
Abstract
Background:
Adolescents often struggle with social, emotional, and behavioral difficulties that can lead to functional impairment later in life. School-going children are at risk of bullying victimization at school, which can lead to social, emotional, and behavioral difficulties (SEBD). This study aimed to estimate the burden of SEBD, evaluate possible risk factors, and explore the correlation between bullying victimization and SEBD.
Methods:
A cross-sectional study was done among 9th to 12th class students from July 2021 to June 2022. Strengths and Difficulties Questionnaire (SDQ) was utilized to evaluate SEBD. Bullying victimization was assessed by “Adolescent peer relation instrument” (APRI). Chi square test, t-test, pearson correlation, and logistic regression was used.
Results:
Out of 391 participants, 35.3% faced peer problems, 22.2% conduct problems, 16.4% hyperactivity, and 15.6% emotional symptoms. Prosocial behavior was present in only 12.7% of adolescents. 70.8% bullied others and 62.9% were victims in the past 1 year. The victims were at increased risk for emotional symptoms, conduct problems, hyperactivity, and peer problems. Social perpetrators were at risk for emotional symptoms, conduct problems, hyperactivity, and peer problems; verbal and physical perpetrators were prone to conduct problems and hyperactivity. Higher emotional problems and prosocial behavior were reported among girls; higher conduct problems, peer problems, and hyperactivity were reported among boys. Hyperactivity was significantly more prevalent in students with poor performance. Emotional symptoms, conduct problems, hyperactivity, and peer problems were positively correlated with bullying and victimization, but negatively correlated to prosocial behavior.
Conclusions:
The burden of SEBD and bullying is high among school-going adolescents. Bullying and gender are significant risk factors for social, emotional, and behavioral difficulties. It also impacts the academic performance of the student. Anti-bullying interventional programs, cognitive behavior therapy, and parent management training programs for parents at school should be implemented universally at school to control these problems effectively.
Keywords
Introduction
The highest prevalence of psychiatric disorders across the human lifespan is in adolescents, who often struggle with social, emotional, and behavioral difficulties (SEBD). 1 SEBD can significantly impact adolescents’ lives, causing functional impairment in their relationships, family dynamics, peer interactions, and educational achievements. 2 According to a meta-analysis study, prevalence of emotional and behavioral problems were in 6.5% of community adolescents and 23.3% of school-going adolescents. 3 Various studies from around the globe have depicted mental health problems in 10.3%-26% of adolescents.4–7 According to research from 41 studies conducted in 27 countries, 13.4% of adolescents experience mental health issues. 8
Bullying is a significant problem due to its consequences on mental health,9–14 social relationships,14,15 school performance,12–14,16,17 and school absenteeism, 18 and it is also a risk factor for suicide attempts.19,20 Emotional Intelligence (EI) is associated with less bullying, that is, adolescents who were less involved in bullying, either as aggressors or victims, have higher EI scores. 21 Both bullies and victims lack adequate emotional management or regulation skills. 21 Victims and bullies/victims have elevated rates of young adult psychiatric disorders.16,22 The risk of school bullying (bullies, victims, or bullies/victims) is higher among students who experience mental health issues like anxiety, self-injury (non-suicidal), and suicide ideation. 10 Adolescent depression and suicidality are potential consequences of victimization and bullying. 23
Many studies from different countries reveal that difficulties in socializing with their peers, conduct-related problems, peer relationship problems, and psychosomatic issues were increased in students who were involved in bullying as perpetrators, victims, or both.24–27 Some studies were conducted about bullying and mental health more than five years ago in this country. Still, there is a paucity of data regarding the association of bullying victimization with the emotional and behavioral aspects of mental health in adolescents going to school. SEBD can lead to functional impairment later in life, so this study was planned to estimate the burden of SEBD in adolescents going to school. Another objective was to find the association of bullying victimization with social, emotional, and behavioral difficulties. The third objective was to evaluate the possible risk factors for mental health issues among them and, further, to find the correlation between different aspects of bullying victimization and the emotional and behavioral aspects of mental health.
Methodology
Study Design
A school-based, cross-sectional study was conducted among senior secondary schools (both government and private) in urban Rohtak, Haryana, India. The sample was collected with instructions and a questionnaire administered in Hindi language between July 2021 and June 2022.
Study Setting and Participants
The study population comprised school-going adolescents studying in class 9th to class 12th. The sample size was calculated by referencing a study done by Patel et al. in 2017. 28 The prevalence of bullying was 49%, with an absolute error of 5% and a confidence level of 95%; the calculated sample size was 384. The students with chronic systemic illness and with mental conditions like developmental disorders, specific learning disorders, attention‑deficit hyperactive disorder, impaired sensory functions, and neurological disorders were not included in the study as they will not be able to give the answers properly and the quality of data can be compromised. The details of these conditions were asked by the principal/teacher and they were communicated to us after seeing the school records.
Instrumentation
Adolescent peer relation instrument (APRI) is a self-reported questionnaire consisting of 36 items that helps to measure 3 subscales of perpetrators (physical, verbal, and social) and 3 subtypes of victims (physical, verbal, and social). 29 To generate scores on subdomains, the scale considers information from the past year and assesses it ranging from “never” to “every day” (six-point Likert scale). A score less than 36 (or 18 on each subscale) is classified as never been bullied by others or never bullied others in the past. The instrument’s internal consistency is good, with Cronbach’s alpha value of 0.93 for a total bully score, 0.95 for the total victim score, and 0.83 to 0.92 for subscale scores.29–31 The Hindi version of this instrument was used. 32
The strengths and difficulties questionnaire (SDQ), self-reported version, which is widely used in Indian studies, was utilized to evaluate the emotional and behavioral difficulties. 33 This scale consists of 25 items, with scores ranging from 0 to 2 (0: false, 1: somewhat true, and 2: definitely true). The tool measures five subscales: conduct-related issues, emotional symptoms, hyperactivity-inattention, peer relationship issues, and prosocial behavior. The higher score on each subscale denotes higher concerned mental health problems, except for the prosocial scale.
Procedure
The list of senior secondary schools (both government and private) was obtained from the district administration of the Education Department in Rohtak. There were 68 private higher schools and 21 government higher schools in the urban area of District Rohtak, Haryana. The lottery method randomly selected two government and two private senior secondary schools from this list. Permission was taken from the principals of the selected schools to conduct the study, and the day for sample collection was decided. Before the sample collection day, the consent form was sent along with the students to take the consent from their parents for the study. The students who gave assent and whose parent’s gave consent were included in the study. The students with chronic systemic illness and with mental conditions like developmental disorders, specific learning disorders, attention‑deficit hyperactive disorder, impaired sensory functions, and neurological disorders were not included in the study. The selected students from each class were assembled in separate classrooms. The study participants were given a pre-tested, semi-structured questionnaire to complete their responses. Four investigators were present in each class (class 9, 10, 11, 12) with the students to facilitate them to fill the responses. The candidate recorded the responses.
Data Analysis
Data analysis was done by using Statistical Package for Social Sciences (SPSS 24) software. The quantitative descriptive analysis used univariate statistics to report frequency distribution as percentages. For inferential statistics, chi-square and t-tests were conducted using 95% confidence interval (CI). Multivariable logistic regression was performed for variables with a P value of <.25. The strength of the association was measured by calculating the odds ratio with 95% CI. Cross-scale correlation was performed to assess the correlation between mental health and bullying victimization subscales.
Ethics
Ethics approval was obtained from the Ethical Research Committee of the institute. Written permission was obtained from the District Administration, Education Department of District Rohtak and selected schools’ principals, and written informed consent was obtained from the parents of the study participants and study participants themselves.
Results
Participants Characteristics
The study included 391 participants, of which 58.1% (n = 227) were from private schools and 41.9% (n = 164) were from government schools. The study participants’ mean age was 15.36 ± 1.3; 56.8% (n = 222) were male, and 43.2% (n = 169) were female; 28.4% (n = 111) were from 9th class, 22.5% (n = 88) from 10th class, 22.3% (n = 87) from 11th class, and 26.9% (n = 105) from 12th class. Out of the total participants, 18.4% (n = 72) belonged to upper socioeconomic status, 12.3% (n = 48) to upper-middle socioeconomic status, 9.7% (n = 38) to middle socioeconomic status, 8.4% (n = 33) to lower middle socioeconomic status, and 4.3% (n = 17) to lower socioeconomic status.
Prevalence of Bullying and Victimization
According to the study, 70.8% (n = 277) of students agreed that they had intentionally inflicted one or other types of harm on others in the past year, and 62.9% (n = 246) agreed that they were affected by bullying by others in the past year.
Bullying and Victimization as Risk Factors for Emotional and Social Problems
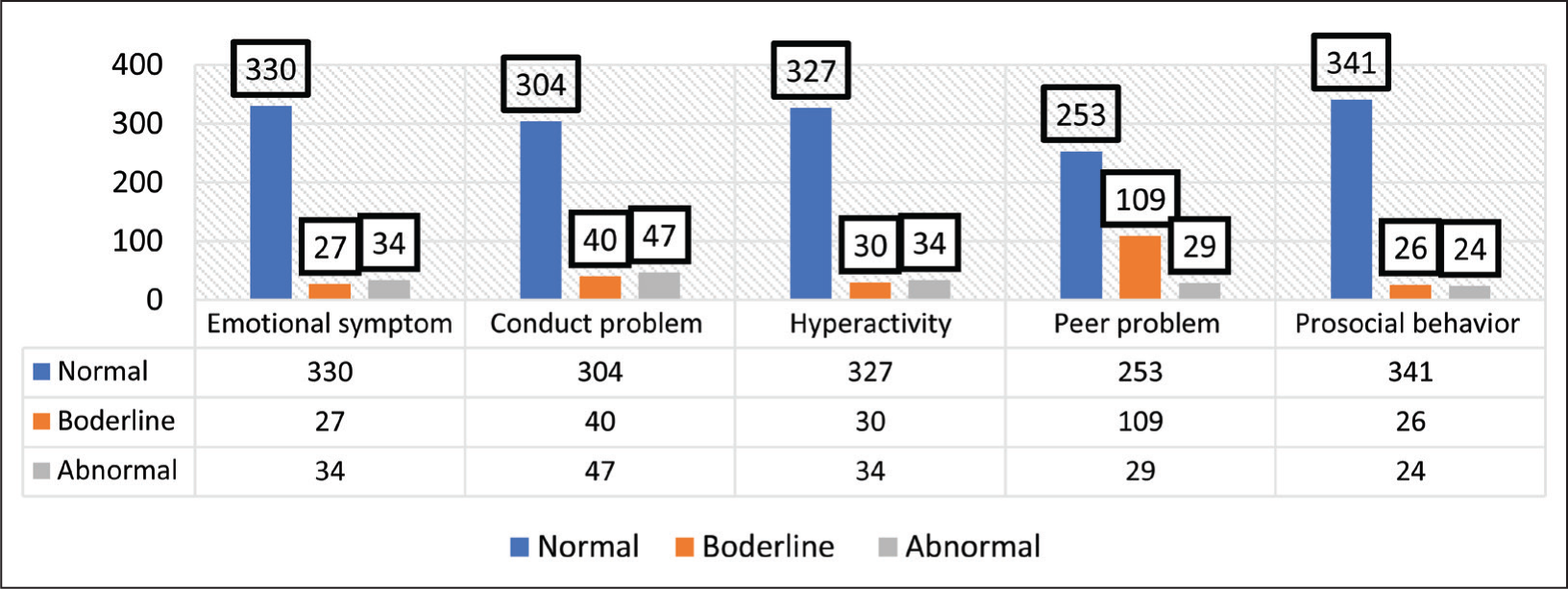
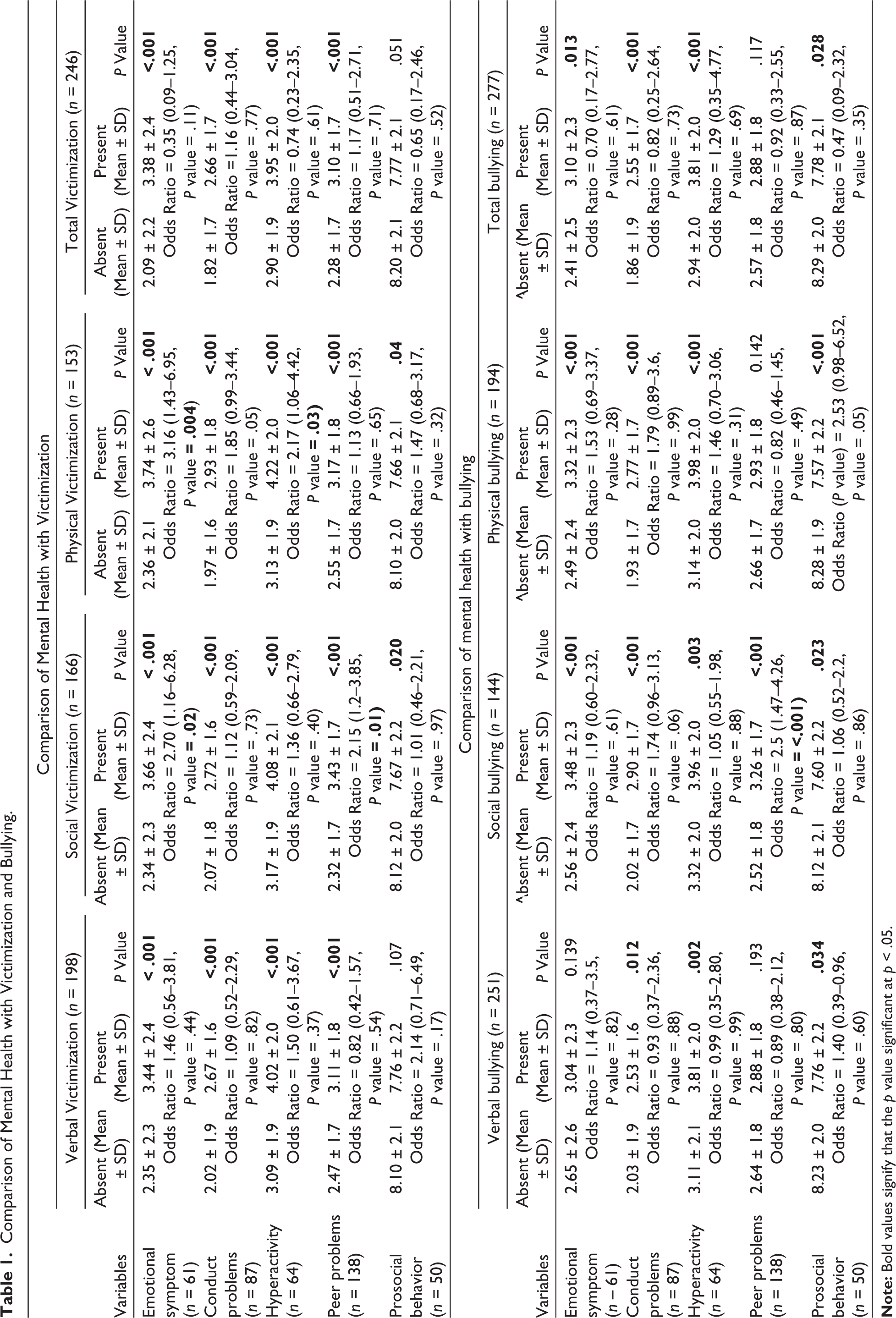
It was observed that 35.3% of adolescent participants were facing peer problems, followed by conduct problems (22.2%), hyperactivity (16.4%), and emotional symptoms (15.6%). Prosocial behavior was present in only 12.7% of adolescents (Figure 1). The victimized adolescents were at more risk of mental health problems than non-victimized students, particularly emotional symptoms for social and physical victims, hyperactivity for physical victims, and peer problems for social victims. Those bullying others were also at risk of mental health problems, particularly social bullying to peer problems. The mean value of prosocial behavior was more among non-victimized people and those who never bullied others in the last year. Table 1 depicts the association of different types of victimization and bullying with adolescent students’ mental health and their strength of association.
Prevalence of Mental Health Issues.
Comparison of Mental Health with Victimization and Bullying.
Other Risk Factors for Mental Health Problems
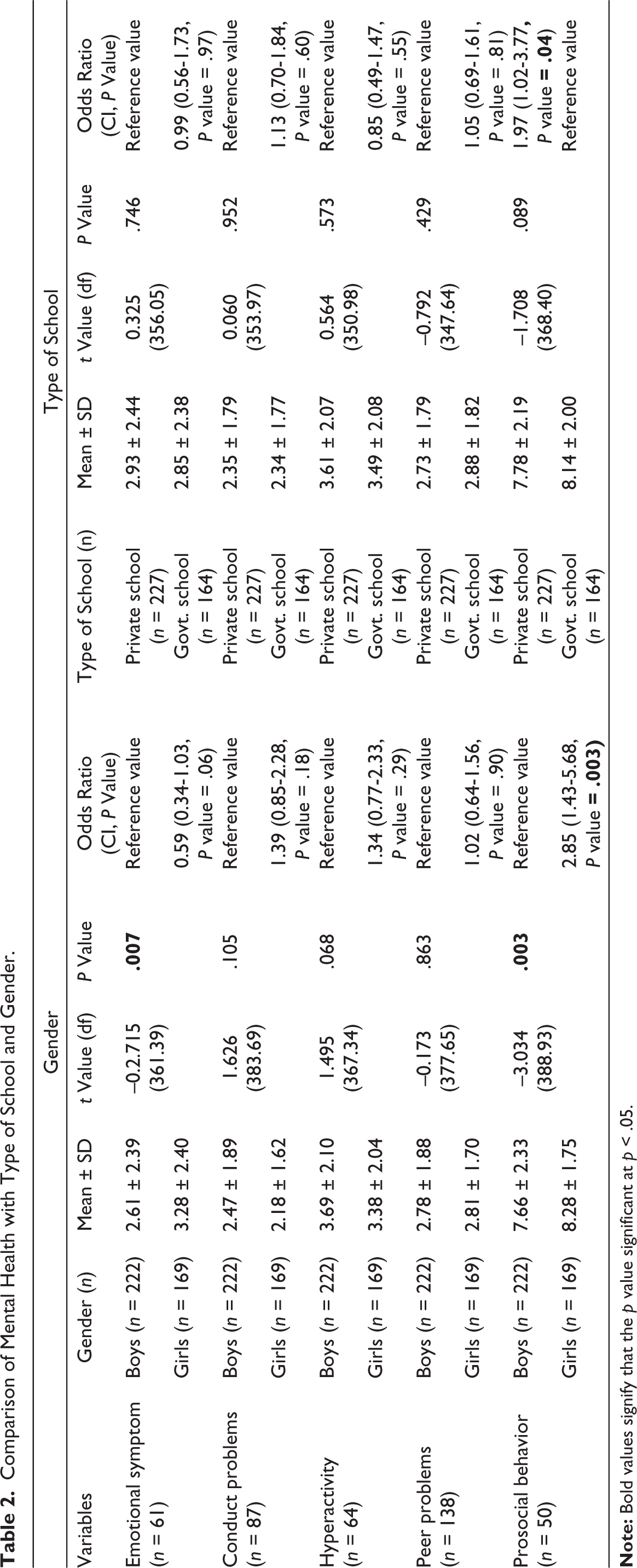
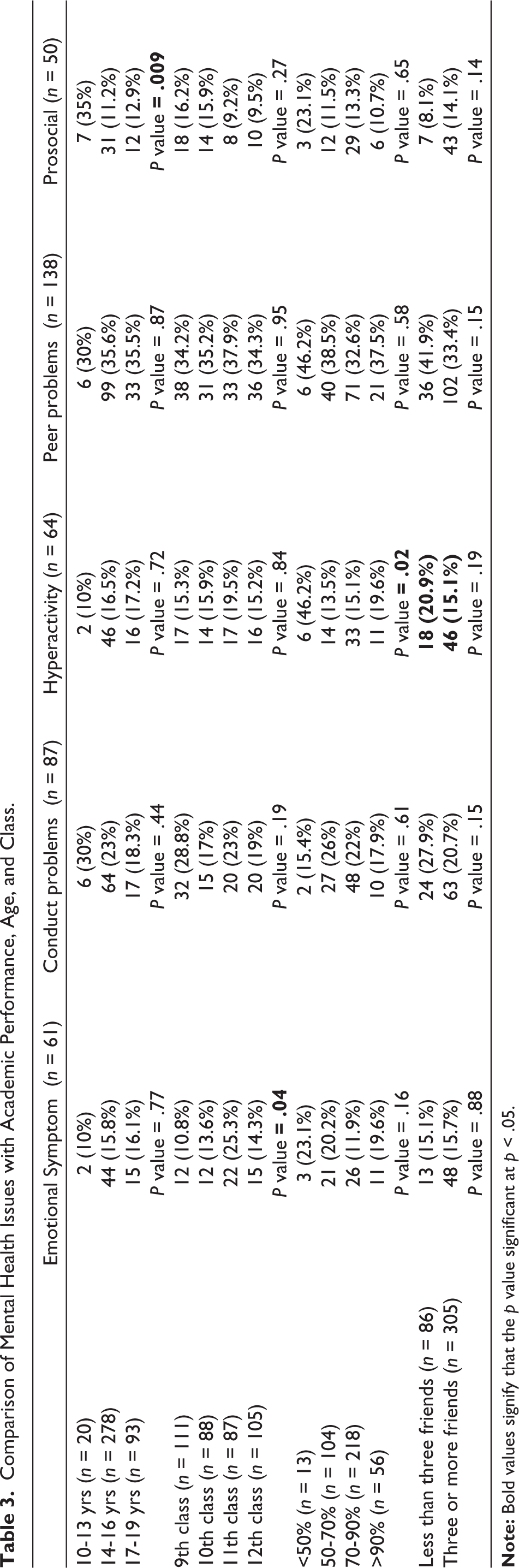
As depicted in Table 2, gender was significantly associated with emotional symptoms and prosocial behavior. The mental health status of adolescents was not influenced by the type of school, and all the parameters were non-significant. Prosocial behavior was 2.85 times more in girls and 1.97 times more in private school students. The association of age, class, and student’s academic performance is shown in Table 3. It was observed that social victimization and emotional problems were significantly more in 11th-class students. Hyperactivity was considerably more in students with poor performance, with less than 50% marks obtained.
Comparison of Mental Health with Type of School and Gender.
Comparison of Mental Health Issues with Academic Performance, Age, and Class.
Correlation Between Bullying, Peer Victimization and Mental Health Issues
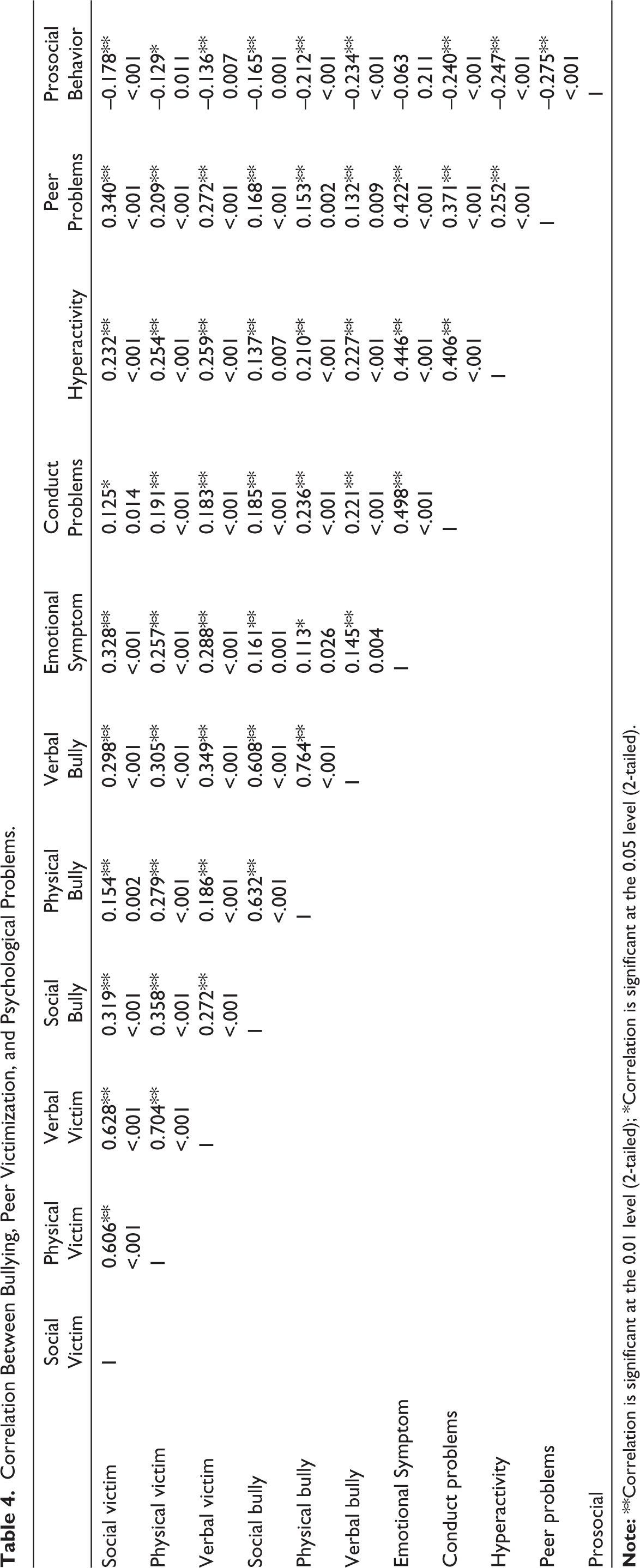
Table 4 depicted that emotional symptom, conduct problems, hyperactivity, and peer problems were positively correlated with bullying and victimization, but prosocial behavior was negatively correlated. A high positive correlation was observed between physical bullying and verbal bullying. There was a moderate positive correlation between a social victim with a physical victim and a verbal victim, a physical victim with a verbal victim, a social bully with a physical bully, and a verbal bully. A low positive correlation was found for the social victim with a social bully, emotional symptom, and peer problem; for the physical victim with a social bully and verbal bully; for the verbal victim with a verbal bully; for emotional symptom with conduct problems, hyperactivity, and peer problems; and for conduct issues with hyperactivity and peer problems.
Correlation Between Bullying, Peer Victimization, and Psychological Problems.
Discussion
Burden of Social, Emotional and Behavior Difficulties Among Adolescents Going to School
The current study depicted that 8.7% of adolescents had emotional symptoms, 12% had conduct problems, 8.7% had hyperactivity, 7.4% had peer problems, and 6.1% had low prosocial behavior. The findings were similar to studies done in Kerala 4 and Gujarat. 5 They were different to research done in Bengaluru, India, 26 where significant emotional problems were found in 10.5%, conduct issues in 20.3%, hyperactivity‑inattention in 6.2%, peer problems in 16.9%, and low prosocial behaviors in 5.7% of study participants. The study done at Nagaland, 6 India, depicted highly abnormal emotional problems (17.1%), hyperactivity (16.1%), and conduct problems (15.2%) in comparison to our study. The differences may be due to geographical, cultural, and behavioral differences across the country. One study done in Iran 7 revealed that the youth screened for conduct disorder were 34.7%, peer relationship problems were 25.4%, emotional problems were 24.5%, hyperactivity was 23%, and impairment of prosocial behavior was 5.7%.
Bullying Victimization Among Adolescents Going to School
The current study was done to discover the association of bullying and victimization with social, emotional, and behavioral difficulties, with 70.8% of students who bullied others and 62.9% being victims. The studies done in India by Gujrat (2017) 28 and Bengaluru (2019) 26 reported bullying at 49% and 97.1%, and victims at 29.7% and 97.9%, respectively. According to United Nations Educational, Scientific and Cultural Organization (UNESCO), 2019 report, 34 in the preceding month, nearly 32% of children had been bullied on one or more days and 7.3% had been bullied on six or more days. Globally, there is a huge differences region-wise in the prevalence of children being victimized, ranging from 22.8% in Central America to 48.2% in sub-Saharan Africa, with Europe and North America having rates of 25.0% and 31.7%, respectively. 12 The variation in prevalence may be due to geographic variation in the behavior of students, variations in discipline and regulations for students at schools, and the nature of tools used to assess bullying.
Bullying and Victimization as Risk Factors for Mental Health Problems
This study depicted that bullying and victimization were risk factors for emotional and behavioral problems. Similarly, Patel et al. (2017) 28 in their study concluded that victimized students have increased problems in peer relationships, higher emotional problems, and higher activity compared to non-victim students. Perpetrators have higher conduct problems, hyperactivity, and lower scores on prosocial behavior than the non-bully group. A study conducted in Italy by Ginni et al. (2008) 27 found that victims of bullying are at a higher risk of developing conduct-related issues, hyperactivity, and issues with peers, while bullies are more likely to develop hyperactivity. In addition, a study in Bengaluru found that emotional and conduct-related issues and increased activity behavior were significantly related to bullying. In contrast, bullying had inverse relation with prosocial behaviors. 26 Another study revealed that self-esteem was lesser in aggressive students and those who were victims of bullying at school. These students were prone to higher depressive symptoms and higher psychological problems. 35 Bullies are at higher risk for hyperactivity, conduct problems, and low prosocial behaviors. 36 The study’s result is concordant to many other studies done before with results showing a positive correlation of behavioral problems with bullying.37–39 These results are closer to one meta-analysis 40 which found that bullied adolescents are likelier to experience psychosomatic and internalizing problems than non-bullied adolescents.
Other Risk Factors for Social, Emotional and Behavior Difficulties
Emotional problems and prosocial behavior were higher in girls in the current study. Conduct problems and hyperactivity was 1.39 times and 1.34 times more in boys than in girls. The finding was similar to a meta-analysis comparing the data of different countries like the UK, Australia, China, and South Africa, which found that emotional problems and prosocial behavior was significantly more in girls. 41 On the contrary, conduct problems and hyperactivity were significantly more in boys. 41 Two studies conducted in South India and Gujarat also depicted the same results as the present study.4,5 Our study showed that hyperactivity was significantly more in students with poor academic performance (marks <50%). Similarly, academic performance and interpersonal relationships were significantly impaired in adolescents with persistent ADHD. 42 The study done in the USA depicted that academic performance and psychological problems were higher in youth who experienced multiple victimizations. 43 In the present study, conduct problems, hyperactivity, and peer problems were more common in those with fewer friends; in contrast, prosocial behavior was more common among those with more friends. A study by Nair et al. revealed that having friends decreased the odds of a high SDQ score. 5
A meta-analysis done by Gaffney, Ttofi, and Farrington in the year 2019 44 found that approximately 19%-20% school-bullying perpetration and about 15%-16% school-bullying victimization were reduced by anti-bullying intervention programs. The updated meta-analysis by Gaffney, Ttofi, and Farrington (2021) 45 showed that the burden of bullying victimization was effectively reduced by two components: informal peer involvement and information provided for parents. Only bullying perpetration was reduced effectively by components like anti-bullying policies, a whole-school approach, classroom rules, and work with victims. Another interventional study was done in the Republic of Ireland in 2012 2 on adolescents with social, behavioral, and emotional problems, and the parents of those children found that parent-rated child total difficulties, parent-rated child conduct difficulties, adolescent-rated emotional difficulties, and parental stress and satisfaction significantly improved with a five-month follow-up after the intervention. The intervention was a combination of cognitive behavior therapy (CBT) and parent management training (PMT), namely, Working Things Out (WTO), the adolescent program, and the Parents Plus Adolescent Programme’ (PPAP). The WTO program supports overcoming specific health problems by highlighting the connection between thoughts, feelings, and actions; thus, it helps in promoting positive mental health. For building good relationships with teenagers, a solution-focused positive parent training program for parents of children aged 11-16 years (PPAP) can be approached where parents are taught about parenting skills and techniques. These types of interventions can be implemented in every school in our country in order to decrease the burden of psychiatric disorders in adolescents across their lifespan, who often struggle with SEBD.
The limitation of the study was that the other risk factors for mental health issues like parental bonding, family conditions, and rearing of child at home and at schools by teachers were not considered. Apart from physical, verbal, and social bullying, cyberbullying is also an important aspect for mental health, which was not considered here. Another limitation was that urban area schools were not included in the study. Socioeconomic status could not be assessed as students may not be fully aware of their family income status. Further studies can be conducted to address these issues.
Conclusion
The study concludes that there is an increased burden of SEBD among school-going adolescents and an increased prevalence of bullying victimization at schools, irrespective of type of school. The second observation was that bullying victimization and gender are significant risk factors for SEBD. The burden of mental health problems and bullying victimization has not decreased over the years in the country. Various studies in different countries have highlighted the importance of anti-bullying interventional programs, cognitive behavior therapy for students with SEBD, and parent management training programs for parents that effectively control these problems. Though the mental health guidelines have been formed, they lag behind on formation of school-specific policy and also the proper implementation of formed policies. As mentally sound adolescents are the successful future adults in society, we recommend that the government should revise its mental health policy by inculcating anti-bullying programs, parent management training programs, and cognitive behavior therapy with the help of trained psychologist appointments, in all schools irrespective of whether it is government or private school, along with its mandatory implementation at school-level. Further interventional studies can be planned in the future to appreciate the effect of anti-bullying interventional programs, cognitive behavior therapy for students with SEBD, and parent management training programs for parents in our country.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability
It will be provided by the corresponding author if requested.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The research was approved by the Institutional Ethics Board under Ethics Committee No. BREC/20/182, dated 30.09.2020. Written and verbal informed consent was obtained from all study subjects. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.