
Abstract
Purpose of Review:
Grief in children and adolescents is uniquely different, depending on their developmental stages and level of understanding. It may occur due to the death of a loved one, or due to other intangible losses such as moving out of a neighborhood. Grief is not often expressed spontaneously by children, which leads the caregiver to believe that the child is coping well with the loss. Unanticipated deaths, preexisting psychological vulnerabilities in the child and inadequate coping mechanisms in the existing caregivers lead to more severe grief reactions.
The following article is a narrative review describing grief in the younger population, along with developmental contexts, role of culture, complex presentations of grief and an overview of management.
Collection and Analysis of Data:
Developmental considerations form the core of identifying, evaluating, and treating grief. Contrary to what is believed, even infants can identify the loss of the caregiver and react to the loss. Secondary losses such as a change in lifestyle also impact significantly. Grief in children with developmental disorders is often misinterpreted, as grieving children may not be able to communicate or understand their own distress. Grief may also result in somatization and conversion reactions.
Conclusion:
It is important to identify grief in children and adolescents, especially in recent times, due to increased unexpected deaths due to the COVID-19 pandemic, leading to bereavement in many children and adolescents. Interventions for grief are necessary to prevent consequences such as complicated grief, increased severity of depression, post-traumatic stress disorder (PTSD), poor socio-occupational functioning, substance use and self-harm.
Keywords
Background
Grief in children and adolescents can be distinctly different from that in adults, and can often be misinterpreted as stress, anxiety, depression, adolescent moodiness, part of developmental disorders, and behavioral disturbances. The different developmental stages entail different levels of understanding of the concept of death. In addition, the nature of the relationship with the bereaved (parent vs. extended family), suddenness of loss, and traumatic losses (accidents, disasters) can also influence the presentation of grief in children. 1
About 4% of young people in Western countries experience the death of a parent before the age of 18. 2 According to the United States (US) Census Bureau, about 1 in 20 children below the age of 18 have experienced the death of one or both parents. 3 About 70,000-75,000 children die each year in the US, most of whom have siblings who have to contend with this loss. 3 Grief due to parental loss prior to age 18 has also led to long-term consequences as per a longitudinal study of 7 million people in Scandinavia, who remain at increased risk of suicide for at least 25 years. 4
Data concerning the incidence and prevalence of childhood and adolescent grief are lacking in the Indian population but can be expected to have similar or increased rates, considering a higher overall mortality rate compared to developed countries.
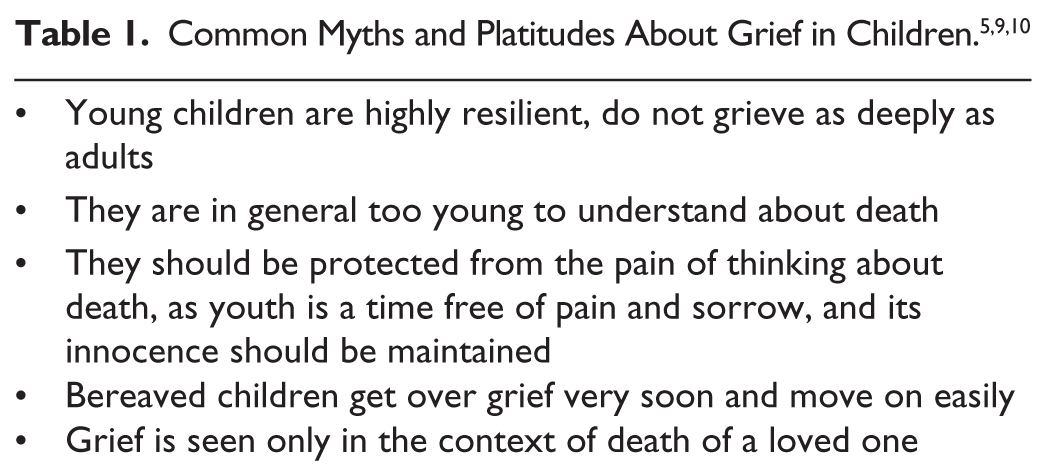
Notwithstanding the inadequate epidemiological data, there are many prevailing myths and misconceptions which make the identification and management of grief in children and adolescents difficult (Table 1).
In spite of the significant impact grief can have on children and adolescents, very little time is dedicated to training medical students and postgraduates in the assessment and management of grief, especially during critical periods of development. This review aims to provide students and practitioners (psychiatrist/clinical psychologist/pediatrician/other health care provider) with the foundational knowledge and skills to communicate effectively about death, loss, appreciate socio cultural factors associated with grief, identify diverse ways grief can manifest across developmental stages, strategies to ensure long-term consequences such as unresolved/complicated grief can be prevented, and to facilitate adaptive grief interventions for children and their families.
Materials and Methods
Search Strategy. Study Selection, and Data Extraction
Electronic searches of MEDLINE, PubMed, and Google Scholar were carried out from inception till December 2023. We used the following search terms which included combinations of MeSH or free text terms—“grief in children and adolescents,” “developmental considerations for grief in children,” “assessing grief in children,” “impact of grief of children on the family,” “social and cultural factors in grief in children,” “grief in children with neurodevelopmental disorders,” “grief in children and COVID 19,” and “interventions for grief in children.” Reference lists of generated articles were also hand searched to ensure completeness.
Inclusion criteria were English language articles with full text, which discussed grief in children and adolescents. We excluded articles without full text and which did not specifically focus on children and adolescents. Case studies were also excluded.
Searches were done by all authors independently, and the final list of articles was decided by discussion and consensus. The initial search yielded 886 articles, of which relevant English language articles with full text were examined, and 33 articles were chosen for this narrative review, analyzed, and synthesized as the following themes: (a) Causes of grief in children and adolescents. (b) Types of grief and complex presentations. (c) Developmental considerations for assessing grief in children. (d) Outcomes of grief in children. (e) Treatment interventions for grief.
In addition to the information obtained from various articles, other novel clinical perspectives have been incorporated into the present article, gleaned from personal experience of the authors in working with children and adolescents and their families dealing with grief.
This current review did not explore in depth, grief associated with end-of-life care for children, grief in the contexts of refugee children and those who have been victims of war-related trauma, grief in children who have been orphaned and child & adolescent homicide survivors. We have also not described the impact of social media and the internet on grieving in children and believe that along with all the above these should be areas of future study and review.
Grief in Children and Adolescents
What Causes Grief?
The concept of “grief” cannot be limited to the death of a loved one but is a natural response to any kind of loss. 5 In children, this loss may be in the form of death of parents, siblings, grandparents, significant family or friends, pets; loss of intact families through separation, divorce; the loss of home, neighborhood, friends, teachers and school due to moving; the loss of a loved one to incarceration/addiction/homelessness; moving away of a sibling to higher studies; losing a favorite possession or toy; death of a celebrity or role model (e.g., Sushant Singh Rajput/Kim Jong-Hyun); break up of a romantic relationship or peer group.
Grief can also occur in children suffering from chronic, debilitating or terminal illnesses in the form of loss of connection with school, peers and family due to symptoms, missing classes, activities such as art, sports and music due to prolonged hospital admissions, disruption of developmental trajectories in social, educational and home spheres. Grief can also occur for the loss of physical capacity, prior appearance, and bodily integrity. 5 It is both a cognitive and emotional necessity for children and adolescents to grieve.
Common Grieving Mechanisms and Processes
Grief may not often be expressed spontaneously by children, as children often recognize that their questions make adults uncomfortable, and do not pursue such discussions. They may assume that the questions were inappropriate, in case the adult reacts with sadness or distress. They may worry that they may lose other adults the same way they lost this loved one. Oftentimes, children may offer support to grieving adults, which can impress upon the caregiver that the child is coping well and does not need assistance. 6
Some thought processes occur commonly to grieving children following a loss. The first consists of a shift in self-concept: Did I cause this to happen? Children may view the loved one’s death as a desertion. There may also be a sense of ineffectuality in controlling life events occurring in relation to self and immediate family: Why couldn’t I stop it? There may also be identification with the bereaved. The child may emulate the qualities of the bereaved, which may be an unconscious defense mechanism. Denial and idealization are other defense mechanisms commonly employed by grieving children. 1 Will it happen to me too? is a common question which occurs to many children, along with worry about the future and the surviving caretaker: Who will take care of me now?. Some children are also unable to move beyond the idealization of their parent after their death, often unable to free themselves to build their own identity or “become their own man/woman” and continue to underplay the parent’s limitations, even when they had been mistreated by the parent and sometimes adolescents continue to use this pattern in their other relationships with peers and partners.
What Makes Some Children More Vulnerable than Others?
A population-based longitudinal study found that the type of death (unanticipated, homicide, suicide), preexisting psychological vulnerabilities in the child or existing parent contributed to more severe grief reactions. 7 Another study evaluated the effect of parental coping in the surviving parent and found that maladaptive parental coping styles had a major impact on the child’s grief symptoms. The difficulties are also said to be greater when a prior relationship with the deceased had high ambivalence or high dependence. 8
Types of Grief
Uncomplicated grief is wherein the child has symptoms such as sadness, distress, anger, loss of appetite, sleep disturbance, but is able to complete the mourning process and heal. 5
Complicated grief is seen when the child is not able to adapt to the loss. Symptoms may be similar to uncomplicated grief but greater in intensity and duration. Certain factors prevent or delay the normal grief process. 5
These reactions may be chronic (persisting beyond the usual period of six months) or delayed (child may not have comprehended the loss initially, and there is a delayed onset and an overwhelming reaction). Some children may experience additional anxiety, depressive episodes, symptoms of post-traumatic stress disorder (PTSD), along with symptoms of grief, leading to exaggerated grief reactions. On the other hand, some children may manifest physical symptoms such as headaches, body pains, and sometimes, exaggeration of preexisting physical conditions instead of emotional symptoms, called masked grief reactions. 9
The concept of complicated grief in children is poorly understood even by clinicians, as evidenced by a survey in which experienced clinicians participated. It showed that there was difficulty in defining complicated grief in children, but that intensity and duration were major defining aspects. They also felt that using adult criteria was inappropriate for children. 10
It is therefore clinically challenging to know when to intervene or when to let grief take its natural course. It is suggested that professional intervention is required when grief persists longer than that expected by the cultural norms and evidence-based expectations, and when it disrupts the natural progression from acute to integrated grief or starts becoming maladaptive.
Childhood Traumatic Grief (CTG)
Cohen et al. describe a form of grief which occurs after certain types of loss, such as violent/unexpected deaths during natural disasters, terrorism, war, homicide or suicide. Here, maladaptive patterns of grief which contain symptoms of unresolved grief, PTSD, along with depressive symptoms develop. Unusually, such symptoms may also occur in losses which are not conventionally “traumatic.” Nonetheless, these symptoms need to be addressed irrespective of the type of loss, first targeting the trauma symptoms and then moving towards grief-related symptoms. 11
Anticipatory Grief
Described as a response to the threat of death rather than the death itself, it focuses on the past and present losses in addition to future losses. There may be a rehearsal of death, with time available to accept death and resolve issues. Mourning is for both the past experiences as well as the future which the loved one will never have. It is common in children of terminally ill parents and should be identified and supported.5,11
Disenfranchised Grief
Disenfranchised grief is a type of grief that is often not socially validated or openly acknowledged or culturally recognized. In the authors’ experience, in children this encompasses a wide range of situations such as the child’s expectancy of having a sibling but mother having a stillborn/abortion, loss of an undisclosed pregnancy in an adolescent girl, loss of the partner of a culturally unsanctioned relationship, such as same sex partners, a grandparent having dementia/cognitive loss or a sibling leaving home for studies or a career (“sibling empty nest syndrome”). 12
Differentiating Between Complicated Grief and MDD
At first glance, though both may appear similar, there are certain qualitative differences which help differentiate the two. In grief, depressed mood is focused specifically on the loss, anhedonia is rare, yearning or longing is prominent, anxiety and guilt are focused on issues related to the deceased. Preoccupying thoughts about the loss are predominant instead of depressive cognitions, and avoidance is focused on reminders of the loss rather than generalized social withdrawal. Suicidal thoughts and behavior may be seen in both. 5
Developmental Considerations as the Cornerstone of Assessing Grief
During the early period of childhood and adolescence, specific reactions are highly likely to be influenced by the level of development. Grief reactions are no different. The impact of loss and trauma on children depends heavily on the life stage during which the event occurs. An understanding of the child’s concept of death is necessary for one to assess grief.
By two to five years of age, the concept of definitiveness and irreversibility is not yet developed, there is an intense curiosity about death, and it is often considered akin to protracted sleep. By five to nine years of age, the concept of definitiveness develops, but a belief that there is possibly a way out of it continues to be held. By nine years and older, death is understood as irreversible and inevitable for all living creatures. 13
This concept development is not necessarily fixed, and an understanding of death may develop sooner or later. An exploratory study in Indian preschool children aged three to five years revealed that many understood the universality and irreversibility of death, but few were able to comprehend non-functionality. It was found that most people avoided talking about death to children even when required, as they were unsure about when children start understanding the concept of death. 14
Infants are able to detect the absence of caregivers—there is a loss of the familiar person, disruption of daily routines, smells, voices, and touch of the loved one. The child is at the sensorimotor stage, where sensory motor skills are just developing and there is no verbal development. Grief may therefore manifest itself in the form of irritability, crying, difficulty to soothe, changes in sleep and feeding patterns, withdrawal, frustration, aggression, separation anxiety, and clinginess, with fear of unfamiliar adults. At this stage the infant could also be reacting to the adult’s grief or the exposure to adult distress. Impact of an emotionally unavailable parent, as in a lack of attunement and attentiveness, also needs to be considered.
By preschool to five years, language and cognitive skills are still immature, there is egocentric, moralistic, and magical thinking. Being in the preoperational stage of cognitive development, they may fail to gain abstract concepts completely, and resort to concrete thinking (e.g., Bad things happen to bad people. I didn’t put away my toys, that’s why he died. It’s all my fault).
Irreversibility and non-functionality concepts of death are not adequately developed, and questions about when the person will come back are frequent, with anger towards the deceased for delaying return, and fear of abandonment. Symptoms are in the form of anxiety, distress, temper tantrums, aggression, regression (return to thumb sucking, loss of toileting skills) and themes of death expressed through play and behavior. 15
Primary school age: School children may be significantly preoccupied with their own needs and how the loss will affect them in the long run. They continue to have magical thinking, and may believe that it is their fault, leading to guilt and regret. They may start worrying about the existing caregivers, about their health and their potential death, offer support, assume a caregiving role to the parent and sibling, inhibiting their feelings of sadness and fear. There is concrete thinking, and vulnerability to faulty beliefs (e.g., It is the hospital which caused death, rather than the illness). There may be repetitive, specific questions about death (such as what happens to the body when buried), which need to be addressed with correct information and concrete language. Symptoms may present as disrupted sleep and appetite, nightmares, somatic complaints, behavioral changes (withdrawal, aggression), regression, learning difficulties, fluctuation about short periods of strong reaction and usual behavior (as though nothing has happened), and playing out themes to understand the changes.5,15
Preadolescents and Adolescents: Adolescents are less likely to accept help when offered, as they are transitioning to individuation from the family. Emotional experiences are usually kept private and may be discussed more with peers than family. However, the need for conformity with the peer group may lead to a sense of isolation and make them unwilling to openly talk about grief. There is greater cognitive capacity (abstract thinking, problem solving, reasoning) which allows for rumination, overthinking and intellectual struggle (“Why me?” and the unfairness of death), with an adult approach to grief.
Symptoms may present themselves according to internalizing and externalizing temperaments. There may be anxiety, depression, guilt, withdrawal from support systems, inability to concentrate, hypervigilance, fear of death/violence occurring again, thoughts of self-harm and suicide. There may also be an increase in risk-taking behaviors, substance use, aggression, anger outbursts, delinquency, acting out behaviors and so on. They may also start questioning religious beliefs, and some may start exploring spirituality.5,15
Impact of Secondary Losses
Secondary losses are the losses of aspects of life which would have been contributed by the person who died, such as a change in lifestyle (change in financial or social status), change of city, school, loss of relationship with friends and family of the person who died, less time available with the surviving parent, who may have to take on more responsibilities, loss of specific activities (the parent who died may have been taking the child to sports matches and cheering for them), a loss of safety and trust in the world in general. Some losses may become tangible only years later, such as a person experiencing a loss of her mother’s advice and expertise when her own child is born.
The Family’s Role
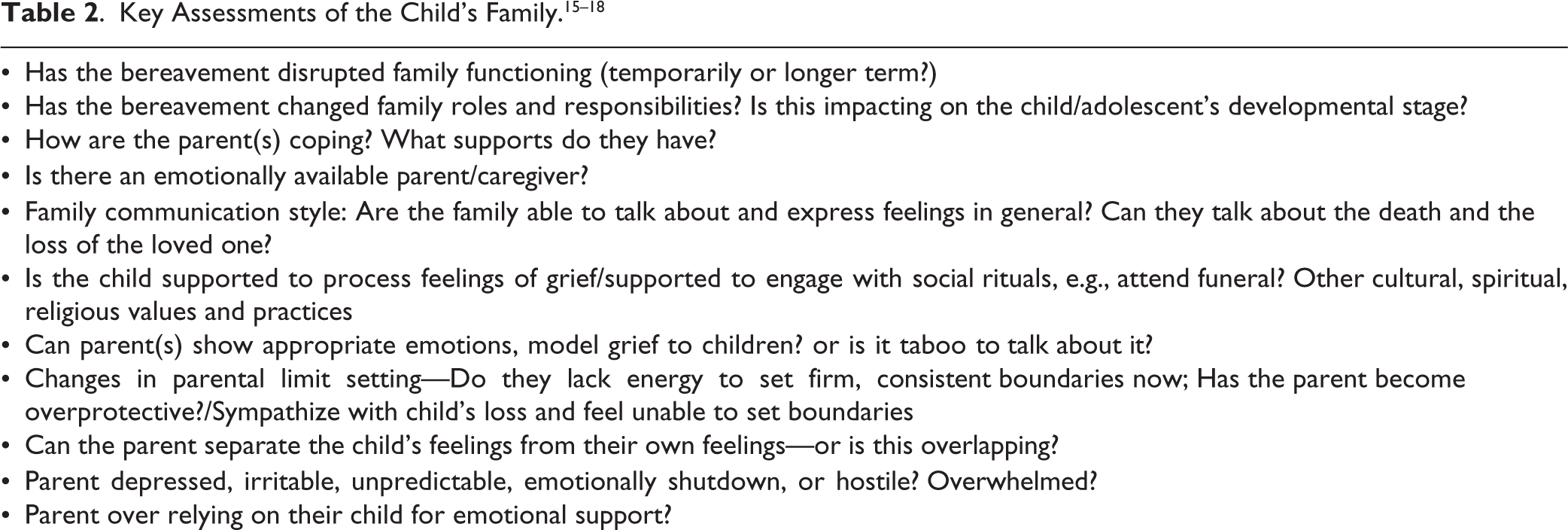
The family forms the immediate environment for the bereaved child, and it is important to understand the family’s position, as the family as a whole also grieves, which again impacts the child. Interventions should take the family context into consideration. The factors to be assessed while evaluating the family are mentioned in Table 2.
Socio-cultural Considerations
The expression of grief and mourning are different in different cultures, in the form of various customs and rituals. Dr VK Verma’s article “Cultural Psychodynamics in Health and Illness” talks about “cultural defences” like individual defense mechanisms to cope with anxiety. 19 This cultural defense can be provided by customs, traditions, rituals, sanctions, prohibitions, or symbolisms, and may serve as a coping mechanism in particular situations. For instance, elaborate rituals exist in India during mourning in almost all cultures, which enables family members to express their emotions about the deceased person and serves as a “Natural Psychotherapy” recommended for grief resolution. A few days in a year are dedicated to paying homage to ancestors in Hindu culture. Some cultures approach death as a celebration of life, honoring and celebrating the deceased on Dia de los Muertos (Day of the Dead). 20 The beliefs of “After Life” and “Reincarnation” in some cultures may provide spiritual consolation that it is not the “end” for the deceased soul.
Complex Presentations in Grief
Grief and Developmental Disorders
Diagnosing and managing grief in children with developmental disorders is a doubly challenging task, as these children may not have the verbal ability to express their thoughts and emotions. This may lead to non-recognition or misinterpretation by the caregiver and healthcare provider. Conversely, the grieving child himself or herself may not understand why the changes are occurring, complicated by the fact that there is a limited repertoire of confidantes. The limitations of language skills, cognitive difficulties, decreased or altered expression of emotions are some of the biggest challenges. In addition, there may be a learnt tendency to respond positively (pleasing people for social acceptability). Oftentimes, the child may not be informed about the death, or sometimes given false information, such as, They’ve gone on vacation/They have moved to another city. Family members treat them differently, leading to an overprotection from death and related themes. This can lead to a delayed grieving process, along with a loss of trust in the existing caregiver.21,22
In addition to death or separation, these children have to routinely contend with other often ignored secondary losses such as disrupted relationships with peers and family members, loss of functioning or ability, loss of independence, opportunity, and a loss of identity. Grief in children with developmental disorders may manifest in the form of somatic complaints (headache, stomach pains), social withdrawal, increased compulsive behaviors, ritualization, and self-stimulatory behaviors (hand flapping, twisting, head-banging). 23
Significant secondary losses, poor communication ability, poor understanding and non-development of coping mechanisms leads to increased risk of pathological grief in these children.
Conversion Disorder
Grief converted into symptoms can often result in somatization and conversion reactions. Recent loss of a loved one was a contributory psychosocial factor in 12.5% of children with conversion disorder assessed in an Indian population. 24 A study evaluating conversion disorders in children found unresolved grief reactions in 58% of the study sample. 25 Grief, presenting as conversion reactions, are poorly studied. However, even with the existing research, the clinician would be justified in considering the possibility of unresolved grief when evaluating conversion disorders in children and adolescents.
COVID-19 and Grief
Increased unexpected deaths due to the COVID-19 pandemic has led to bereavement in many children and adolescents, with about 2.2 children and 4.1 grandchildren bereaved for every person who dies. 26 In addition to the suddenness of the loss, various other factors such as forced social isolation, not being able to say goodbye to loved ones by being with them during their last minutes, loss of comfort of physical contact such as hugs have increased the risk of complicated or unresolved grief. In addition to losses due to the death of near and dear ones, unemployment in the family, lack of food supplies, and financial concerns also contribute to complicated grief, especially in children from disadvantaged backgrounds. 27 Some may even have had multiple deaths in the family. Parents may have been unable to provide adequate support due to their own losses, financial insecurities, and increased responsibilities. However, it cannot be ignored that the lockdown had increased the time spent with family members, and this may have contributed to improving relationships. 28
Outcomes of Grief in Children and Adolescents
A longitudinal study of bereaved children, adolescents and their families, with yearly assessment for up to three years after parental death showed that 30.8% showed grief reactions for more than nine months after death, after which they resolved. A total of 10.4% of individuals had sustained grief reactions even after three years of death. The rest showed rapid resolution of symptoms within one year of death. Prolonged grief also predicted earlier onset of depression. 7 A population-based study in bereaved families with biological offspring of 7-25 years of age showed that bereaved offspring and their caregivers had an increased risk of depression and PTSD, and bereaved offspring had three-fold increased risk of depression even after controlling for other risk factors. 29 Separation anxiety, depression, conduct disorder and substance abuse were more likely to be seen in bereaved than non-bereaved children. Another study found that bereaved youth had lower competency at work, lower peer attachment, decreased educational aspirations, and less elaborate planning for future careers. These were more commonly mediated by the effect of bereavement on caregiver and child functioning as well as family climate. These outcomes were not related to the age at the time or cause of parental death or gender of the deceased parent. 29
Treatment Interventions for Grief
General Principles
To work in the intervention of grief, one must be aware of one’s own grief issues, should be able to interpret the range of normal grief behaviors and permit individual differences in coping strategies. In children, there may be an additional need of being there for the surviving parent while they reinterpret death evolving through their cognitive abilities.
Many children traverse the tasks of mourning and find their way to integrated grief without professional assistance. Helping identify their personal supports/circles so they know whom to reach out to when they need to talk or emote or want reassurance or guidance is important. Such local “safety nets” could include compassionate friends, peers at school, religious organizations, school/local counselors, and teachers. These could be sources of active listening and granting safe space in which they can tell and retell their stories of grief until they feel the narrative is more integrated.
The body of literature on resilience indicates it can be unproductive to introduce “grief work” to a child when it is not needed. For the smaller percentage of those who experience grief that significantly disrupts functioning in the months or years after a death, therapeutic interventions can facilitate more constructive coping. Professional help is often a must when thoughts, emotions, and behaviors arise during grief that (a) persist longer than expected by cultural norms and evidence-based expectations, (b) disrupt the natural progression from acute to integrated grief, and (c) become maladaptive. Identifying red flags like prolonged withdrawal, self-harm or severe changes in behavior is extremely important and should warrant professional help.
Encouraging open communication, providing age-appropriate information, normalizing grief reactions and providing social support from the ground rules during grief intervention in children. Using creative therapies like art play and music can ease the expression of emotions in grieving children. Supporting structured daily routines, teaching coping skills through techniques like breathing exercises and mindfulness can go a long way.30-32
One important element of the treatment process is for the child mental health professional to work with the parents, especially when the grief is with younger children. Following are some strategies that could be used in helping parents:5,9,33
For pre-school children, parents should answer the child’s questions around the bereavement in a simple yet factual manner. Not helpful to lie or tell half-truths, avoid confusing terms and euphemisms, for example, a long sleep, on a trip, lost, etc. A few identifiable triggers—Death anniversaries, birthdays, holidays, Mother’s Day, Father’s Day, and graduations, may be triggering events for grief. Prepare the child for loss where possible, for example, illness. Children need to continue to develop mastery of their world. Provide a structured environment that is consistent and predictable. Positive regard, warmth, nurturing, and affection are important, but important to reinforce the idea to parents that love does not mean becoming permissive. Emphasize to parents the need to contain acting out behavior, to not allow for school refusal to build. Parenting factors also need to be addressed by the mental health professional, especially overprotectiveness, enmeshment, over-reliance. Be patient with regressive behaviors (no need for trigger finger responses to thumb sucking!). Maybe engaging with activities with the child is better than talking. Provide more opportunities for play. Creating linking objects—Children may fear that they will lose memories and forget the loved one as time passes, especially when they were younger, when the person died. Help memorialize and retain connection to their loved ones through memory boxes, photo albums, family videos, keepsakes. For adolescents, parents should encourage them to find prosocial outlets in physical and creative activities. Independent assessment & treatment of the surviving parent may become necessary in some cases.
More specific interventions with the child can involve the following:
Explore defense mechanisms and positive and negative coping styles: Important to remember that defense mechanisms apart from serving the objective of self-preservation, also reflect the deeply ingrained socio-cultural norms and expectations that shape the child’s actions and beliefs. Changing these beliefs and generating insight must be done gradually, since breaking defense mechanisms without creating alternative constructive coping styles can be dangerous. Cognitive behavioral therapy—Cognitive behavioral strategies to help reframe negative cognitions (filtering, personalizing, catastrophizing, and so forth), and reality testing or generating evidence for/against can assist with prevalent guilt. This should also involve identifying avoidance behaviors and teaching to avoid avoidance (there is no way through it but through it). The professional should be able to ultimately use developmentally appropriate language to help the child process grief and a coherent narrative. To create coping skills toolboxes with the child, for use when they feel overwhelmed (coping cards, emotion regulation strategies). Play therapy—This could involve a variety of play materials available such as art supplies, blocks, dolls, puppets, rescue vehicles, and medical kits, to name a few. Children often use these “props” to play out their versions of the death scene. Some play therapists are directive and ask children to play with specific play materials and to show (with the toys) how the person died: Others are non-directive and instruct children to choose any toy and to self-select activities. The implicit belief of both types of therapists is that children will use play materials to act out anxieties and fears. In children with developmental disorders who may either have limitations with language skills or may resist talking, urging them to communicate grief and associated emotions with multi-sensory components such as writing, role play, drawing, listening to music, or playing a game, could be useful. Other creative outlets—There are anecdotal reports for the use of music therapy, bibliotherapy, puppet and doll play, storytelling, letter writing in children who find it difficult to articulate their grief.
Conclusion
Children have different ways of coping with loss than adults. Children need consistently available adult parenting figures to process a loss and tolerate the painful feelings. Their limited cognitive development may hinder their understanding of death and may re-process things as they mature and acquire capacity at different developmental stages. A child’s identity may be affected by a loss because self-development is still in process. Provision of active listening; education about grief—its physical, psychological, and spiritual effects is vital. Primary tasks of mourning, performance of risk assessment, teaching of coping strategies are important components of effective work with grieving children and families. In Indian families, though, there would be some alternate caregiver taking up the responsibility of “looking after the child,” it is often seen as a replacement of the deceased, which the child may not resonate with. It becomes very important to educate families about handling grief in children.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The research study uses publicly available secondary literature and data; thus, it did not require any ethics approval or participant consent.