
Abstract
Introduction:
With a rising number of children being placed in childcare institutes across the country, the delivery of adequate socioemotional care has become imperative. The role of caregivers in such institutions is pivotal in ensuring the well-being of the children yet little is known about their current capacity and practice with respect to providing psychological care. This study aims to develop and validate knowledge, attitudes, and practice scale for caretakers in childcare institutes.
Material and Methods:
A cross-sectional design was used to develop and validate the scale through three phases (a) the first phase (qualitative phase) was a comprehensive review of literature for item generation; (b) the second phase (quantitative phase) con- sisted of establishing content validity (item reduction) by seven experts in the field of child and adolescent mental health rating each item on suitability, relevance, and acceptability; (c) the third phase entailed translation of the questionnaire in the regional language.
Results:
In an initial item generation of 60 items, resulting in a final pool of 40 items validated by experts, satisfactory content validity index was (CVI > 0.79).
Conclusion:
This scale can be used to assess caretakers in institutional homes for children in the Indian context. The gaps identified in the knowledge of the caregivers by this assessment can be utilized in developing a robust training module and intervention for caretakers.
I ntroduction
India houses one of the largest populations of children in the world, 1 with 1.8 lakh children in institutional care 2 and holds the responsibility of ensuring the care and protection of children through its cross-cutting policies and programs. The Juvenile Justice Act of 2015 is a policy developed for the protection, care, and rehabilitation of neglected and vulnerable children, paving the way for reform of institutional homes in India. According to the Ministry of Women and Child Development, 2 children are usually admitted into childcare institutes (CCIs) because they are orphans, abandoned, runaway, sexually abused, subjected to child pornography, rescued from labor, had a physical or intellectual disability, and affected by human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). The functioning of CCIs is critical in the development of these children, primarily, for their rehabilitation and re-integration into society. However, the viability of institutionalization has been debated due to its long-lasting impact on the developmental trajectory of children.3,4 Dozier and colleagues 5 work shows that institutions have common features such as “high child- to-caregiver ratios; caregivers with low wages and little education or training who work rotating shifts; regimented and nonindividualized care; and a lack of psychological investment in the children.” In a country like India when there are so many complex sociodemographic factors at play and where institutional care may be the only setting available for a child, the role of quality caregiving is imperative.
There is compelling evidence to establish that children placed in institutional homes lack a nurturing and conducive environment for development. 2 The common practice of a regimental system in CCIs prevents caretakers from providing individualized care for children. 6 Effects in physical growth, cognitive development and psychosocial health seem most pronounced when children have least access to individualized caregiving, and when deprivation coincides with early developmental sensitive periods. 4 Thus, it becomes imperative to assess the current capacity of caretakers to provide such care. From an Indian context, it needs to be highlighted that children in CCIs often suffer from structural neglect in terms of minimal human resources, fluctuating staffing patterns as well and inadequate socioemotional care. The estimated ratio of caregiver-child ratio is 1:8 which is only fulfilled across 40% of the CCIs across the country driving a gap in the delivery of effective and accessible care in institutional homes. 2 In previous studies with children in institutional care, it is seen that although children enjoyed the basic necessities of life, that is, food and shelter, they battled psychological turmoil, had poor social cognition, 7 poor resilience, 8 and were more vulnerable to emotional and behavioral problems (poor peer relationships, sadness, and disruptive behavior).9,10 Caretakers become a critical factor in facilitating the social integration of these children with consistency and support, essentially acting as “transition guides.” 11 A comprehensive understanding of the existing knowledge, attitudes and current practices (KAP) of the caretakers is the first step to inform about the upskilling or improving the capacity of this workforce. In order to enhance institutional care, it is important to understand the nature of caregiving environment through caretakers’ knowledge, beliefs, and practice. 12 Currently, there is no widely disseminated, validated tool for measuring such knowledge, attitudes, and practices of caregivers in childcare institutes in Indian context. Such tool can provide insight into the current landscape of caregiving which can guide us further in developing capacity-building programs based on their needs.
The process of development and validation of such a scale is essential to exhibit good psychometric properties, in terms of drawing replicable results as well as establishing a concrete conceptual framework. Content validity is an important criterion for measuring validity as it broadly ensures a thorough internal structure and effective writing of items based on expert judgment. 13
With this objective, this study was carried out to develop and validate the KAP scale for caretakers in childcare institutes in Delhi, India. Currently, there is no validated instrument for assessing immediate caretakers’ knowledge, attitude, and practices about psychosocial aspects of caring that is available in India to the best of the researchers’ knowledge. We also attempted to do content and face validate this tool as well as translate it into the local language for ease.
Materials and Methods
Study Design and Setting
This study was conducted across five districts of Delhi from July 2023 to September 2023 and consisted of a development phase and validation phase. This study is a part of the larger project aimed at developing training manual for caretakers funded by ICSSR and ethics approval was granted by the institutional ethics committee (Proposal no: 180/2022-2023/ICSSR/RP/MN/GEN) and all methods were performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants.
Participants
Caretakers who are the key stakeholders in taking care of children first and direct contact. For ease of understanding, the caretaker is defined as a housefather/house mother/housekeeper/house aunty deputed in CCIs full-time and part-time based on their duties and roles. Mostly all the caretakers are involved in maintaining discipline, hygiene, daily routine, looking after their safety, and escorting children. 14
Development and Validation of the KAP Questionnaire
It was an observational, descriptive study with a cross-sectional design to develop and validate the
Phase I
Step 1: Conceptualization and Identification of Domains and Sub-domains for Caretakers’ KAP Tool
For conceptualizing domains to develop initial pool of items, two round table discussions were held among experts who are the critical stakeholders in children’s welfare. To assess the existing landscape of caregiving, a small convenience sample of 14 volunteers from target population of welfare officers, counsellors, superintendent, CWC (Child Welfare Committee members), officials from WCD (Department of Women and Child Development) in various parts of Delhi was taken. These members are in supervisory roles and are apprised by the issues related to caregivers as well as children.
The objective of these round table discussions was to understand the challenges and concerns related to childcare with respect to caretakers and elicit best practices to inform skill-training for caretakers in the future. The discussions explored the knowledge of early psychosocial development, mental health concerns and legalities involved with institutionalized children among caregivers. Additionally, the perceptions and beliefs that are prevalent among caregivers regarding children in institutional care were explored. Lastly, caregivers’ practice of sensitized caregiving and other parenting practices were discussed.
Step 2: A Literature Review to Identify Domains and Sub-domains and Generate a Preliminary Item Pool for the Tool
Using a deductive approach, an extensive literature review was carried out to analyze the existing evidence on caretakers and caregiving of institutionalized children. The literature review was done by the researchers from April to June 2023. Different databases (such as PubMed, Science Direct, Scopus, Google Scholar, Web of Science) were used. The terms that have been used for searching were caregivers, caretakers, vulnerable children, childcare home/s, institutional care and knowledge, attitude, and practice from the Indian context. There were 10 selected full-length, peer-reviewed articles with first-hand accounts of caregiving in institutional setup in India which were considered for the study.
The field notes from the round table discussions and findings from the review of literature were subsequently analyzed to derive the domains and sub-domains of the KAP tool.
Knowledge was based on concepts of early development, childhood mental health concerns, and legal aspects of children in institutional care. Attitude was defined as the set of perception and beliefs that the caregivers hold towards the children in institutional care and whether they were positive or negative. Lastly, practice was based on parenting practices such as use of corporal punishment, structured routines, managing crisis, and offering affection to children.
Step 3: Developing the Structure of the Questionnaire Through Expert Review
The initial pool of 60 items was reviewed by experts and the number of items was reduced to 42. This set of identified items was organized into the form of a questionnaire. These 42 items were selected after the discussion with the two subject experts based on agreement, suggestion, language, format, and response system.
Phase II
Establishing Face and Content Validity and Estimation of Agreement Coefficients
Face validity is the lowest level of validity and represents the assumption of an expert and acceptance that a test represents the domain being assessed. After the preparation of the first draft, the questionnaire was reviewed by experts in the field and caregivers of children in CCIs for face validity by assessing the readability and clarity of the language used in the items. It was seen that the items were generally easy to answer.
The content validity of the tool “Knowledge, Attitude, and Practice Scale” for caregivers providing individualized care for children (CKAP-CCI) followed a step-wise process. The researcher prepared the content validation proforma for the subject matter experts to validate the items systematically and comprehensively. The experts evaluated each item on three components. The rating protocol was designed in the form of the following domains:
Relevance: Each item was rated on a Likert scale of 1 [not relevant], 2 [somewhat relevant], 3 [quite relevant] and 4 [highly relevant]. Suitability: Each item was rated dichotomously as 1 [agree] and 2 [disagree] Acceptability: Each item was rated on a Likert scale of 1 [completely acceptable and selection of item], 2 [requires modification] and 3 [not acceptable and elimination of item].
15
In this study, seven subject matter experts were selected through convenience sampling after their consent was sought. All the subject matter experts were actively working with the child and adolescent population across various domains of mental health fields like psychology, social work, and child psychiatry. They were requested to check grammar, phrasing, item allocation, and scaling in terms of the qualitative content validity of the scale. The experts were encouraged to provide written comments to improve the relevance of items to the targeted domain. The idea behind receiving feedback on various components was to provide more freedom to experts to judge and strengthen the validation process. All comments were then taken into consideration to refine the domains of KAP and its items.
Phase III
Translation and Back Translation of the Tool in Hindi
The standard translation procedure 16 was followed using a series of steps. The first step involved translation from the original language (English) to the target language (Hindi) by two independent translators. The identification of any terms, words, or phrases that may need to be modified according to cultural context and meaning was done. The independent translators were bilingual and experts in mental health to understand the nuances of the target language as well as the concerned population. Both the translators were aware of the concepts the questionnaire intended to measure to provide a translation which closely resembled the original instrument. Discrepancies between the translators were discussed and resolved.
After this, the initial translation was independently back translated to ensure the accuracy of the translation. This was also done by two independent translators. Researchers who were familiar with the construct and developed the original questionnaire and the forward and backward translators reviewed all the versions of the translations and determined whether the translated and original versions achieved semantic and conceptual equivalence. Discrepancies were resolved and the group reached a consensus on all items to produce a prefinal version of the translated tool.
Lastly, to ensure that the question reflects the intended underlying construct and is well accepted by the concerned caretakers’ cognitive interviews were done using a small sample. This process is one of the most crucial steps, as it helps in determining whether the items developed by the researcher are understandable to the respondents and whether they answer in the fashion intended by the researcher. 17 In this study, the researcher conducted cognitive interviews with five participants. Based on their experiences, seven items were modified concerning the language and understanding of the items.
Measures
We chose indices of validity to validate the KAP tool.
Content Validity Indices (CVI)
A CVR was calculated for each item. Items were eliminated possibly occurring due to chance of using a table of critical values found in Ayre and Scally. 18 Alternatively, Polit et al 19 suggest items with a CVR of 0.78 or higher with three or more experts could be considered evidence of good content validity. If an item does not reach this threshold, it is deleted from the final instrument. The CVR tells us about the validity of individual items. The CVR is a useful statistical technique to determine the validity of individual instrument items, as rated by a panel of content experts.
Results
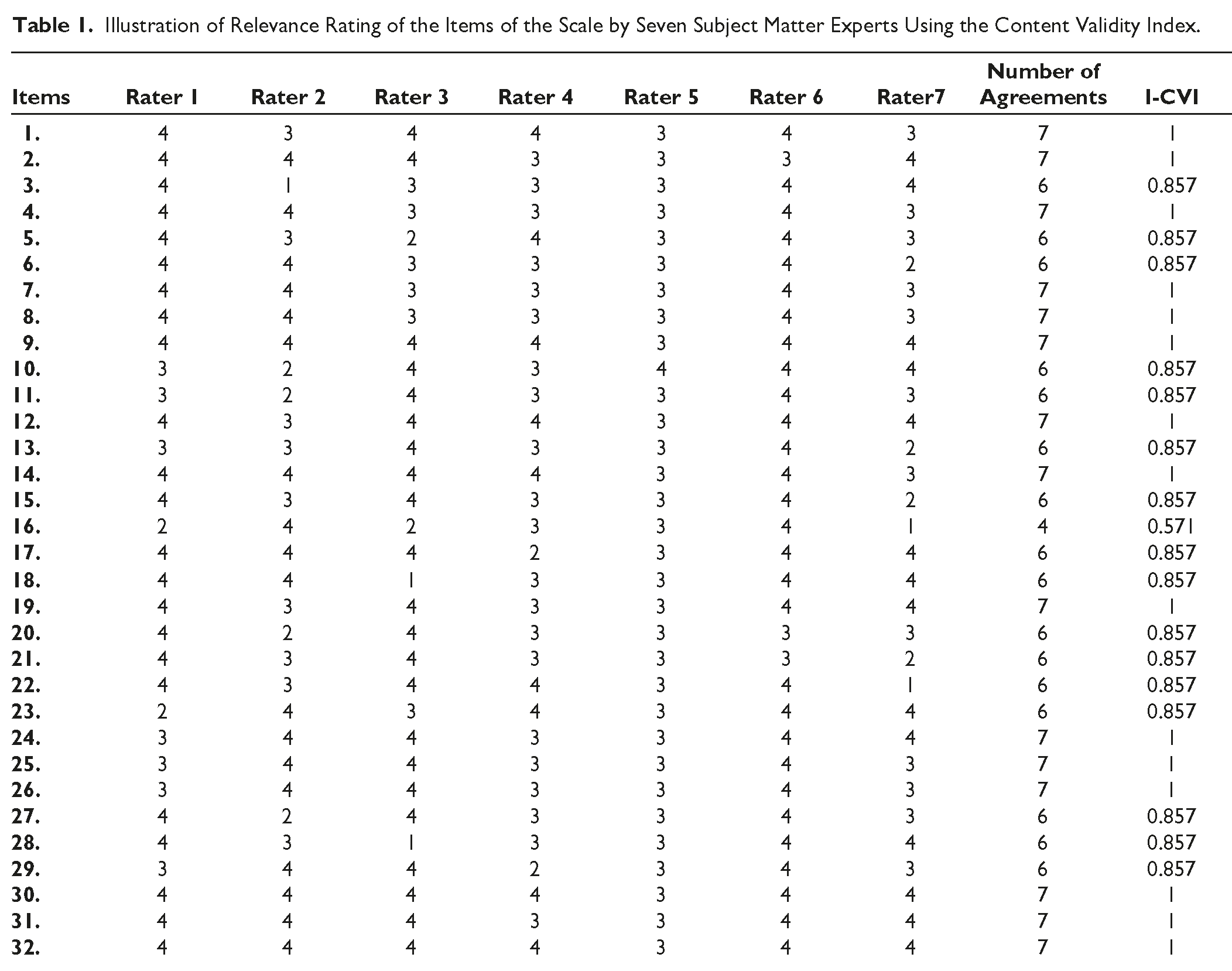
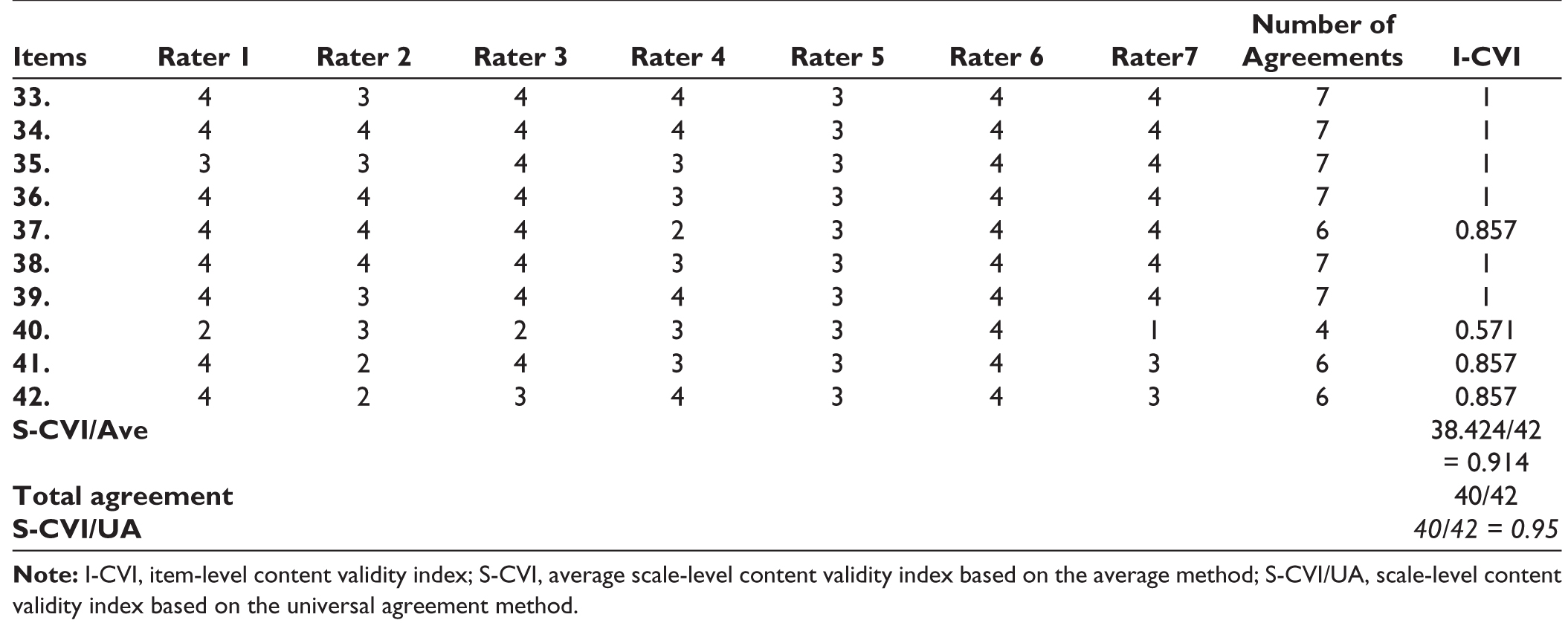
Table 1 shows the I-CVI and S-CVI/Ave for each of the components of content validity. In the quantitative phase, the content validity index (CVI) and content validity ratio (CVR) of the tool were assessed for each item. The CVI was assessed by asking the experts to rate each item according to its simplicity, relevance and clarity 2 on a scale from 1 = not relevant, 2 = somewhat relevant 3 = quite relevant and 4 = highly relevant and suitability (agree or disagree). For the newly developed scale, the CVI was measured as the proportion of items on the questionnaire that achieved a rating of 3 or 4.15,20 Researchers have stated that a score of 0.9 is considered excellent, and 0.8 is considered appropriate.15,21 Based on the above considerations, two items were removed (due to CVR and CVI of lower than 0.64 and 0.8), and the items of KAP were reduced to 40 items. A CVI score of 0.79 or above for each item was acceptable. Researchers recommend that a scale with excellent content validity should be composed of I-CVIs of 0.78 or higher and S-CVI/UA and S-CVI/Ave of 0.8 and 0.9 or higher, respectively.15,21,22 After the content validity, two items were removed from the newly developed scale, namely, items no 16 and 40.
Illustration of Relevance Rating of the Items of the Scale by Seven Subject Matter Experts Using the Content Validity Index.
Flowchart of the Development and Validity of the Knowledge, Attitude, and Practice (KAP) Questionnaire.
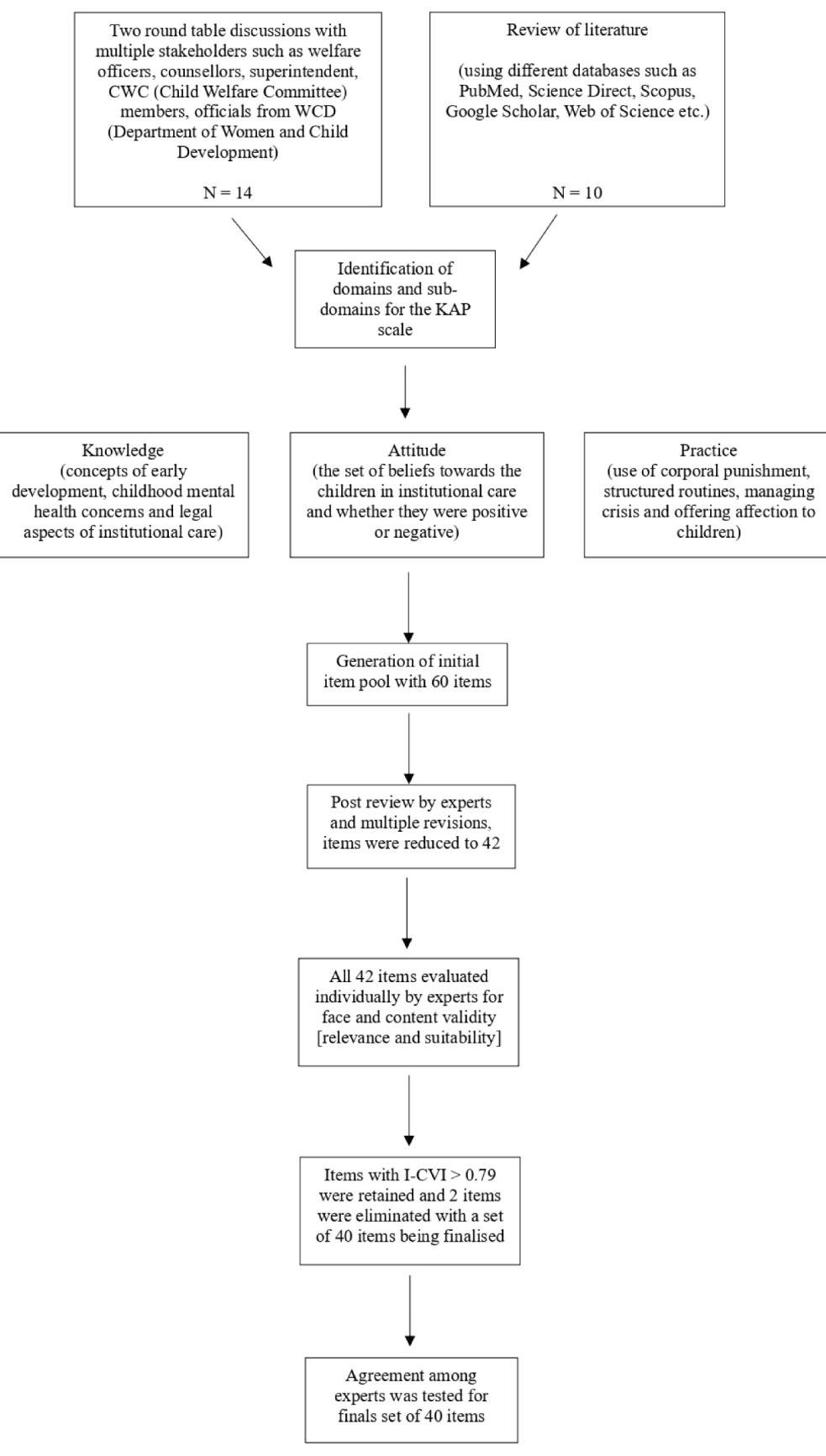
The final KAP has 40 items with 15 items in the Knowledge domain, 16 items in the Attitude domain and 9 in the Practice domain and the response section designed to have a Likert scale of 1 [agree], 2 [neutral] and 3 [disagree] (Appendix 1)
Discussion
The caregiver’s perspective in understanding the integral functioning of childcare institutes and their improvement has been proved useful in studies conducted in other countries.23,24 Due to poverty, lack of access to education, and other necessities, children in care have better opportunities for their future than living with their biological parents. 25 Thus, it becomes pertinent that children grow in a supportive and encouraging environment. Caregivers, having first-hand interaction with the children regularly, influence the well-being and adjustment of the children in a pivotal manner. However, the existing literature suggests that most of the children placed in institutional care have negative experiences and consequent negative impact on their development. 26 In lower- and middle-income countries where institutional care becomes the only alternate care for children without parental care, it is vital to make best use of institutional care systems by transforming its living conditions. Children in care not only require basic needs fulfillment but also the emotional and psychological problems need to be addressed with care. The few existing studies indicate that these caregivers rarely have specialized qualifications in childcare and face extremely poor working conditions.27,28 Generally, they report a high workload and stress level.28,29 A study done by the government body in India revealed that many childcare institutions are overcrowded or with shortage of staff and the strength of children are not proportionate to the capacity of childcare institutions. 30 Previous studies conducted in India with childcare institutes have seldom integrated the caretakers’ perspective into the understanding of vulnerable children. 25 Very little is known about the caretakers that play a vital role in childcare institutions. It is necessary to understand the challenges faced by caretakers, and their suggestions of ways to improve the quality of care in children’s homes. 25 To build any specific intervention program to upskill the caretakers and build their capacities, it becomes necessary to assess the existing knowledge of the caretakers. The overarching research question of this study was the felt need of the caregivers which is likely to influence behavior and practice in the field of childcare. This study fulfills the goal of creating an organized medium to measure the capacity and knowledge of caretakers in childcare institutes. It bridges the gap in the understanding of caretakers’ understanding of providing psychosocial care, highlighting specific areas of care in caring for vulnerable and separated children.
This study developed and validated a KAP questionnaire survey that can be administered among caretakers in childcare institutes. The content of the questionnaire was curated through a thorough review of literature and discussion among mental health experts to ensure suitability and coverage. Further, the tool was scientifically validated by the calculation of content validity indices. The assessment of content validity is a critical and complex step in the development process of instruments. It describes the required elements of the content for the instrument and is not related to the scores obtained from that construct. According to Lawshe, 15 content evaluation of a tool is done by experts in the domain who rate each of the items as “necessary,” “useful,” or “not necessary.” For this study, a panel of seven subject matter experts was collated to rate the items on the Lawshe content validation criterion. The final set of 40 items had satisfactory content validity indices (CVI > 0.79). Additionally, the final questionnaire was evaluated through cognitive interviewing with five participants to determine whether the items were eliciting the intended underlying construct. The tool largely covers psychosocial aspects of caregiving and what must be the expected level of knowledge, attitudes, and practice adopted by the caretakers to address the evolving needs of the children.
Despite contradictory evidence, the practice of institu tionalization continues to remain a reality across the globe. The prospects of institutional care need to be improved with developmentally informed and psychosocial practice within the homes. The development of a validated KAP will function as an essential assessment to identify existing gaps in the knowledge of the caregivers and construct appropriate interventions to bridge these gaps. The developed and validated KAP questionnaire survey is useful in identifying the existing gap in knowledge among caregivers of children in CCIs. Policymakers can also be informed about the capacity building needs and what the skills that these caretakers require while taking care of children in homes.
The findings can be implemented in developing a comprehensive training module that addresses psychological needs and enhances practice that promotes psychosocial care. This study is not free from limitations. The initial knowledge gathering about the caretakers was done from important stakeholders in the system, but not directly from the caretakers. The premise was set with their understanding of the felt need for skill building as viewed by others. However, the cognitive interviewing at the end of the designing of the tool provided reasonable feedback which was in line with the initial premise. The strength of the study is the expertise of the various professionals in the validation process of the tool.
A previous study emphasizing the need for caregivers to receive appropriate training and skill development revealed that none of the caregivers employed at the childcare facility possessed any specialized qualifications in early childhood education. Furthermore, the eligibility criteria for hiring caregivers did not include such qualifications. 25 Hence, the development of the scale is a step towards mapping existing knowledge, attitude, and practices to develop such trainings. The KAP items largely fulfil the gap in understanding child development, familiarity with early childhood principles and practices, policies, and regulations. Caregiver beliefs and values may influence practices and quality of interaction with children.
This can guide us in the direction of factors influencing KAP such as training and education, supervision and support, working conditions, and cultural context which can help devise trainings to build capacities and answer some of these concerns of the caretakers to function competently.
Strengths and Limitations of Study
The strength of the study is the expertise of the various professionals working in child and adolescent area in the validation process of the tool. The study is not free from limitations. In initial round table discussions to assess the baseline, the knowledge gathering about the caretakers was done from important yet critical stakeholders in the system, but not directly from the caretakers. Their inclusion may have resulted in learning about lived experiences of caregivers. The premise was set with their understanding of the felt need for skill building as viewed by others. However, the cognitive interviewing at the end of the designing of the tool provided reasonable feedback which was in line with the initial premise.
Conclusion
There is an imperative need for the delivery of adequate socioemotional care in childcare institutes for vulnerable children. This study’s objective is to develop and validate a KAP questionnaire survey to assess the existing knowledge of caregivers in CCIs which further leads to the development of a training module for efficient psychosocial care of children in such institutional homes. This tool covers major aspects of caregiving and has been scientifically validated by a variety of mental health experts. The final version of the KAP can be administered among caretakers in institutional homes for children in Indian context. The results of the survey will provide the inputs needed for the design of an effective program, as well as the baseline data for the future evaluation of the success of the program.
Footnotes
Acknowledgements
The authors would like to acknowledge the Department of Women and Child Development, Delhi, for providing the necessary approval to conduct research in CCIs across the Delhi district. The authors also extend their gratitude to the superintendents, welfare officers as well as the caretakers for their cooperation and for generously providing their valuable time.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is a part of minor research project funded by Indian Council of Social Science Research (180/2022-2023/ICSSR/RP/MN/GEN). The grant is received by Dr. Prerna Sharma, Project Director. The project is titled “Developing caregiver training module for staff working in Govt. and Govt. funded Child-Care Institutes in Delhi.”
Statement of Informed Consent and Ethical Approval
Written Informed Consent was taken from all the participants. The study was accorded Ethical Committee Approval vide Ethics Committee (mention Name and Institute) No. IEC-IHBAS 2023/4/2/V-1 dated 28 April 2023. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Appendix A
Knowledge, Attitude, and Practice (KAP) Schedule for Caretakers of Childcare Institutes
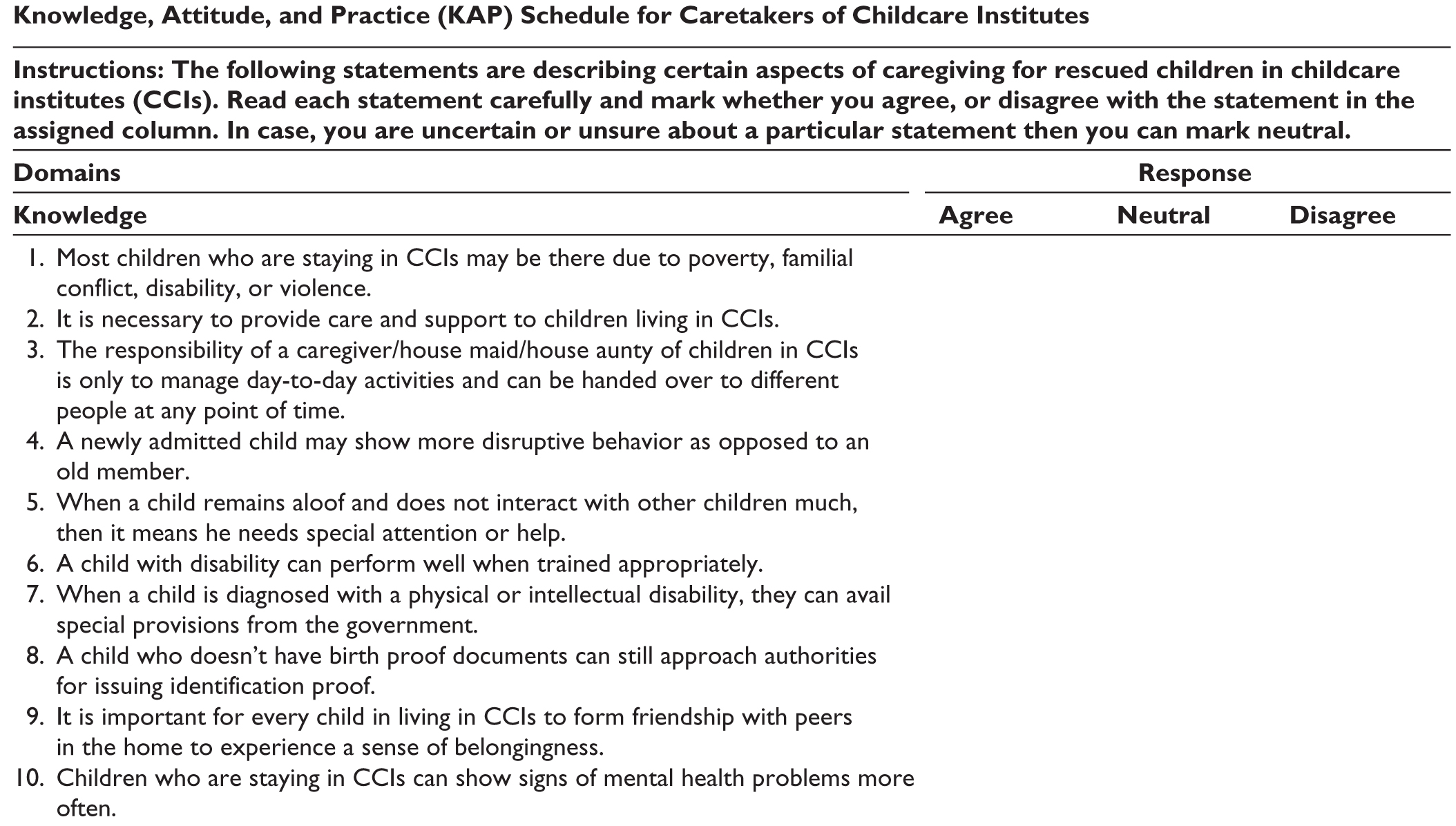
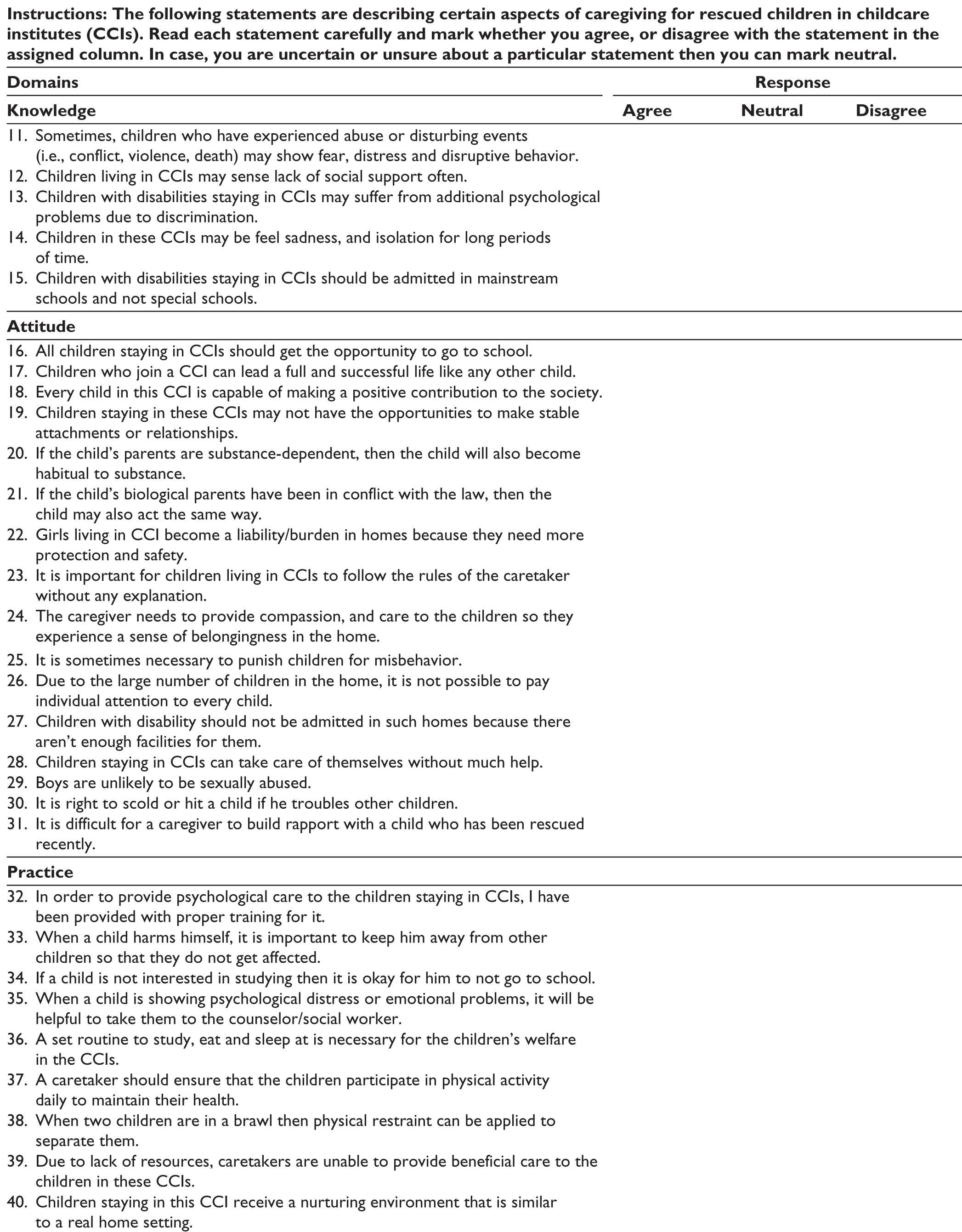
| Instructions: The following statements are describing certain aspects of caregiving for rescued children in childcare institutes (CCIs). Read each statement carefully and mark whether you agree, or disagree with the statement in the assigned column. In case, you are uncertain or unsure about a particular statement then you can mark neutral. | |||
| Domains | Response | ||
| Knowledge | Agree | Neutral | Disagree |
| 1. Most children who are staying in CCIs may be there due to poverty, familial conflict, disability, or violence. |
|
||
| 2. It is necessary to provide care and support to children living in CCIs. | |||
| 3. The responsibility of a caregiver/house maid/house aunty of children in CCIs is only to manage day-to-day activities and can be handed over to different people at any point of time. | |||
| 4. A newly admitted child may show more disruptive behavior as opposed to an old member. | |||
| 5. When a child remains aloof and does not interact with other children much, then it means he needs special attention or help. | |||
| 6. A child with disability can perform well when trained appropriately. | |||
| 7. When a child is diagnosed with a physical or intellectual disability, they can avail special provisions from the government. | |||
| 8. A child who doesn’t have birth proof documents can still approach authorities for issuing identification proof. | |||
| 9. It is important for every child in living in CCIs to form friendship with peers in the home to experience a sense of belongingness. | |||
| 10. Children who are staying in CCIs can show signs of mental health problems more often. | |||
| 11. Sometimes, children who have experienced abuse or disturbing events (i.e., conflict, violence, death) may show fear, distress and disruptive behavior. | |||
| 12. Children living in CCIs may sense lack of social support often. | |||
| 13. Children with disabilities staying in CCIs may suffer from additional psychological problems due to discrimination. | |||
| 14. Children in these CCIs may be feel sadness, and isolation for long periods of time. | |||
| 15. Children with disabilities staying in CCIs should be admitted in mainstream schools and not special schools. | |||
|
|
|||
| 16. All children staying in CCIs should get the opportunity to go to school. | |||
| 17. Children who join a CCI can lead a full and successful life like any other child. | |||
| 18. Every child in this CCI is capable of making a positive contribution to the society. | |||
| 19. Children staying in these CCIs may not have the opportunities to make stable attachments or relationships. | |||
| 20. If the child’s parents are substance-dependent, then the child will also become habitual to substance. | |||
| 21. If the child’s biological parents have been in conflict with the law, then the child may also act the same way. | |||
| 22. Girls living in CCI become a liability/burden in homes because they need more protection and safety. | |||
| 23. It is important for children living in CCIs to follow the rules of the caretaker without any explanation. | |||
| 24. The caregiver needs to provide compassion, and care to the children so they experience a sense of belongingness in the home. | |||
| 25. It is sometimes necessary to punish children for misbehavior. | |||
| 26. Due to the large number of children in the home, it is not possible to pay individual attention to every child. | |||
| 27. Children with disability should not be admitted in such homes because there aren’t enough facilities for them. | |||
| 28. Children staying in CCIs can take care of themselves without much help. | |||
| 29. Boys are unlikely to be sexually abused. | |||
| 30. It is right to scold or hit a child if he troubles other children. | |||
| 31. It is difficult for a caregiver to build rapport with a child who has been rescued recently. | |||
|
|
|||
| 32. In order to provide psychological care to the children staying in CCIs, I have been provided with proper training for it. | |||
| 33. When a child harms himself, it is important to keep him away from other children so that they do not get affected. | |||
| 34. If a child is not interested in studying then it is okay for him to not go to school. | |||
| 35. When a child is showing psychological distress or emotional problems, it will be helpful to take them to the counselor/social worker. | |||
| 36. A set routine to study, eat and sleep at is necessary for the children’s welfare in the CCIs. | |||
| 37. A caretaker should ensure that the children participate in physical activity daily to maintain their health. | |||
| 38. When two children are in a brawl then physical restraint can be applied to separate them. | |||
| 39. Due to lack of resources, caretakers are unable to provide beneficial care to the children in these CCIs. | |||
| 40. Children staying in this CCI receive a nurturing environment that is similar to a real home setting. | |||