
Abstract
Trauma-focused cognitive behavioral therapy (TF-CBT) is an efficacious treatment for trauma-related symptoms in children and adolescents. It is found to be effective for symptoms of post-traumatic stress disorder (PTSD), depression, sexually inappropriate behavior, externalizing symptoms, dissociative symptoms, fear, and anxiety in sexually abused children. Here, we present a case report that describes the psychotherapeutic management of a 13-year-old girl who was sexually abused and subsequently developed symptoms of PTSD, depression, and anxiety. TF-CBT was employed for the management of trauma-related symptoms. The post-therapy assessment showed a reduction in symptoms of PTSD, depression, and anxiety, indicating the utility of TF-CBT in treating trauma-related symptoms in children.
Introduction
Child sexual abuse (CSA) is a ubiquitous social and public health problem that adversely affects children’s mental health. 1 CSA is prevalent globally as studies indicate a prevalence of 8%-31% for girls and 3%-17% for boys. 2 In India, 53.22³% of children are reported to have experienced one or more types of sexual abuse. 3 Studies that examined the impact of sexual abuse in Indian children found the presence of depression, anxiety, and low self-esteem in child victims, 4 high risks for obsessive-compulsive disorder, temperamental issues, poor social adjustment, lack of trust, insecure relations with parents, low academic performance, sexual risk behaviors, and sexually-transmitted diseases. 5
Research shows that victimized children are susceptible to physical, emotional, behavioral, cognitive, and interpersonal issues. The short-term or long-term effects of CSA are determined by factors like the child’s developmental level, duration of abuse, the severity of abuse, intra-familial or extra-familial abuse, and use of force or physical injury in abuse. The presence of multiple types of abuse, lack of social support, and negative appraisal by the victim also influence the development of symptoms. 6
Empirical research suggests that trauma-focused cognitive behavioral therapy (TF-CBT) is the most effective and widely disseminated therapy for CSA victims with trauma-related symptomatology. 7 Developed by Esther Deblinger, Judith Cohen, and Anthony Mannarino to address post-traumatic stress disorder (PTSD) symptoms in sexually abused children, TF-CBT is a manualized treatment program for children aged 3-18. It is provided either individually or with non-offending parents and is usually delivered in 12-20 sessions. Its components include psychoeducation and parent skills training, relaxation training, affective expression and modulation, cognitive coping, trauma narrative development and processing, in vivo exposure, conjoint parent-child sessions, and enhancing personal safety and future development (acronym PRACTICE). 8
The following case is part of a preliminary research study to examine the effectiveness of TF-CBT in reducing symptoms related to PTSD, depression, and anxiety in adolescents who experienced sexual abuse. Informed consent from the parent (mother) and assent from the child was obtained for assessment, therapy, and publication.
Sufficient and essential information relating to the research study (assessment, course of treatment, and termination) was provided to the accompanying parent and the child. It was ensured that information was comprehended by the parent and child. They were informed about the voluntariness of participation and the risk associated with revisiting traumatic experiences. Privacy and confidentiality were ensured.
Case Description
Divya (name changed), a 13-year-old girl studying in 8th standard, from a low socio-economic level, urban background in Western India, presented with recurrent memories of an experience of sexual abuse followed by complaints of feelings of sadness, inability to concentrate on studies, feelings of worthlessness and helplessness, worry about the outcome of ongoing judicial trial related to abuse, fear of being revictimized by the perpetrator, anger outbursts and decreased appetite for the past 1½ years. Divya was observed to be anxious and had thoughts characterized by shame and self-blame. She was aware that all the difficulties she was facing were due to her abusive experience and reported that she needed help for her problems.
Divya was functioning well till 11½ years of age when she was sexually abused by a middle-aged married man living in the neighborhood. She was called to his house on the pretext of buying some groceries for him from a nearby store. The act involved fondling her while encouraging her to do the same to the perpetrator. Though shocked and confused at first, she gathered the courage to resist the advance and escape to the house of an extended family member who lived nearby. The matter was disclosed to the parents immediately, who reported the crime to the police and the perpetrator was arrested. In the following days, Divya showed excessive fear of the perpetrator; her sleep and appetite decreased, she was irritable, and feared going outside the house. Her mother reported that difficulties lasted for about a month and gradually reduced in severity as she was adequately supported by her parents and extended family members.
During the evaluation, approximately 1½ years after the traumatic event, the child reported recurrent memories about the traumatic event, after which she felt uneasy and sad, shameful about being part of the act, and guilty of embarrassing the family. She reported that she had become an unworthy person, dirty and damaged before others, and regretted not being able to prevent the act from occurring. Thoughts about the trauma and subsequent feelings affected Divya’s academics. As a result of her declining performance in academics, her mother started controlling her excessively and demanded good performance in exams, which led to frequent conflicts between Divya and her mother. Conflicts were marked by verbal aggressiveness in Divya. At school, she feared that her peers would discover her traumatic experience and reject her. Disputes with friends at school and in the neighborhood were reported to increase after the trauma. She was observed to have developed a fear of elderly males and was observed to interact less and be watchful around such people. Divya also expressed fear about the outcome of the court trial and worried that the perpetrator would return to hurt her again. She was reported to have a decreased appetite and had not eaten sufficiently since the traumatic event.
Divya is the eldest among two siblings born of a non-consanguineous union, nuclear family, her father is a factory worker, and her mother is a homemaker. The mother is the primary caretaker of the child. There are inconsistencies in the parenting practices of the parents, as the father is warm and supportive of Divya and does not limit or set high expectations for her while the mother is strict, controlling, critical, has high expectations, and is unstable in being affectionate and supportive to her. Mother’s parenting style causes conflicts characterized by anger outbursts in Divya. She is emotionally attached to her father and her younger brother.
Having a normal development, Divya is temperamentally easy to warm up, cheerful, active, and sociable with normal moral standards, but low frustration tolerance, impulsivity, and sensitivity toward criticism. She is average in her studies and actively participates in extra-curricular activities at school.
Assessment
The first three sessions (excluding the therapy sessions) focused on building rapport and evaluations including case history.
At screening, Divya was assessed on the Strength and Difficulties Questionnaire (SDQ), 9 in which she obtained a total difficulty score of 13 (normal range). However, an analysis of her SDQ profile showed that the score of the emotional problem subscale was in the abnormal range. In pre-testing, she was assessed on the Clinician-Administered PTSD Scale for DSM-5 Child/Adolescent version (CAPS-CA-5), 10 on which her score was 29 (endorsing 12 symptoms), and she met the diagnostic criteria for PTSD. Analysis of the CAPS-CA-5 profile showed a high score on the subscale of intrusion symptoms. On Children’s Depression Inventory-2 (CDI-2), 11 Divya got a total score of 15 and a corresponding T-score of 59 which is in the average range. However, a profile analysis revealed an elevated score range for the interpersonal problems subscale (T-score = 82). Furthermore, on the Revised Children’s Manifest Anxiety Scale-2 (RCMAS-2), 12 she obtained a total score of 24 and a corresponding T-score of 61, indicating the presence of anxiety symptoms of moderate severity. The scores of validity scales of Defensiveness and Inconsistent responding index were in the normal range. Among the anxiety scales, Physiological anxiety (T-score = 61) and Social anxiety (T-score = 62) had scores indicating moderate severity. 3
Case Formulation
The traumagenics model proposed by David Finkelhor & Angela Browne (1985) 13 and the transactional model by Steve Spacarelli (1994) 14 are relevant in understanding Divya’s psychological adjustment to the abusive event.
The traumagenics model proposes four factors as the basis for psychological injury and the source of various emotional, behavioral, and cognitive symptoms in children who are sexually abused. They are traumatic sexualization, betrayal, powerlessness, and stigmatization. 13
Traumatic sexualization is the process by which a child’s sexuality is shaped in developmentally inappropriate and interpersonally dysfunctional patterns due to sexual abuse. 13 In Divya’s case, exposure to a sexual act shocked and alarmed her initially. Perception of invasiveness in the physical violation would have imparted intense feelings of disgust, shamefulness, and repulsion, thereby generating conflicts about self and leading to the belief that she became dirty and damaged (“I became dirty” as quoted by the child).
Betrayal is the dynamic by which children discover that someone they trusted and depended on has caused harm. 13 Divya’s perpetrator was known to her. He was married and had children. A sudden, unexpected incursion by a person who is a father figure would have violated her trust and led to fear for elderly males. The abusive event would also have undermined her trust in her mother as she, being the primary caretaker, was unable to protect Divya from abuse contributing to hostility and anger toward her mother.
Powerlessness occurs when the child’s will, desire, and sense of efficacy are contravened, and the child experiences coercion and manipulation by the offender. 13 Divya was made to engage in the act against her will, which would have produced feelings of inability and helplessness in her as it could not be prevented, leading Divya to assume responsibility for the occurrence of the act and the formation of negative beliefs such as “I have embarrassed my family in society.”
Stigmatization occurs when individuals in the family and community attach negative connotations to abuse and when children are treated as bad and blameworthy by offenders leading the child to incorporate these negative connotations into their self-image. 13 In Divya’s case, the responses of family and community members implied that an immoral and shameful act was committed against her, which contributed to her feelings and thoughts of unworthiness, indignity and self-blame (“My name is spoiled,” “No one in society would respect me because of what happened with me”).
In the index case, Steve Spaccarelli’s (1994) 14 transactional model (see Figure 1) is relevant in understanding the interactions between intrapersonal, environmental, and abuse-related factors that influence the development of symptoms post-CSA. The model has three basic principles: (a) Related to sexual abuse, the child faces an array of stressors that contribute to abuse stress. (b) the child’s cognitive appraisals and coping act as mediators between abuse stress and its outcomes, and (c) the relationship between abuse stress, coping and cognitive appraisals, and psychological consequences are bidirectional.
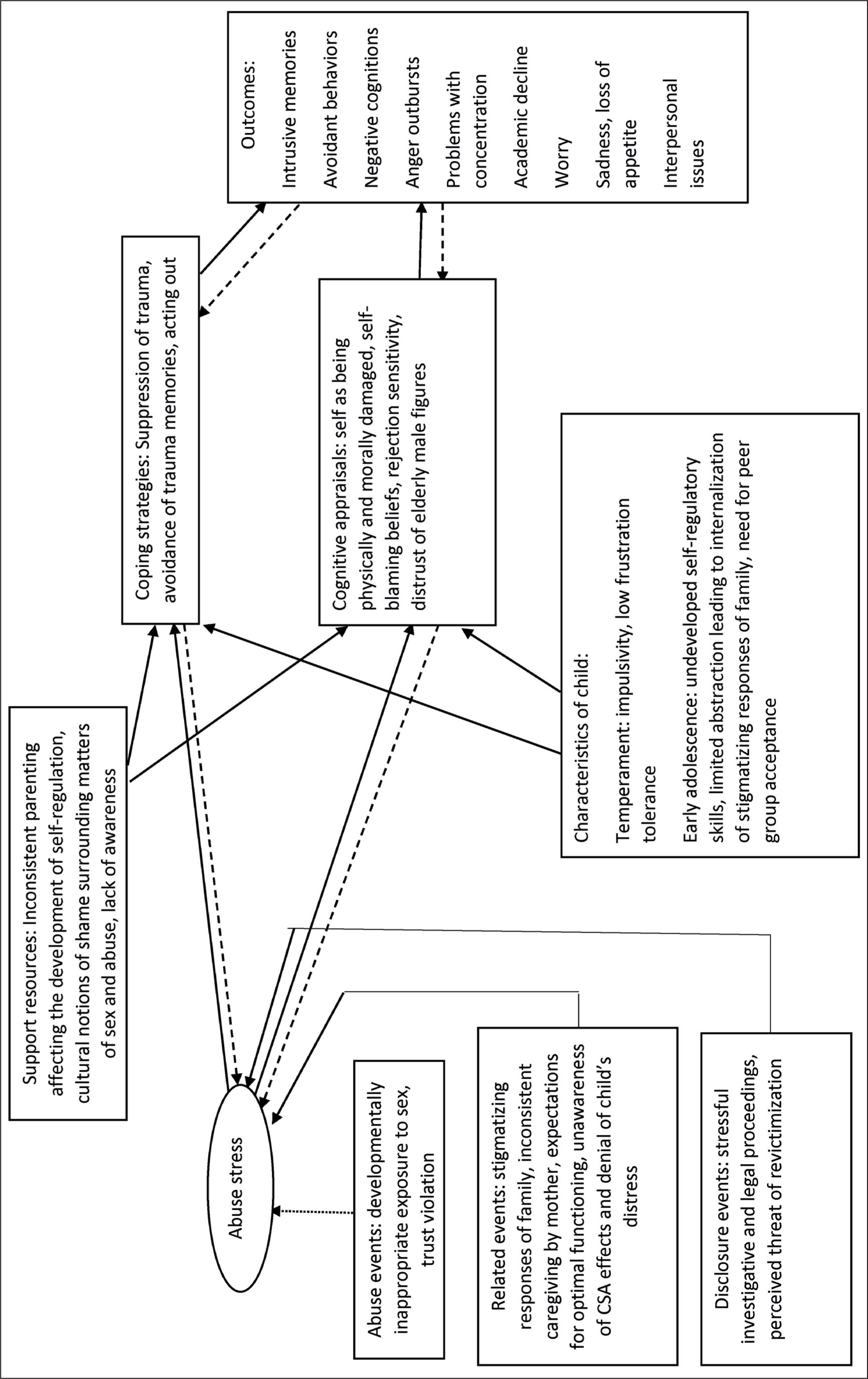
Furthermore, it is theorized that pre-existing factors related to the child and his/her environment can act as
Psychotherapy
Structure and Content
Therapy sessions were organized at the office of the Non-Governmental Organization through which the case was contacted for research study. Diyya was accompanied by her mother for every session. Adequate measures were adopted to ensure the privacy of the child during sessions.
Divya was provided 12 individual sessions of TF-CBT following the protocol of the research project in which her case was included. The sessions were 45 minutes-1 hour in duration and were provided weekly. The therapy components were imparted in a phased manner which included Psychoeducation, Relaxation Training, Affective expression and modulation, Cognitive coping, trauma narrative, and, Enhancing personal safety.
The components of parenting skills training, in vivo exposure (the only optional component which is provided only when clinically indicated), and conjoint parent-child sessions were not provided as parents did not participate in the intervention following the research criteria, owing to the heterogeneity concerning the family environment of child cases included in the research study.
Notwithstanding the exclusion of parent skills training in the intervention format, in view of concerns on the ethicality of the need to educate Divya’s mother due to the presence of a lack of awareness about the psychosocial impact of sexual abuse, parenting practices and stigmatizing responses that significantly contributed to child’s distress, a session was held in the beginning phase of therapy to educate mother about psychosocial effects of sexual abuse and relevance of adopting healthy parenting practices in the context of abuse. Also was a session organized for the mother at the final phase of therapy to discuss risk reduction, feedback about progress made by the child, and termination of therapy.
Goals
Therapy goals were set collaboratively based on Divya’s expectations from therapy, assessment findings, and TF-CBT objectives. She expected that therapy would help her deal with distressing memories of abuse and would help her to improve her academic performance. The therapist responded by acknowledging her needs as one of the important aspects that therapy would address.
The goals of therapy were: (a) to help contextualize and normalize the feelings, thoughts, memories, and distress associated with abusive experience, (b) to develop skills to manage trauma reminders, emotional regulation, and personal safety skills, (c) to form healthy beliefs about self and to facilitate the evolution of a new perspective of abusive experience
Therapy Process
The therapy components were provided sequentially under three phases namely stabilization phase, trauma narrative and processing phase, and integration and consolidation phase. Progression from one component to the next was carried out only after Divya had learned the skills adequately.
Stabilization Phase: (Sessions 1-6)
The treatment sessions began by providing the child with feedback about the assessment findings. Therapy was introduced to Divya as a safe place where she could talk about difficult feelings and thoughts related to the upsetting event she had experienced, learn more about the event she experienced, identify her strengths, and learn skills to manage difficulties associated with the abusive experience. The rationale for therapy, its phases and contents were elucidated in simple language and goals were discussed.
Though Divya showed readiness to know about the facts related to abuse, especially about how and why children feel after the abuse had occurred, and was receptive to the information provided by the therapist, she was observed to be in distress when discussions were about who is a perpetrator. The therapist validated and normalized the child’s feelings and praised her courage and decisiveness to address her difficulties.
A parallel session was conducted for the mother that focused on educating her about sexual abuse and its effects on the child’s psychosocial functioning. During the session, the mother expressed concern about Divya’s anger outbursts and her lack of interest in learning at home. She was supported in her concerns and was explained the impact of sexual abuse on children from a biological and psychosocial perspective. Because of stigmatizing responses in the family, the mother was also explained how such responses adversely affect the child’s mental health. The session also focused on improving her communication with the child (active listening, positive attention, utilizing praise), being consistent in showing warmth and support, and maintaining reasonable expectations and firm rules in the background of abuse. The mother comprehended the information provided in the session and consented to bring about changes in her interaction with Divya.
Divya’s task during this phase was to disclose overwhelming feelings triggered by traumatic memories to her mother while her mother was encouraged to support and listen to Divya when she disclosed her feelings. Divya also practiced recording the frequency of intrusive memories, trauma reminders, feelings associated with trauma memories, and their intensity in a logbook (on a scale of 1-10 based on the feelings thermometer given in the TF-CBT workbook).
The rationale for relaxation training, physiological and psychological responses to stress, and how the technique would help her manage reactions to trauma reminders and other stressors were explained. Both techniques were demonstrated by the therapist and practiced in session by Divya following which she started practicing regularly at home.
During this phase of therapy, Divya was reported to have been practicing relaxation techniques and affective modulation skills at home which was corroborated by her mother.
Trauma Narrative and Processing Phase: (Sessions 8-10)
Divya preferred to write about the abusive experience. Distress experienced was rated using the feelings thermometer (10-point scale) at the beginning, middle, and end of the activity. While writing about the experience for the first time (Session 8), she experienced intense feelings of sadness, resentment, and shame which she rated as eight at the beginning of the activity, nine in the middle, and eight by the end of the activity. The therapist validated her emotions and facilitated ventilation. Focused breathing was practiced in session by Divya.
She iterated the beliefs that were formed in her post-abuse like, “I brought shame to my family,” and “I became dirty.” These beliefs and other related thoughts reported during the evaluation by Divya were gradually brought forth and restructured.
The process continued in the 9th and 10th sessions wherein Divya reviewed the narrative, rated distress, practiced relaxation in session if indicated, and reframed negative thoughts. Negative thoughts about elderly males being dangerous were explored and were trust issues regarding the mother. The therapist facilitated the reframing of these negative thoughts, however, Divya showed ambivalence in addressing her thoughts about elderly males. Thoughts about peer rejection and fear of the perpetrator returning to harm her again were also addressed in this phase.
The process ended when Divya could tolerate trauma memories and reminders without experiencing significant emotional distress. Ratings of distress varied from 5 to 7 (10-point scale) in the 10th session while reviewing the narrative of the traumatic event. In the context of an observable decrease in distress experienced, Divya was motivated to continue the process of reviewing the narrative at home until the exposure to trauma content no longer generated negative emotions of high severity.
The application of various coping methods learned in therapy was emphasized. The trauma processing phase ended by listing down the skills learned to manage trauma memories, reminders, and avoidant behaviors. She also wrote down the new perspective she developed over the course of therapy about herself, abusive events, relationships, and her future.
Divya and her mother were notified about termination as Divya showed significant improvement in symptomatology and functioning.
Integration and Consolidation Phase: (Sessions 11 & 12)
Finally, the therapy goals were revisited, progress assessed, and feedback provided to Divya. Termination of treatment was discussed, and she was taught to recognize the warning signs that warrant the judicious use of the coping skills learned in therapy. Divya was praised for her efforts to manage her difficulties through active involvement in the therapeutic process, timely completion of homework, and regular practice of techniques at home.
A parallel session was held with the mother to discuss the safety plan for risk reduction and the progress made by Divya in therapy. The support provided by parents during treatment was acknowledged and praised, and they were advised to continue supporting the child in her efforts to cope with trauma.
Treatment Outcome
The assessment conducted post-therapy indicated that Divya has improved concerning presenting symptoms.
On CAPS-CA-5, she obtained a total severity score of 12 (compared to 28 in pre-assessment). She no longer met the diagnostic criteria for PTSD. On CDI-2, a total score of 8 and a corresponding T-score of 50 indicated that the score is in the average range. An analysis of the CDI-2 profile showed that all subscales (compared to elevated scores in the domain of interpersonal conflicts in pre-assessment) were in the average range. On RCMAS-2, a total score of 10 and a corresponding T-score of 44 were obtained, indicating that the severity level of anxiety symptoms is in the average range.
Divya reported a decreased frequency of intrusive memories and associated distress, improved capability in managing distress, and improved concentration on academic work. She no longer considered herself the cause of humiliation to her family and reported decreased feelings of shame and guilt. However, she reported the presence of thoughts about being violated and a lack of trust in elderly males. Interpersonal issues were reported to have decreased with her mother and friends. Also, her appetite was reported to have improved.
“I was small, I did not understand, I did not expect it (abusive act), but I could save myself from more harm. I was strong.” (about abusive experience)
“That incident… (abusive event) it is not my fault, it is his.”
“I want to go ahead… I want to go to college and secure a job.”
“I can learn a little more at home, need to keep trying.”
“I am not always angry… like before… so I fight less with mother and friends….”
Discussion and Therapist’s Reflections
The TF-CBT was provided to the child without any modification to the manual and its core components, given the adaptable nature of the treatment model for diverse populations and settings. However, analogies appropriate for Indian culture were used for the implementation of contents like Affective expression and modulation, and trauma narrative. 8
Divya reported significant improvement in her symptoms concerning PTSD, depression, anxiety and her functioning,15–17 which was corroborated by her mother and through clinical assessment. Many factors contributed to treatment gains. Divya was aware of the association between her distress and trauma experience and hence was motivated to actively involved in treatment from the beginning of therapy. A positive relationship based on trust, safety, openness, warmth, and validation could be established with her, which mobilized active collaboration on therapy goals and tasks. Her mother was receptive to the new information related to the effects of sexual abuse and the need for positive parenting, and both parents supported the child’s participation in therapy till the end.18,19
The self-efficacy-based model of TF-CBT, which focused on providing knowledge and skills, and the manual’s adaptable nature, which provides the therapist with the flexibility to use culturally sensitive ways to implement treatment components, 8 made it safe and acceptable to the child and usable for the therapist. In addition, the treatment provided a means for appropriate externalization of distress and processing of trauma. This holds relevance in the Indian context, where the community is largely unaware of the mental-health effects of CSA and expects the child to function optimally, disregarding the child’s distress which eventually taxes his or her mental health. 20
However, certain aspects of the case limit the generalization of the findings. To begin with, the case is part of a research project that lacks a follow-up period, hence there is no data available on whether the improvement in symptomatology post-therapy was maintained in the long term. The child’s motivation and active involvement in therapy, child’s attributes like openness, assertiveness, and ambitiousness as well as the parent’s support for her participation, essentially contributed to the outcome of therapy, which may not be observed in other cases of sexual abuse. Finally, the severity of abuse and other contextual factors may determine the duration of the implementation of components like trauma narrative and in vivo exposure and the entire contents of TF-CBT.
Barriers and Challenges Faced in Therapy
The child’s mother was unfamiliar with structured mental-health treatment and had to be explained about the need for counseling the child beyond 1 or 2 sessions. She had to be explained that counseling is different from advice-giving and is not about helping the child to forget about trauma. The mother was excessively concerned about the child’s academics and worried whether talking about the abusive event would adversely affect the child.
Scheduling of sessions was yet another concern as school worked till Saturday and sessions had to be arranged on Saturday afternoons after school hours.
Conclusions and Implications
To conclude, this case study emphasizes one of the primary concerns that victimized children face, which is the denial of mental health care for the needy due to a lack of awareness among primary caregivers about the mental health effects of CSA and the stigma surrounding CSA and mental-health issues. The case throws light into the need for regular case management or monitoring of CSA survivors for potential psychosocial effects of abuse for a considerable period following abuse.
The participation of non-offending parents or caregivers in the psychotherapy is paramount as it would help address interpersonal and parenting issues and the effects of trauma on parents adequately.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed consent from the parent and assent from the child were obtained for assessment, therapeutic work, and publication. Ethical approval for the study was provided by the Institutional Ethics Committee (IEC) of the National Forensic Sciences University.