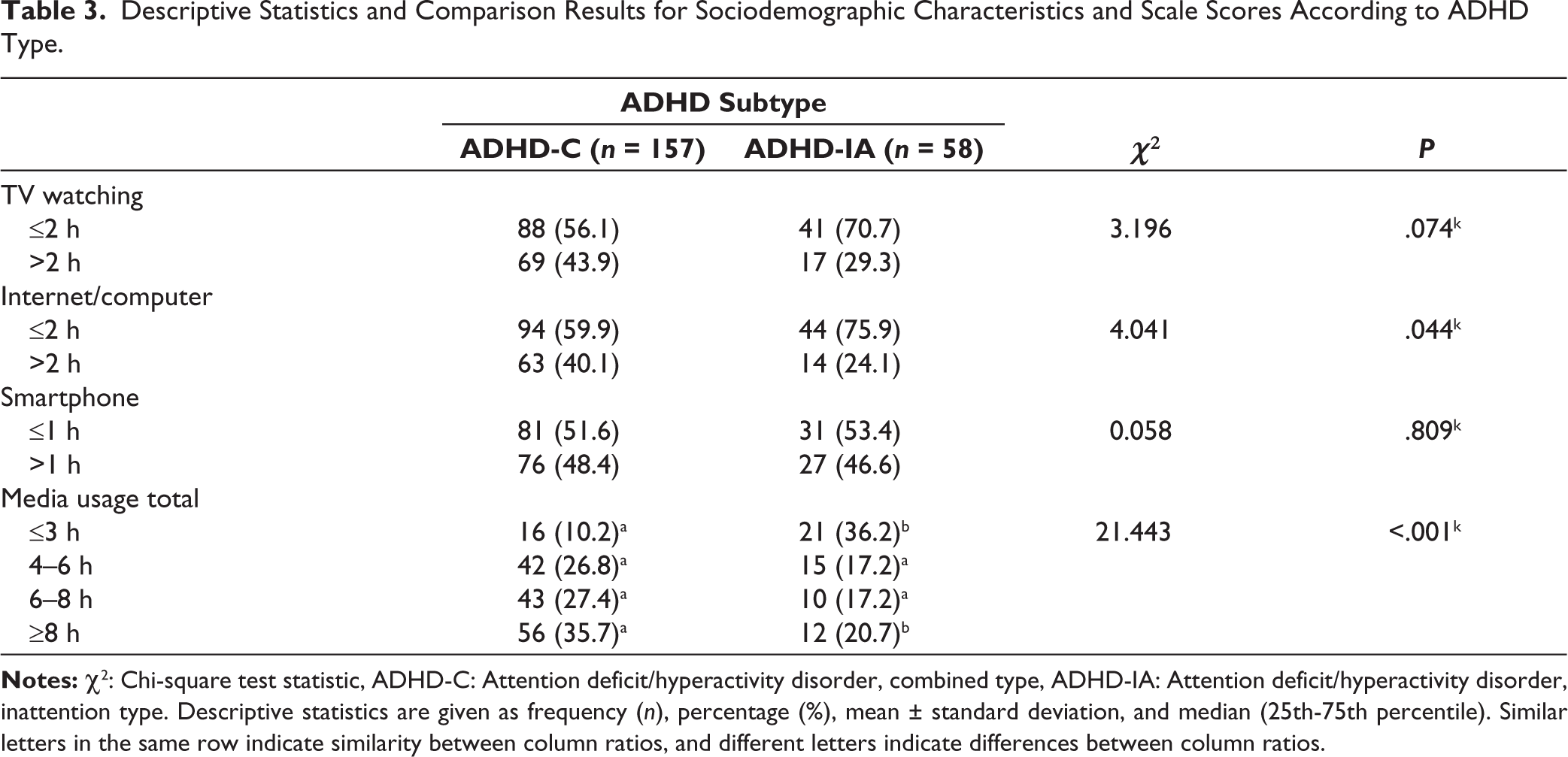
Descriptive statistics and comparison results regarding sociodemographic characteristics and scale scores according to ADHD type are given in Table 3.
Descriptive Statistics and Comparison Results for Sociodemographic Characteristics and Scale Scores According to ADHD Type.
Discussion
The increasing prevalence of digital media usage among children and adolescents has been well-documented in the literature. 27 A recent systematic review revealed that school-aged children spend an average of 2.77 h/day on digital media, with nearly half exceeding 2 h daily. 28 The literature indicates that children with ADHD have higher levels of screen exposure compared to their typically developing peers. It has been reported that over 80% of children with ADHD exceed the recommended screen time limits. 29 In our study, the average time spent with digital media was 6.7 ± 2.9 h/day. Notably, our results align with existing trends in the literature, indicating heightened digital media usage among children and adolescents recently diagnosed with ADHD.
Children’s and adolescents’ exposure to media is influenced by several environmental factors. It has been suggested that various social and physical elements within the household environment can influence family media habits. Among those, studies have demonstrated an inverse relationship between maternal educational level and children’s television viewing.30,31 Lower maternal education is associated with a child having a television in their bedroom and decreased parental concern about children’s screen time, particularly in school-aged children.22,30,31 Since maternal educational level is frequently used as an indicator of family socioeconomic status, the observed association between lower computer and internet usage may reflect limited access to necessary devices in these households. Consequently, these results may be applicable to families experiencing different types of disadvantages. Mothers with lower levels of education might be parenting their children in socially disadvantaged environments and using digital media as a free recreational activity. Furthermore, they might have less access to educational resources or community support. 30 On the other hand, paternal education level is associated with better screen time management among children. 32 The significant correlation between higher paternal educational level and reduced smartphone usage in children and adolescents, supports previous research, as higher educated parents may often be more aware of the potential risks of excessive screen time and may be better able to set guidelines or limits for their children’s media use, particularly following educational interventions by clinicians.32,33 Therefore, our results suggest that screen habits may vary across different socioeconomic backgrounds, and warrant further assessment. 34
In our study, another factor that may have influenced the duration of screen exposure was IPV. The connection between IPV and prolonged media exposure may reflect higher parenting stress and reduced child–parent interactions, leading to impaired family functioning. 35 Extended screen time in this context may be viewed as an extension of neglect or maltreatment. Dysfunctional parenting practices may result in diminished control over media use, which can increase the risk of oppositional behaviors, particularly in children with lower self-control. 22
Conversely, living with a child with ADHD may be distressing. Their inability to adhere to rules, impulsivity, and oppositional behaviors are linked to increased parental stress and family conflict, which may make it more challenging for these parents to implement effective strategies for managing their children’s digital media use. 36 The literature has noted that in families with children with ADHD, lower levels of connection and decreased affective responsiveness, warmth, and involvement from parents may affect the quality of relationships with their children. 37 Therefore, poor communication between parents and children may contribute to excessive media exposure. In some cases, parents may use digital media to control their children’s behaviors, which can lead to a repeating cycle of problems.
In the literature, there are insufficient data on the effects of subtypes of ADHD on digital media usage characteristics. Our findings suggest that children with ADHD-Combined type (ADHD-C) watch TV and play on the internet longer, which are associated with prolonged total screen time compared to children with the ADHD-Inattentive type. Moreover, as media time increases, hyperactivity and opposition scores are reported to be higher both by parents and teachers. A recent study demonstrated that children who are exposed to screens for 2 h a day have a heightened risk of having inattention and hyperactivity symptoms and an increased risk of having an ADHD diagnosis. 12 Although the underlying mechanism is not fully clarified, children with hyperactivity symptoms may struggle with impulse control, leading them to seek more stimulating media, such as fast-paced video games, which offer excitement and immediate gratification. Furthermore, challenges with self-regulation and impulsivity can result in prolonged media exposure. Our study suggests a trend by presenting an association between TV viewing and total media time and hyperactivity symptoms.
Beyond the subtypes, symptom severity could be another parameter that may predict overall media exposure. Research indicates that individuals with higher symptomatology are associated with an increased risk of developing an addiction. 38 Higher levels of inattention have been linked to an increased likelihood of smartphone addiction in younger adults, as suggested by our study. 39 Individuals experiencing greater difficulties with attention may be more susceptible to problematic smartphone use and other forms of digital media addiction.
A prospective cohort study demonstrated that, although rarely studied, higher screen time is associated with a higher prevalence of disruptive behaviors, including oppositional defiant disorder and conduct disorder, especially when screen time exceeds 4 h/day. 40 Although patients diagnosed with oppositional defiant disorder and conduct disorder were not included in our study, our findings suggest a trend in symptom patterns in disruptive behaviors. Maladaptive parenting, inconsistent discipline, and difficulties in following the rules, which are frequently seen in children with oppositional defiant disorder symptoms, may result in the risk of prolonged screen exposure. 41 Moreover, it has been observed that oppositional traits strongly impact family functioning and may have an indirect effect on digital media characteristics. 42 As our study shows, children with higher emotional lability are associated with increased smartphone usage, aligning with findings in the existing literature. Children with an initially higher symptomatology may be at risk of developing an addiction to media and may present with longer digital exposure before receiving treatment.
In conclusion, existing research highlights a significant association between excessive digital media usage and ADHD-like behaviors in children and adolescents. Given that individuals diagnosed with ADHD are particularly vulnerable to problematic media use, it is crucial to examine various factors that may contribute to prolonged exposure to screens. This includes considering ADHD subtype, parental education level, experiences of IPV, and overall family functioning. Efforts to promote healthy media usage practices and mitigate potential negative effects on children’s well-being are warranted, with further research needed to elucidate the nuanced interplay between media exposure and ADHD-related behaviors.
The study has some potential limitations. The research mainly focused on children and adolescents with ADHD, potentially limiting the generalizability of the findings to all children with ADHD. The broad age range of children included in the study may necessitate caution in generalizing findings regarding the variability in media usage and ADHD symptomatology. The absence of a control group limited the ability to determine whether the observed usage patterns are specific to ADHD or part of broader behavioral trends. Conducting the research in a single center may have limited the diversity and representativeness of the sample. The study includes self-reported data, which may have been subject to recall bias or social desirability bias, potentially leading to inaccuracies in the reporting of symptoms. Although data on educational and employment status were collected, additional information on broader family dynamics and lifestyle factors that may influence media usage habits should also be considered. The absence of specific scales or measures to assess smartphone usage or internet addiction could have limited the study’s ability to comprehensively capture and analyze media usage characteristics among children with ADHD. Finally, the study did not account for the potential effects of various treatment plans, including medical and psychosocial interventions, on media usage patterns among children with ADHD. Longitudinal studies are needed to clarify the direction of the relationship and gain a better understanding of the connection between ADHD and media exposure.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was approved by the Ethics Committee of Adana State Training and Research Hospital (Process No.: 04.01.2024/143). Written informed consent was obtained from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.