
Abstract
Introduction:
Health-risk behaviors among adolescents are increasing at an alarming rate, as observed by families, educational institutions, and medical professionals. These risk behaviors are diverse and extensive. There is a need to identify the indulgence of adolescents in various risk behaviors and have a composite assessment of the same for any planned intervention initiative to enhance adolescent well-being. The authors, endorsing this need, have attempted to develop a comprehensive scale to assess the overall health-risk behavior of adolescents.
Material and Methods:
The adolescent health-risk behavior scale was standardized on a sample of 1388 adolescents aged 14-19 years from India.
Results:
The initial scale of 49 items was run through an exploratory factor analysis, resulting in a 30-item scale with nine factors. A confirmatory factor analysis resulted in a final scale of 20 items with seven factors.
Conclusion:
The scale showed satisfactory reliability and validity measures, resulting in a comprehensive assessment tool to assess adolescent risk behaviors. The scale can be used not just for research but also as a simple and comprehendible diagnostic tool to assess adolescent risk behaviors.
Health-risk behaviors (HRBs) are actions undertaken by individuals at a frequency or intensity that elevates the likelihood of disease or injury, irrespective of their awareness regarding the potential outcomes of such behaviors. 1 At times, the effects associated with HRBs can be profound, leading to outcomes such as death, permanent disability, or societal issues. 2 Adolescence is a stressful time and a period of rapid transformation where susceptibility to engage in risky behavior is high. According to the World Health Organization (WHO), 3 over 4500 adolescents and young adults between 10 and 24 years die every day across the globe, primarily due to injuries from road accidents, interpersonal violence, and self-harm. In most circumstances, they are preventable. Adverse health behaviors raise morbidity and mortality rates, and there is a dire need to address them. However, from a global perspective, the major HRBs encompass unhealthy sexual activities, consumption of alcohol, tobacco, and other substances, actions causing accidental harm or violence, unhealthy eating patterns, substandard hygiene habits, and insufficient physical exercise. 4
In India, research shows that about 10%-30% of young people engage in risky health practices such as unhealthy dietary habits, lack of physical activity, acts of violence, unsafe sexual behaviors, and risky practices on roadways. 5 HRBs, such as substance abuse, reckless driving, and unprotected sexual practices, not only have long-lasting repercussions on the adolescent’s future but also contribute to the economic and social growth of the country.6,7 These behaviors often go unaddressed due to inadequate assessment. It is essential to develop a simple and comprehensive assessment tool to effectively evaluate these behaviors.
Youth Risk Behavior Survey Questionnaire 8 and Global School-based Student Health Survey Questionnaire 9 are the frequently used questionnaires in India to assess HRBs.10–12 However, all the items within these questionnaires are not culture-free, which limits their applicability in the culturally diverse Indian context. One of the major criticisms of these scales is the non-uniform response cues that cannot stand the test of advanced statistical treatment. 13 Alternative scales, viz., the Health-Risk Behavior Inventory for Chinese Adolescents 13 and Health-Risk Behaviors Scales by Çimen and Savaşer 14 and Courtenay et al. 15 are widely used by researchers but are not found to be holistic and comprehensive. On the other hand, Perkins Adolescent Risk Screen, 16 Problem Oriented Screening Instrument for Teenagers, 17 Adolescent Risk Behavior Screen, 18 and Risky, Impulsive, and Self-destructive Behavior Questionnaire 19 do not capture the entire spectrum of adolescent HRBs.
The abovementioned concerns indicate the need for measures specific to the geographical and demographic contexts. 20 To address the limitations of cultural specificity, length, and broader inclusivity of HRBs, there is a need to develop a comprehensive scale to measure risk behaviors among adolescents. The construction and validation of the adolescent health-risk behavior scale (AHRBS) is an attempt to address these limitations. The study’s main objectives were to (a) develop a self-report scale to assess HRBs among adolescents, (b) assess its underlying structure, and (c) examine the psychometric properties of the constructed scale.
Methods
Participants
Through purposive sampling, adolescents aged 14–19 were recruited from different schools and colleges in Kerala and Telangana (India). The pilot study was conducted on 229 adolescents aged between 10 and 19 years (Meanage = 16.13, standard deviation (SD)age = ±2.04), including 106 males and 123 females. Two separate datasets were considered for exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). For the EFA, data were collected from 1,071 adolescents between 14 and 19 years (Meanage = 16.69, SDage = ±1.57), including 585 males and 486 females. For CFA, separate data were collected from 317 adolescents aged 14–19 years (Meanage = 17.30, SDage = ±1.51), including 125 males and 192 females. The inclusion criteria consisted of male and female adolescents aged 14–19 years with a basic understanding of English. Adolescents with physical or psychological problems were excluded.
Procedure
The Institutional Ethics Committee’s approval was followed by official permissions from the educational institutes. Informed consent was obtained from parents for participants under 18 years of age, while participants aged 18 and 19 provided their own consent. Additionally, participants under 18 signed an assent form to indicate their agreement to participate.
Adolescents under 18 were initially addressed in their classrooms for 10–15 min, during which rapport was established, and an overview of the study was provided. Consent and assent forms were sent home with the participants for discussion with their parents. Only those who returned signed consent and assent forms were included in the study. For participants aged 18 and 19, consent procedures and rapport building were conducted directly during classroom sessions, allowing them to complete the process in a single interaction.
After obtaining consent, the AHRBS questionnaire was administered to students in a group within their respective classrooms. The students took approximately 20 min to complete the questionnaire. Before the abovementioned procedures, the scale was constructed and validated through two major phases.
Phase I: Item Construction and Content Validation
An initial pool of a 76-item questionnaire related to risk behaviors was prepared after a thorough literature search on risk behavior and its prevalence,6-9,13,14,16,18-21 by the first two authors. In the initial draft of the scale, items were listed under major HRBs identified through the literature review, including alcohol or other substance abuse, risky sexual practices, sedentary behaviors, unhealthy diet patterns, violent and aggressive behaviors, sleep hygiene, suicidal tendencies, personal hygiene, internet addiction, and on-road risky behaviors.
The scale was rated on a 5-point Likert scale ranging from almost daily (5), weekly (4), monthly (3), less than monthly (2), and never (1), as well as a not applicable (0) option for a few items. The “Not Applicable (NA)” option was incorporated to alleviate the response error. For example, a respondent selecting “never” in response to the item “wear a helmet while riding a two-wheeler” could indicate either neglect in wearing a helmet, and a participant may also select “never” when he or she does not know driving or has never used a two-wheeler altogether. This distinction highlights the necessity for nuanced response options that accurately capture the intent and circumstances of the respondent, thereby enhancing the validity of the data collected.
The initial pool of 76 items was given to 15 adolescents aged between 10 and 19 years to ascertain the clarity and relevance of the items. Four items considered redundant or lacking clarity were removed, resulting in a 72-item scale. The scale was then given to eight experts, including psychology professors, psychiatrists, practicing psychologists, and researchers, to establish the content validity. The items were retained for administration based on a content validity ratio cut-off of 0.75 and an item-level content validity index cut-off of 0.78 for individual items.22,23 A scale-level content validity index value of 0.813 indicates that approximately 81% of initially developed items were relevant for the scale construct. This eliminated 23 items, reducing the scale length to 49 items.
Phase II: Pilot Testing, Factor Analysis, and Validity-reliability Testing
The resulting 49-item scale was then pilot-tested on a sample of 229 adolescents to assess the scale’s efficiency and ease of understanding. Although the initial study design aimed to include the full adolescent age range (10–19 years) as defined by the WHO, the exclusion of early adolescents was necessary to address the ethical and practical concerns raised by parents. During the pilot testing, nearly 75% of parents of adolescents aged 10–13 raised objections to providing consent, expressing concerns about their children being exposed to specific items on the scale related to sexual behaviors and substance abuse. As a result, the decision was made to standardize the scale exclusively on middle and late adolescents (14–19 years).
For exploring the underlying structure of the scale through EFA, data from 1,071 adolescents between 14 and 19 years were collected. The retained items from EFA, along with the other three scales, were then administered to another set of participants (N = 317) to confirm the factor structure (CFA) and validation of the scale. Finally, the finalized scale was administered to 100 participants from the 317 after a gap of 2 weeks for the test-retest reliability assessment.
Measures
Teens Self-Destructive Scale
The scale consists of 35 items, 24 listed under four domains, viz., risk behaviors, negative thoughts, social support, and detachment, rated on a 5-point scale ranging from “never” to “always” (e.g., running away from home and making competitions/speeding car/bike races). The teens self-destructive scale (TSDS) is used to assess the intensity of self-harming behaviors among adolescents. Cronbach’s alpha for the scale was 0.74.
Barratt Impulsiveness Scale-15
The Barratt impulsiveness scale-15 (BIS-15) is the brief version of BIS-11 and includes 15 items, 25 rated on a 4-point Likert scale ranging from “rarely/never” to “almost always/always” (e.g., I act on the spur of the moment; I am easily bored solving thought problems). It has three sub-domains, viz., planning impulsivity, motor impulsivity, and attentional impulsivity. Higher scores indicated higher impulsivity. The scale was standardized for adolescents and adults and had a reliability coefficient of 0.78.
Healthy Lifestyle Beliefs Scale
The healthy lifestyle beliefs scale (HLBS) comprised 16 items and was developed to evaluate adolescents’ perceptions of their capacity for emotional self-regulation and participation in health-promoting behaviors. 26 It is structured around the following two key dimensions: beliefs about maintaining a physically healthy lifestyle and beliefs regarding coping and family support. Responses were gathered using a 5-point Likert scale ranging from “strongly disagree” to “strongly agree” (e.g., I am sure that I will do what is best to lead a healthy life; I deal with pressure positively). The overall reliability of the scale, as indicated by Cronbach’s alpha, was 0.89.
Data Analysis
Outlier removal was done for all datasets based on Mahalanobis distance. 27 EFA was performed to explore the underlying factor structure of the scale from the initially pooled items, followed by CFA on a separate sample. To evaluate the goodness of fit of the models, chi-square test (Minimum discrepancies of Confirmatory Factor Analysis [CMIN]/degrees of freedom [df]), comparative fit index (CFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), Tucker-Lewis index (TLI), and root mean square error of approximation (RMSEA) were calculated.28,29 Pearson’s correlation coefficients, Cronbach’s alpha, and test-retest reliability were calculated for psychometric analysis. The data analysis utilized SPSS (v20) and SPSS AMOS (v24) software.
Results
Following the development of the items, content validation, and pilot testing, the 49-item AHRBS was administered to the participants for further testing. This section offers a detailed account of handling “Not applicable” items and presents the findings from the EFA and CFA.
Dealing with “Not Applicable” Responses in AHRBS
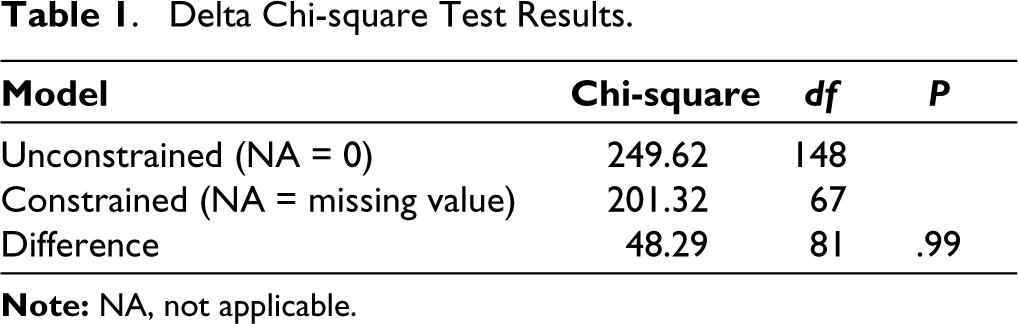
In the 49-item AHRBS administered to the participants, seven items were given an additional response option, “Not Applicable (NA).” The value to be assigned for NA response was decided by comparing two CFA models using the delta chi-square test, the first model by assigning the value “0” for “not applicable” responses and the second model by treating not applicable responses as “missing data.” The results of the delta chi-square test are displayed in Table 1. The difference in chi-square values of the unconstrained (NA = 0) and constrained (NA = missing values) models was 48.29, and the same in df was 81, with a P value of .99 (P > .05), indicating an absence of any significant difference between the models. Though the delta chi-square test indicates that the “not applicable” options can be treated with either zero or missing values, a score of zero was assigned to the “not applicable” option since substituting with missing values can lead to errors in further analysis.
Delta Chi-square Test Results.
Exploratory Factor Analysis
EFA was performed on the data to consolidate the items into underlying factors. 30 Removal of outliers based on Mahalanobis distance resulted in a dataset of 1071 responses. Multicollinearity diagnostics using variance inflation factor (VIF) and tolerance values (VIF above 4 or tolerance below 0.25 indicates that multicollinearity might exist) 31 indicated the absence of collinearity between items. The factorability of the dataset, which assumes the presence of correlations among variables, was collectively affirmed through examination of the anti-image correlation matrix diagonals (all anti-image correlation matrix diagonal values exceeded 0.50), the Kaiser-Meyer-Olkin measure of sampling adequacy (0.87), and the significance of Bartlett’s test of sphericity (P < .001).
The Kolmogorov-Smirnov and the Shapiro-Wilk normality tests were used to check the normality of the distribution. Since the distribution was found to be non-normal, the principal axis factoring extraction method, which is not sensitive to multivariate normality, was used for EFA.32–34 Promax factor rotation was applied to simplify the loading structure and interpretation of observed variables. Items with a communality value of less than 3 were removed to improve the total variance explained. To meet the above criteria, 19 items were dropped from the scale. Communalities of each item obtained from the initial extraction are given in Table 2.
Communalities for Initial 49-item AHRBS.
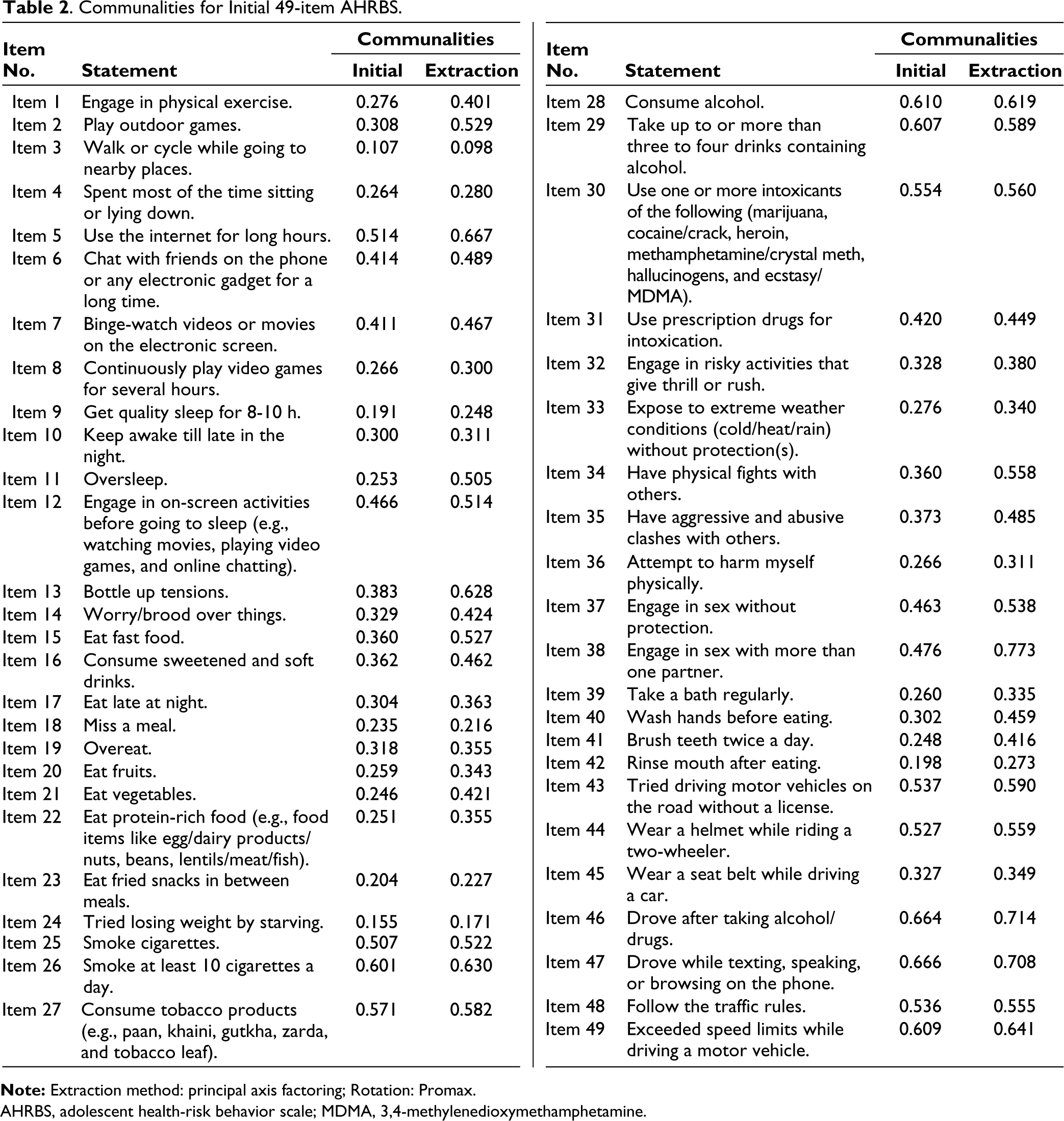
AHRBS, adolescent health-risk behavior scale; MDMA, 3,4-methylenedioxymethamphetamine.
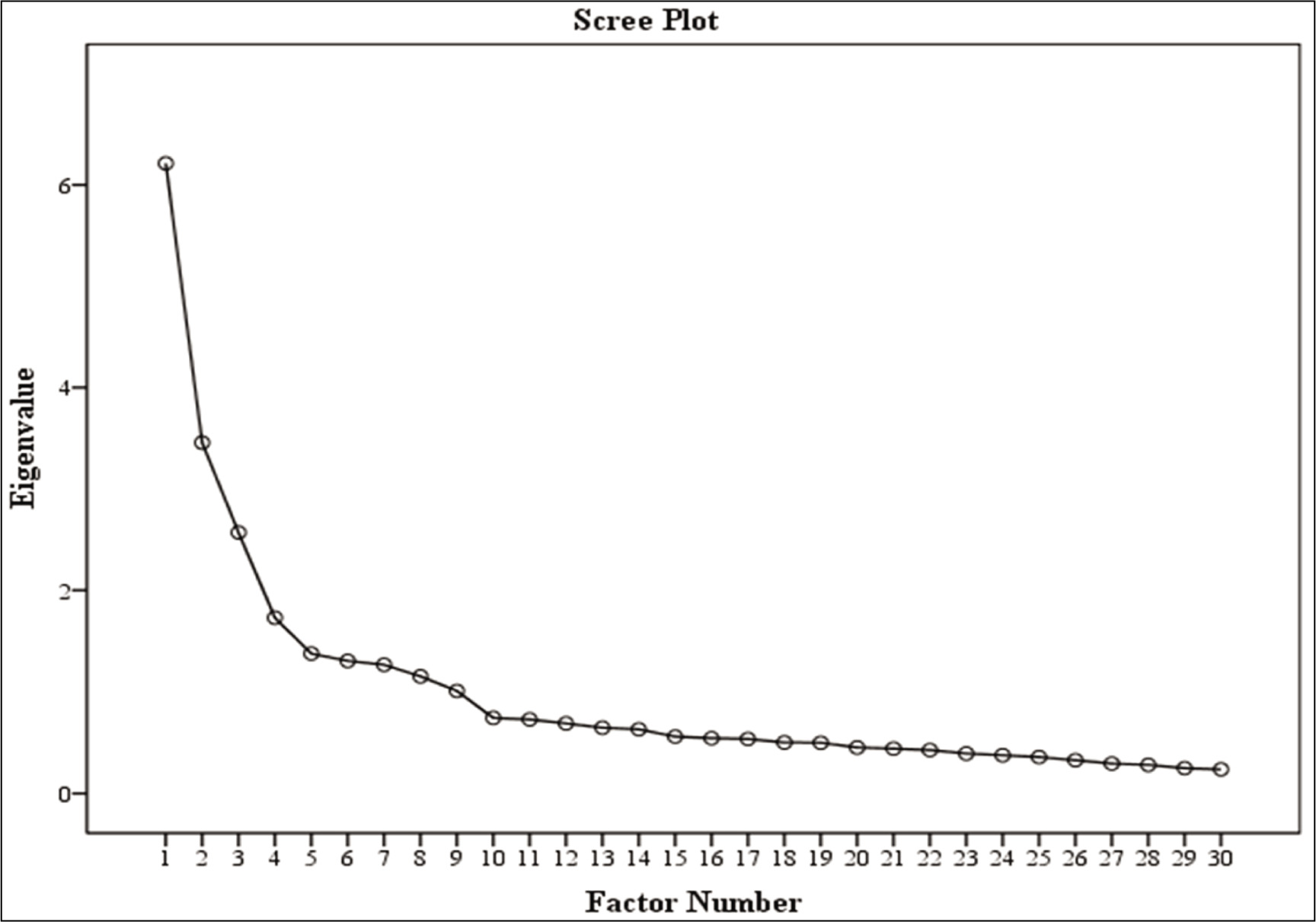
The following three criteria were used to determine the number of retainable factors during EFA: (a) Kaiser’s eigenvalues greater than 1.0 criterion (Table 3), (b) analysis of the scree plot (Figure 1), and (c) factor interpretability. For each factor, items were retained only if they had rotated factor loadings of 0.40 or higher (Table 3). Nine factors emerged, fulfilling all three abovementioned criteria, with a cumulative variance rate of 52.44% (Table 3). Communalities of all the items ranged from 0.33 to 0.70, and the factor loadings ranged from 0.53 to 0.84. Based on the factor loadings, all the items in AHRBS can be interpreted to range from good to excellent. 35
Pattern Matrix of the Nine-factor Solution for AHRBS.
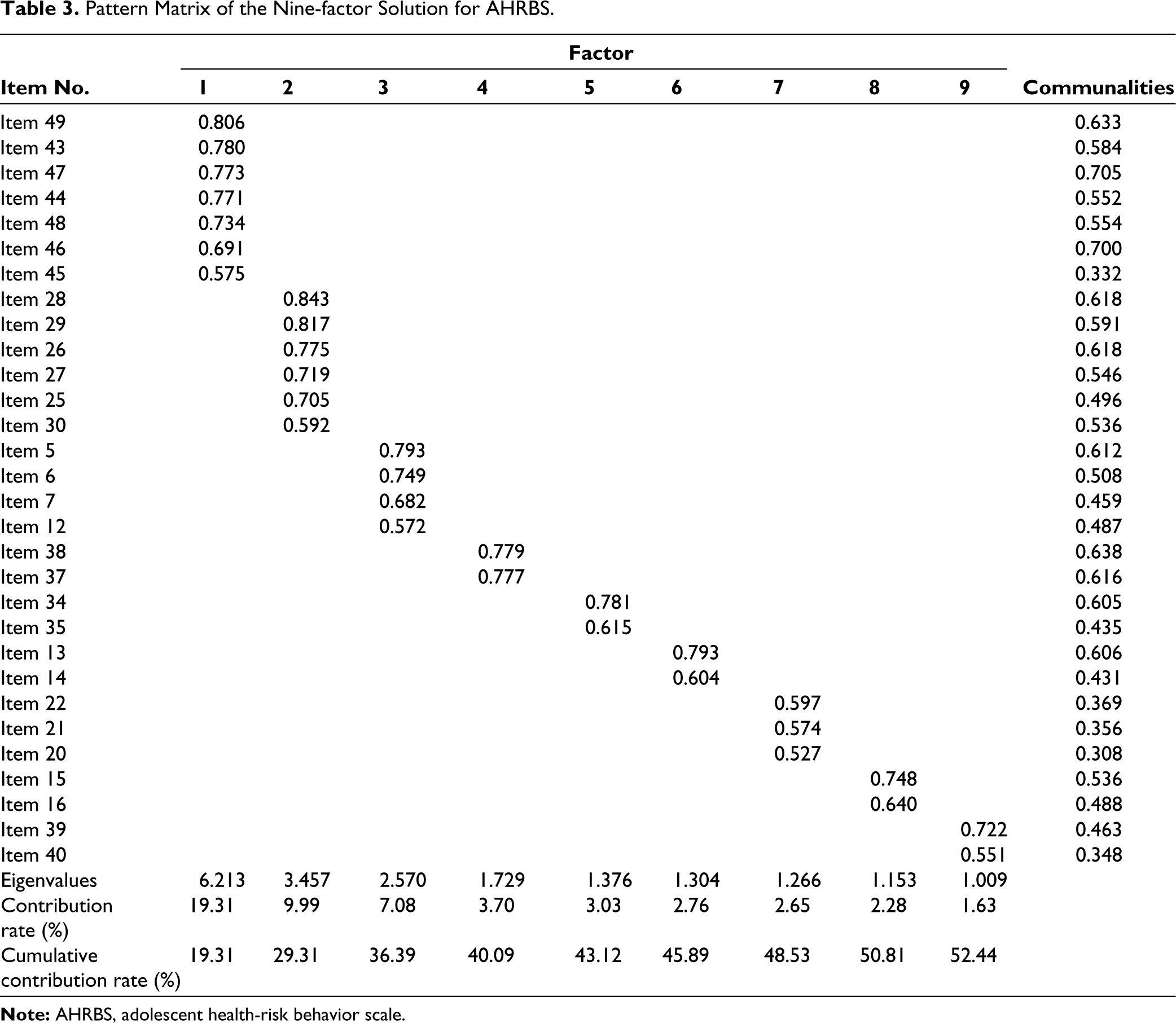
The EFA identified nine distinct factors as significant contributors to HRBs. Factor 1, encompassing seven items (items 49, 43, 47, 44, 48, 46, and 45), was associated with driving behaviors. Factor 2, comprising six items (items 28, 29, 26, 27, 25, and 30), pertained to the consumption of alcohol, nicotine, and other substances. Factor 3, including four items (items 5, 6, 7, and 12), was related to internet usage. Factor 4, with two items (items 38 and 37), addressed risky sexual practices. Factor 5, consisting of two items (items 34 and 35), indicated aggressive behaviors. Factor 6, involving two items (items 13 and 14), related to unhelpful thoughts. Factor 7, containing three items (items 22, 21, and 20), referred to healthy dietary habits. Factor 8, comprising two items (items 15 and 16), focused on unhealthy eating behaviors, and factor 9, with two items (items 39 and 40), related to personal hygiene. The analysis further revealed the percentage of variance each factor contributed to HRBs (Table 3), with factor 1 accounting for 19.31%, factor 2 for 10%, factor 3 for 7.08%, factor 4 for 3.70%, factor 5 for 3.03%, factor 6 for 2.77%, factor 7 for 2.65%, factor 8 for 2.28%, and factor 9 for 1.63%.
Confirmatory Factor Analysis
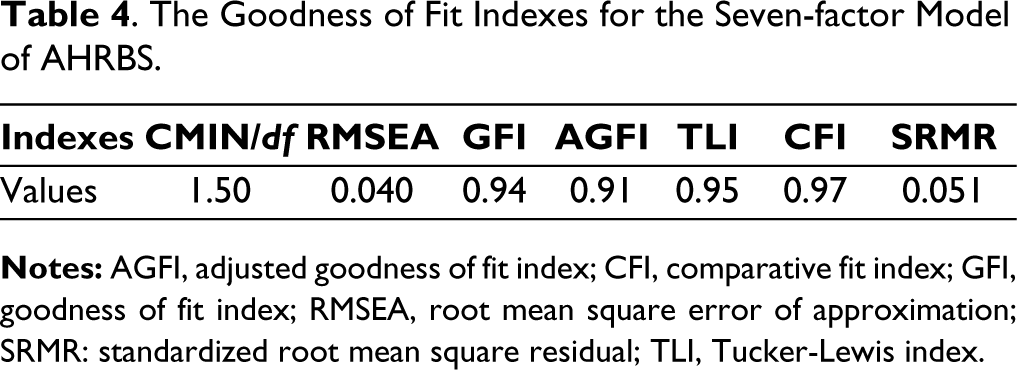
CFA was used to verify the nine-factor structure obtained from EFA. CFA was performed on data from 317 adolescents. The method of maximum likelihood was selected to estimate the model parameters for exploring the association between items and underlying variables. During CFA, 10 items were deleted based on low factor loadings, high standardized residual covariance values, and modification indices, reducing to a 7-factor structure with 20 items. Covariance between error terms was also checked to improve the model fit. The final factor structure was obtained with good model fit indices (CMIN/df = 1.50, GFI = 0.94, AGFI = 0.91, TLI = 0.95, CFI = 0.97, RMSEA = 0.040, and SRMR = 0.051; Table 4).
The Goodness of Fit Indexes for the Seven-factor Model of AHRBS.
The final 20-item AHRBS obtained after CFA comprises seven factors (Figure 2). The first factor, road risk behaviors (F1), consisted of four items (44, 46, 47, and 49), indicating various risky activities individuals engage in while driving vehicles on the road, viz., excessive speeding, mobile phone use while driving, and operating vehicles under the influence of substances (e.g., exceeding speed limits while driving a motor vehicle). Factor 2, named tobacco and alcohol use (F2), consisted of four (25, 27, 28, and 29) items, indicating the usage of alcohol, nicotine, and other substances (e.g., taking up to or more than three to four drinks containing alcohol). The third factor, internet and gadget use (F3), has four items (5, 6, 7, and 12) related to internet usage and screen time (e.g., binge-watch videos or movies on the electronic screen). Factor 4, named sexual risk behaviors (F4), consists of two items (38 and 37) related to protection during intercourse and having multiple sexual partners (e.g., engaging in sex without protection). Factor 5, named aggressive behaviors (F5), consisted of two items (34 and 35) describing verbal and physical abusive behaviors (e.g., having physical fights with others). Factor 6, named negative thought patterns (F6), consisted of two items (13 and 14) related to bottled-up tensions and worrying (e.g., worry/brood over things). Factor 7, unhealthy dietary behaviors (F8), consisted of two items (15 and 16), emphasizing the consumption of fried items, sugar-sweetened beverages, and packaged foods, posing significant health risks for the future (e.g., consuming sweetened and soft drinks).
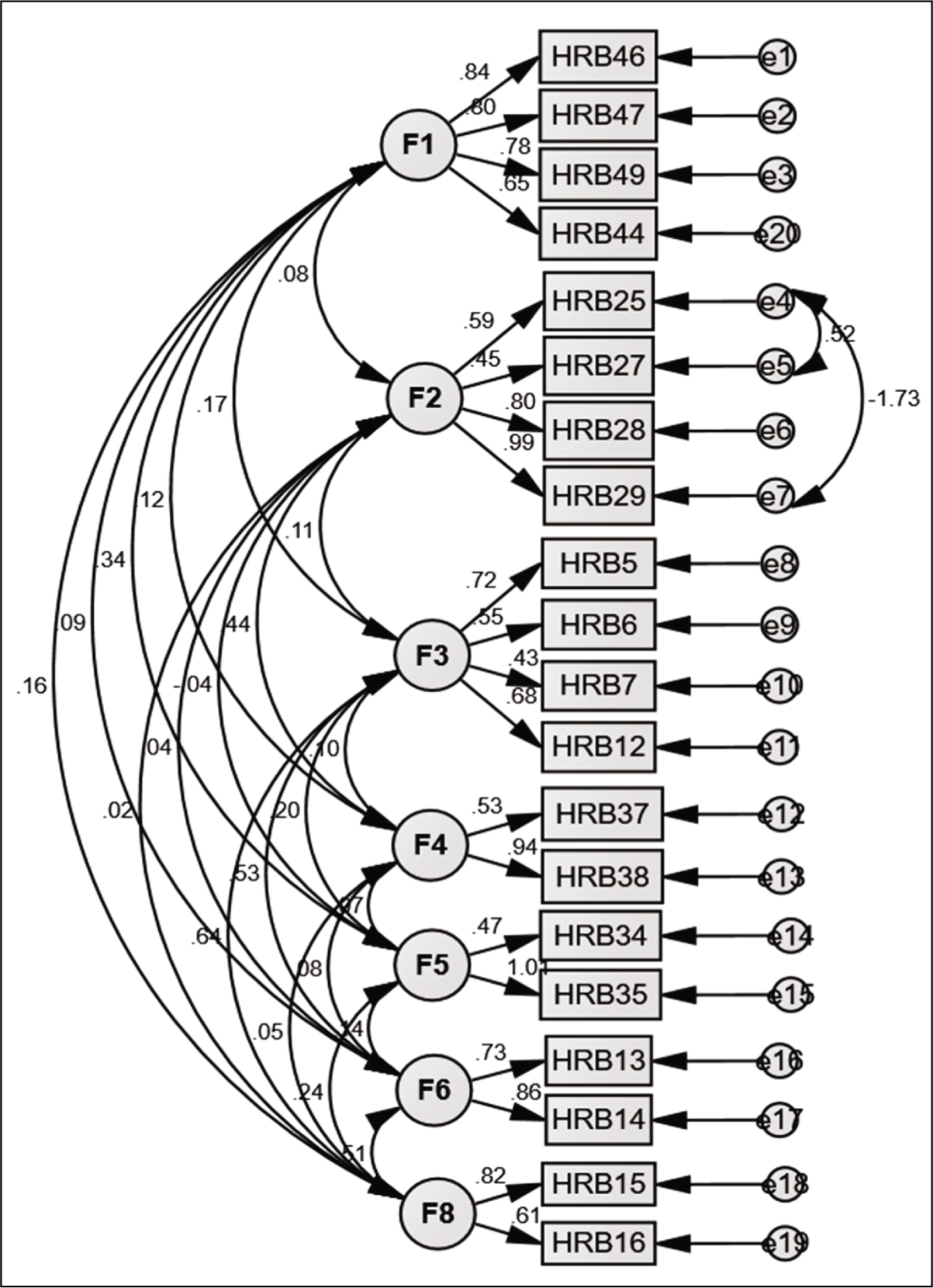
Even though conventional guidelines suggest retaining factors with at least three items for structural validity, 27 the decision to retain four, two-item factors in AHRBS was guided by several considerations. The factors including sexual risk behaviors, aggressive behaviors, negative thought patterns, and unhealthy dietary behaviors were deemed essential to comprehensively represent the construct of HRBs, as highlighted in prior research4,5 and experts’ consultation. Thomas et al. 36 emphasized the importance of retaining factors that align closely with the theoretical framework, even if they are represented by fewer items. Moreover, the robust model fit indices and high factor loadings observed in the CFA further supported this decision. 37 Thus, theoretical relevance and empirical support justified the retention of these factors despite their item count.
Reliability and Validity Testing
Internal Reliability and Test-Retest Reliability
The consistency of results across items within the test was computed using Cronbach’s alpha. The internal consistency of the full scale was α = 0.76, and Cronbach’s alpha for the dimensions ranged from 0.66 to 0.87. Internal consistency for the seven subscales is as follows: road risk behaviors (α = 0.82), tobacco and alcohol use (α = 0.87), internet and gadget use (α = 0.80), sexual risk behaviors (α = 0.66), aggressive behaviors (α = 0.69), negative thought patterns (α = 0.77), and unhealthy dietary behaviors (α = 0.67).
To establish the test-retest reliability, the scale was administered on a subsample of 100 participants (females = 56 and males = 44) after a gap of 2 weeks from the first administration for estimating test-retest reliability. 38 The results indicate good test-retest reliability, with the Pearson correlation coefficient, r = 0.803, P < .01.
Convergent and Divergent Validity
The extent to which AHRBS aligns with other measures of similar constructs was assessed using a revised version of the TSDS and BIS-15. AHRBS was positively correlated with TSDS (r = 0.35, P < .01) and BIS-15 (r = 0.27, P < .01), indicating significant convergent validity.
The divergent validity of AHRBS was assessed through the HLBS. HLBS was negatively correlated (r = −0.18, P < .01) with AHRBS, indicating significant divergent validity.
Discussion
The objective of this study was to develop a scale to assess HRBs among adolescents with sound psychometric properties. The 20-item AHRBS is notably concise, easy to comprehend, and designed for individual and group administration. Its effectiveness is underscored by its comprehensive approach to evaluating a broad spectrum of adolescent health risks, which recent studies have identified as significantly prevalent.11,21,39-42 The AHRBS efficiently captures a wide range of risky behaviors, including road risk behaviors, tobacco and alcohol use, internet and gadget use, sexual risk behaviors, aggressive behaviors, negative thought patterns, and unhealthy dietary behaviors, making it a powerful tool for HRB assessment.
All the 20 items of the scale demonstrated conceptual clarity and efficacy in measuring HRBs. This can be attributed to the extensive literature review, adolescents’ feedback on the initial pool of items, and content validation by experts. The simplicity in the language and ease of comprehension of the scale is highlighted by the higher percentage of retained data (98%), where participants could respond to the items without fatigue. The scale has established good test-retest reliability and internal consistency. AHRBS exhibited a positive correlation with self-destructiveness and impulsiveness and a negative correlation with healthy lifestyle beliefs, affirming the scale’s convergent and divergent validity, respectively.
The AHRBS addresses the limitations of the two widely used tools by providing uniform response cues, which facilitates advanced statistical analysis. Furthermore, the scale incorporates certain HRBs not covered by other scales, such as road risk behaviors and internet and gadget use,16-19 enhancing its utility for assessing these risk behaviors among adolescents.
Though most of the HRBs across the adolescent age group have significantly emerged under different domains during the factor analysis, it was observed that some important factors, viz., sedentary behaviors, sleep hygiene, and personal hygiene, were removed during the factor analysis (EFA and CFA). The exclusion of such factors may indicate that adolescents place minimal emphasis on these behaviors. Interactions during data collection suggest a lack of discipline among adolescents when it comes to engaging in physical activities amidst their demanding academic schedules. Moreover, their limited leisure time is predominantly spent on the internet and various digital devices, often at the expense of adequate sleep. Future studies can explore the underlying reasons for the exclusion of these behaviors.
Additionally, the explicit nature of questions in AHRBS may make it vulnerable to social desirability bias, which may be one of the limitations of the scale. Furthermore, data for the scale were collected only from school- or college-going adolescents who can read and comprehend the items written in English, which excludes the students who cannot read or write and the lower strata of the population. Administering and validating the scale on apparently healthy adolescents from schools poses another limitation in deriving cut-off values for mild/moderate/severe risks. Future studies can address this limitation by administering the scale to the clinical population.
Despite the abovementioned scale-related and sample-related limitations, the final scale achieved good reliability-validity estimations and specified structure. To establish a range of psychometric qualities for this scale, its use in clinical practice, educational settings, and research is highly encouraged. Appendix A (as a Supplementary Material) contains the final scale and scoring information. Future researchers from diverse cultures are advised to adapt the scale in light of the pilot items for a culturally appropriate measure.
Supplementary Material
The supplementary material for this article is available online.
Footnotes
Acknowledgements
The authors are sincerely grateful to Dr. Murugan Pattusamy, Assistant Professor, School of Management Studies, University of Hyderabad, for his insightful statistical guidance.
Author Note
Dr. Usha Chivukula and Aysha Thasleema are co-first authors and have contributed equally to the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of the University. The study followed the principles enunciated in the Declaration of Helsinki (Letter number: UH/IEC/2022/337).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent was obtained from all participants aged 18 and above. Written informed assent was obtained from participants aged under 18 years.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.