
Abstract
Background:
The objective of this research is to provide ideal interventions for youth engaged in self-harm, addressing the scarcity of literature exploring these interventions. While dialectical behavior therapy (DBT) and cognitive behavioral therapy are common approaches, this study aims to explore the potential of problem solving therapy (PST) and coping skills therapy as promising interventions.
Methods:
The study is guided by cognitive behavioral theory (CBT), which provides the framework for understanding the relationships between cognitive constructs, personality profiles, coping skills, problem-solving abilities, emotions, and self-harm behaviors among adolescents. The research is designed as a randomized study protocol and includes primary and secondary outcome measures, including assessments of depressive and anxiety symptoms, quality of life, cognitive constructs, and personality profiles. Gender-specific effectiveness and the effectiveness of interventions in youth with borderline personality disorder (BPD) are also considered.
Study Setting:
The study will be conducted at the Institute of Medical Sciences and SUM Hospital, Bhubaneswar, India.
Statistical Analysis:
The statistical analysis will include a t-test, repeated measures ANOVA, regression analysis, and correlation coefficients to assess the interventions’ effectiveness and their interactions with individual characteristics. Nonetheless, this research protocol holds promise in providing valuable understanding into modified interventions for youth engaged in deliberate self-harm (DSH) behaviors.
Introduction
Deliberate self-harm (DSH) behaviors among youths represent a significant public health concern, prompting the need for interventions that consider individual differences in cognitive constructs and personality profiles. DSH is often characterized by non-suicidal acts of self-injury, It is common among teenagers and young adults and has been linked to various adverse effects, including a heightened risk of suicidal behaviors, psychiatric disorders, and impaired psychosocial functioning.1,2 To address this critical issue, researchers and clinicians have explored various therapeutic approaches, including problem solving training (PST) and coping skills training (CST), which target core cognitive and emotional processes implicated in self-harm.3,4
The effectiveness of these interventions, however, may be contingent upon an individual’s cognitive constructs and personality profiles, which can influence significantly their ability to engage with and benefit from therapeutic strategies.5,6 For instance, individuals with certain cognitive styles, such as rumination or impaired problem-solving abilities, may require targeted remedies that specifically address these cognitive processes.7,8 Similarly, personality traits, such as emotional regulation difficulties or impulsivity, can have an impact on an individual’s response to CST and the extent to which they can effectively manage distressing emotions.9,10
Considering the diversity among the group of young individuals involved in DSH, a detailed understanding of how cognitive constructs and personality profiles interact with treatment modalities is vital. This protocol outlines the design and methodology of a randomized study aimed at investigating the differential effectiveness of PST and CST among youths with varying cognitive constructs and personality profiles who engage in DSH behaviors. Having a cursory examination of how these personal characteristics interact with the remedies, the study’s aim is to provide understanding for creating already tried and tested interventions that can lead to improved well-being and resilience for at-risk youth.
Historical and psychoanalytic perspectives have previously linked self-mutilation to religious fervor and sexual symbolism. 11 However, contemporary research has shifted toward understanding deliberate self-harming behaviors within the context of psychological distress and coping mechanisms. Despite historical and cultural variations in the expression of self-harm, modern interventions such as PST and CST can offer promising avenues for supporting youth struggling with these behaviors.
In adolescents, self-harm results from a highly “complex interplay between genetic, biological, psychological, social, and cultural factors.”1,12
In India, self-harm and related risk behaviors among children and adolescents have received limited attention from the community, family, and government.1,12 According to Kpeno et al., 13 adolescent behavior, including self-harm, is influenced by cultural and social contexts. Additionally, the rise in self-inflicted harm among children and adolescents, particularly those from lower socioeconomic groups, is ascribed to socioeconomic disparity. Furthermore, the authors highlight the impact of societal and cultural norms on the perception of health and well-being among Indian children and adolescents, shaping their behavior. 13
This research protocol emphasizes the pressing need for interventions geared toward addressing DSH behaviors among youths. Bearing in mind the nature of these behaviors, including their prevalence, impact, and complex origins, our study endeavors to shed light on the critical relationship between cognitive constructs, personality profiles, and treatment modalities. This randomized study aims to decipher the success of PST and CST in diverse contexts, acknowledging the uniqueness of each individual’s psychological makeup.
The Study Objective is
To investigate the success of PST and CST for 12 sessions (at a gap of two weeks intervals, hence spanning a period of six months) in reducing DSH behaviors in adolescents having different cognitive constructs and personality profiles having a background of self-inflicted harm behaviors based on the following outcome:
Primary Outcome
To assess the efficacy of problem-solving skills and coping skills relative to dialectical behavior therapy (DBT), the established treatment protocol was employed by clinical psychologists at the Department of Psychiatry at SUM Hospital (the study setting). This will be assessed using the problem solving inventory 14 and brief cope questionnaire. 15
Secondary Outcome
To investigate the effectiveness of PST and CST interventions in reducing DSH behaviors and associated results such as depressive symptoms, anxiety, and quality of life in adolescents with different cognitive profiles.
Depressive and anxiety symptoms will be assessed using “Hamilton Depression Rating Scale (HAM-D)” 16 and “Hamilton Anxiety Rating Scale (HAM-A, also known as HARS)” 17 respectively for measuring the duo.
Methods and Analysis
To ascertain the association between specific personality traits and cognitive constructs and the effectiveness of distinct interventions, namely problem-solving skills training, CST, and DBT.
This will be measured by performing a statistical analysis to identify correlations or associations between specific personality traits cognitive constructs and intervention outcomes. Techniques such as regression analysis or correlation coefficients will be helpful in quantifying these relationships. Also, the “Non-Suicidal Self-Injury Assessment Tool (NSSI-AT)” 18 and Automatic Thoughts Questionnaire (ATQ) 19 and Dichotomous Thinking Inventory (DTI) 20 will be used for the measure.
To assess the gender-specific efficacy of problem-solving and CST compared to a control group in mitigating self-harm behaviors and enhancing mental health outcomes among male and female adolescents with a history of DSH.
To assess this, we will collect participants’ demographic information and conduct a pre-intervention assessment. Subsequently, following the administration of the interventions, a post-intervention assessment will be conducted, separately for males and females, to evaluate self-harm behaviors and mental health outcomes. This will facilitate the assessment of how the interventions have influenced each gender. Statistical analysis will be conducted, employing t-tests, to detect any noteworthy differences or associations.
To examine the effectiveness of PST and CST compared to a control group in reducing self-harm behaviors and improving mental health outcomes in youth with borderline personality disorder (BPD) who have different cognitive constructs and personality profiles
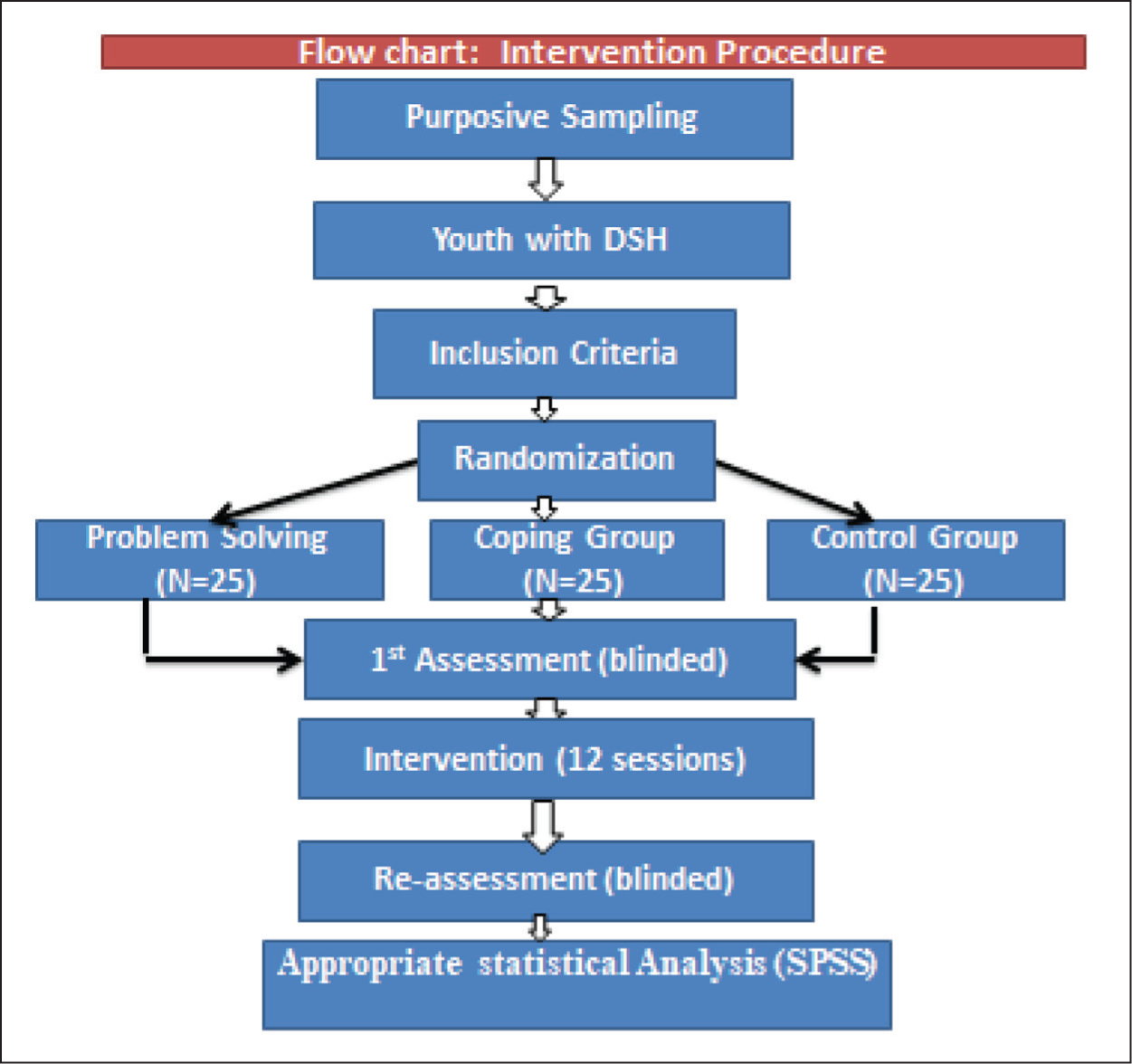
Assessment will be carried out at baseline and after completion of the interventions, thus after the 12 sessions. This procedure is outlined in Figure 1.
Represents the intervention procedures for pre and post assessment.
Inclusion Criteria
In this study focused on understanding DSH behaviors in youth, it is crucial to establish clear inclusion criteria to define the target population. Inclusion criteria serve as specific guidelines for participant selection, ensuring that the research objectives are met effectively and accurately. In the context of this study, the term DSH is defined in accordance with the study’s objectives. “Deliberate self-harm (DSH), also referred to as superficial moderate self-mutilation, self-injurious behavior (SIB), parasuicide, and self-wounding, refers to the wary harm of one’s own body without a clear suicidal intention” Youth, on the other hand, have been defined to include all those persons within the age brackets of 15-29 as defined by the National Youth Policy of India, 2014.
20
The following criteria outline the characteristics and conditions that prospective participants must meet to partake in this training:
Participants or their legal guardians providing written informed consent to take part in the research, aged 15–29 of both genders. Participants must have at least a high school education and be proficient in English reading, writing, and speaking. Patients with DSH behaviors.
Exclusion Criteria
To maintain the integrity and relevance of this research on DSH behaviors in youth, it is equally important to establish exclusion criteria. Exclusion criteria help identify and exclude individuals who, due to specific factors or conditions, may not align with the study’s primary focus or may introduce confounding variables. The following criteria outline conditions and characteristics that may render individuals ineligible for participation in this study:
Patients with a history of mental retardation or spectrum disorders. Presence of any serious physical disorders, head injuries, or neurological disorders. If a patient was currently using substances in the dependent pattern. Alcohol dependence.
Design
In this research study, a meticulous and impartial allocation process will be employed to ensure the credibility and reliability of the findings. Given that participants will be recruited over time as they visit the hospital, the Sequentially Numbered, Opaque, Sealed Envelopes (SNOSE) method will be utilized for patient allocation. The preparation of sealed envelopes, each containing a unique identification number corresponding to one of the study groups, will be conducted in advance. When a patient becomes eligible and consents to participate, a designated individual who is not directly involved in the study and remains blinded to the group assignments will execute the random allocation. This approach guarantees that neither the researcher nor the participants are aware of the group assignments, thereby maintaining the single-blind design method throughout the study. The utilization of SNOSE envelopes ensures a transparent and unbiased allocation process, even in situations where participants are recruited incrementally as they seek medical care at the hospital. Even when participants are added gradually as they seek medical attention at the hospital, the use of SNOSE assures an open and fair allocation procedure. The strength of our study design is improved by this technique. There will be three groups: a problem-solving skills training group, a CST group, and a control group for DBT.
Study Site and Population
The study will be conducted at the psychiatry department, of the Institute of Medical Sciences and SUM Hospital. This Hospital is located in Bhubaneswar, in the state of Odisha/Orissa, India.
Recruitment and Baseline Assessment
Recruitment
As eligible patients seek medical care at the Institute of Medical Sciences and SUM Hospital, they will be identified based on the inclusion criteria. These criteria include participants or their guardians providing written informed consent, age falling within the range of 15-29 years, proficiency in English reading, writing, and speaking, at least a high school education, and a history of DSH behaviors.
Once a patient fulfills these criteria and consents to participate, a designated individual who is not directly involved in the study and remains blinded to the group assignments will execute the random allocation process using the SNOSE envelopes. This method ensures that neither the researcher nor the participants are aware of the group assignments, thereby maintaining the single-blind design method throughout the study.
Baseline Assessment
A complete baseline examination will be carried out in order to develop a thorough understanding of the participants’ cognitive construct, personality profiles, and self-harm behaviors. This assessment will serve as a foundation for subsequent evaluations and analyses.
The baseline assessment will include the collection of demographic information, such as age, gender, and educational background, to characterize the study population accurately. Additionally, participants will undergo a pre-intervention evaluation, which includes measuring self-harm behaviors, cognitive constructs, and personality traits.
Self-harm behaviors will be assessed using validated tools and questionnaires, including the “Non-Suicidal Self-Injury Assessment Tool (NSSI-AT).” 18 Cognitive constructs will be evaluated using assessments like the Automatic Thoughts Questionnaire (ATQ) 19 and the Dichotomous Thinking Inventory (DTI). 20 Personality traits will be assessed using the Sixteen Personality Factors (16PF) 21 standardized personality assessments.
Furthermore, baseline assessments will encompass evaluations of depressive and anxiety symptoms using established instruments such as the “Hamilton Depression Rating Scale (HAM-D)” 16 and “Hamilton Anxiety Rating Scale (HAM-A, also known as HARS).” 17
This thorough baseline assessment will provide a comprehensive understanding of each participant’s cognitive and emotional characteristics, enabling us to explore the associations between these factors and treatment outcomes effectively.
Intervention
Problem-solving techniques are cognitive-behavioral strategies that help individuals identify and address challenges in their lives. The relevance of these techniques especially within the context of DSH is in their ability to help young individuals develop healthier ways to cope with stressors and negative emotions. Problem solving therapy (PST) is a common approach which involves several steps; problem orientation, problem definition, generating alternatives, decision making, solution implementation and solution evaluation. 22 Problem-solving techniques will be taught through structured group therapy sessions or individual counseling.
CST as an intervention measure is aimed at teaching young individuals healthier and more adaptive ways to cope with stressors, leading to a reduction in the likelihood of engaging in self-harm behaviors. 23 Learning to identify and regulate one’s emotions through the teachings of emotion regulation techniques, using problem-solving techniques to address challenges, social support, distraction techniques (engaging in activities that divert attention from negative thoughts or urges) and relaxation methods such as deep breathing or progressive muscle relaxation, all of these strategies form a comprehensive package for individuals facing DSH behaviors.
Each intervention will be held in 12 sessions, the duration for each session will be 45 minutes. The interval between sessions will be two weeks. The intervention providers will be the trained clinical psychologists who are providing clinical counseling in the psychiatry department of the study setting. They have several years of clinical practice experience.
Regarding the control of confounding variables, randomization of the participants into treatment groups will ensure a balanced distribution of confounding factors across groups. Additionally, we will conduct baseline assessments to collect data on relevant covariates, such as demographic characteristics, baseline symptom severity, and prior treatment history. These covariates will be included as control variables in our statistical analyses to account for their potential influence on treatment outcomes.
Furthermore, we will monitor treatment compliance and attendance throughout the study to assess the fidelity of intervention delivery and minimize attrition-related biases. Any missing data related to intervention compliance or dropout rates will be addressed using appropriate statistical methods, such as sensitivity analyses or imputation techniques.
Statistical Analysis
The statistical analysis for this research is designed to carefully evaluate the effectiveness of PST and CST interventions in reducing DSH behaviors among youths with varying cognitive constructs and personality profiles. The analysis aims to provide robust and meaningful insights into the impact of these interventions and their interactions with individual traits.
Primary Analysis
Comparison of PST and CST with DBT
To assess the efficacy of problem-solving skills and coping skills relative to DBT, the established treatment protocol, the problem solving inventory 14 and brief cope questionnaire 15 will be used.
We will employ the same assessment scales during both the baseline and post-intervention assessment stages for all participants, ensuring uniformity in data collection and facilitating meaningful comparisons between the groups.
Statistical analysis will involve comparing the mean scores between the PST and CST groups and the DBT group. Analysis of Variance (ANOVA) or similar appropriate tests will be employed, followed by post-hoc tests if necessary, to identify significant differences in the effectiveness of these interventions.
Secondary Analysis
Effectiveness of PST and CST in Reducing DSH Behaviors and Associated Outcomes
To investigate the effectiveness of PST and CST in reducing DSH behaviors and associated outcomes, including depressive symptoms, anxiety, and quality of life, the “Hamilton Depression Rating Scale (HAM-D)” 16 and “Hamilton Anxiety Rating Scale (HAM-A, also known as HARS)” 17 will be used.
Repeated measures ANOVA or mixed-design ANOVA will be employed to examine changes in outcomes over time (pre-intervention to post-intervention) within each group and between the groups (PST, CST, and DBT).
Association Between Personality Traits and Cognitive Constructs with Intervention Effectiveness
To ascertain the association between specific personality traits and cognitive constructs with the effectiveness of distinct interventions, regression analysis or correlation coefficients will be used.
The “Non-Suicidal Self-Injury Assessment Tool (NSSI-AT),” 18 Automatic Thoughts Questionnaire (ATQ), 19 and Dichotomous Thinking Inventory (DTI) 20 will be utilized to measure these factors.
Separate analyses will be conducted for each personality trait and cognitive construct, examining their relationship with intervention outcomes.
Gender-specific Efficacy Analysis
To assess the gender-specific efficacy of PST and CST compared to a control group in mitigating self-harm behaviors and enhancing mental health outcomes, demographic information and pre-post-intervention assessments will be analysed separately for males and females.
Statistical analysis will involve comparing the changes in self-harm behaviors and mental health outcomes within each gender group across the interventions. T-tests or similar appropriate tests will be used to detect significant differences or associations.
Effectiveness in Youth with BPD
To examine the effectiveness of PST and CST compared to a control group in reducing self-harm behaviors and improving mental health outcomes in youth with BPD who have different cognitive constructs and personality profiles, separate analyses will be conducted for this subgroup.
Similar statistical methods as mentioned above will be applied to evaluate the impact of the interventions on youth with BPD specifically.
Statistical analysis will be carried out using appropriate software (e.g., Statistical Package for Social Sciences, R), the significance level will be established as p < .05. The outcomes will be reported comprehensively, including effect sizes, confidence intervals, and any potential covariates that may influence the outcomes. This rigorous statistical approach will provide valuable insights into the effectiveness of the interventions, their suitability for different subgroups, and their interaction with individual characteristics, thereby contributing to the development of tailored interventions for youths at risk of DSH behaviors.
Study Population and Sample Size Determination
The researcher aimed to define the study population from the patient registers at the psychiatry department’s out-patient department (OPD) and in-patient department (IPD). This data extraction process covered the time period from October 2022 to August 2023, coinciding with the researcher’s arrival at the department. From the department’s records, it was identified that a total of 75 patients met the inclusion criteria for the study, as they had sought medical attention for DSH behavior. To determine the appropriate sample size for the study, the researcher utilized the following formula:

n: Required sample size
N: Population size (75 patients)
Zα/2: Critical value for the desired confidence level (e.g., for 95% confidence, Zα/2 is approximately 1.96)
e: Margin of error (desired level of precision).
Using the formula, the calculated sample size was 63. To account for potential changes in the population and attrition or participant dropouts during the study, the researcher decided to add 20% of the calculated sample size. This adjustment is to ensure that the study would maintain an adequate sample size even if some participants were unable to continue. As a result of this adjustment, the final sample size was determined to be 75, rounding up from the calculated sample size of 63.
Theoretical Underpinning of the Study
In this study investigating the effectiveness of PST and CST for DSH behaviors in youths with varying cognitive constructs and personality profiles, a relevant psychological theory that can underpin the research is the cognitive behavioral theory (CBT).
“Cognitive Behavioural Theory (CBT)”, as proposed by Beck and expanded upon by many others, posits that thoughts, emotions, and behaviors are interconnected and provides a comprehensive framework for understanding how individuals process information and how this processing influences their actions. 21
Thought Pattern
According to CBT, individuals exhibit specific thought patterns that can contribute to self-harm behavior. Negative thought patterns, such as rumination or automatic negative thoughts, may be associated with self-harm. Cognitive constructs related to self-criticism or hopelessness can also be explored within this framework. 21
Emotional Regulation
CBT emphasizes the role of emotions in influencing behavior. It suggests that individuals who struggle with emotional regulation may be more prone to self-harm as a way to cope with intense emotions. This theory allows you to examine how CST can help individuals better manage their emotions and reduce self-harm as a maladaptive coping strategy. 24
Behavioral Change
CBT is action-oriented and focuses on changing behaviors by addressing underlying cognitions and emotions. 25 This study seeks to investigate how PST can equip individuals with the skills needed to address life stressors and problems in a healthier way, thereby reducing the need for self-harm.
Individual Differences
CBT recognizes that individuals have unique cognitive styles and personality traits. It can provide a framework for exploring how these individual differences interact with the interventions. For example, you can examine how certain cognitive constructs and personality profiles may influence the effectiveness of PST and CST. 26
Treatment Customization
CBT supports the idea of tailoring interventions to individual needs. Your study can draw on CBT principles to assess whether customizing interventions based on cognitive and personality factors leads to better outcomes for participants. 27
Results
This study outlined herein is only a protocol of what the researchers intend to carry out and hence there are no results to be presented at this stage. This protocol only intends to serve as a guide showcasing the design, methods, and anticipated outcomes of the proposed investigation.
Discussion
The rising prevalence of DSH behaviors among youths presents a pressing challenge in the field of mental health. 28 While clinicians typically provide supportive psychological care, the increasing complexity and severity of cases demand tailored interventions, especially for those with severe or persistent self-harming behaviors or clear suicidal tendencies. Despite the growing need, there is a noticeable scarcity of research articles that delve into the nuanced examination of cognitive constructs and personality factors as they relate to DSH behaviors in the youth population. Furthermore, studies investigating the efficacy of problem-solving skills training and CST as interventions for youth engaged in self-harm are notably limited.
In the realm of psychological interventions, “Dialectical Behaviour Therapy (DBT)” and “Cognitive Behaviour Therapy (CBT)” have been the predominant choices among clinicians. 29 These evidence-based approaches have demonstrated effectiveness in addressing various mental health challenges, including self-harm behaviors. However, the demand for more diverse and targeted interventions is on the rise. Our discussion is guided by the theoretical framework of CBT, emphasizing the interconnectedness of thoughts, emotions, and behaviors. 24
The present research protocol aims to bridge this gap in the literature by exploring the potential of problem-solving skills training and CST as promising alternatives for addressing DSH behaviors among youths. These interventions hold significant promise, offering a fresh perspective on how cognitive processes and personality traits can be harnessed to guide therapeutic strategies.
An understanding of the cognitive processes that contribute to self-harm, such as negative thought patterns or impulsive behaviors, is essential. Similarly, recognizing how personality factors like emotional regulation difficulties or impulsivity can influence one’s response to coping and problem-solving strategies is critical. It is within this complex web of cognitive and emotional factors that the potential effectiveness of problem-solving skills and CST emerges.
This study is poised to offer mental health practitioners an expanded toolkit for working with young individuals grappling with DSH. The findings may suggest that interventions targeting cognitive and emotional processes specific to self-harm could be integrated alongside, or even in place of, established therapies like DBT and CBT. By diversifying the available therapeutic approaches, clinicians can better cater to the unique needs of their clients, potentially enhancing treatment outcomes.
Strengths and Weaknesses of the Protocol
Strengths
Theoretical Framework
One of the strengths of this protocol is its strong theoretical foundation in CBT. By using cognitive behavioral therapy as the underpinning theory, the research benefits from a well-established framework that links cognitive processes, emotions, and behaviors, providing a comprehensive understanding of DSH behaviors among youths.
Customized Interventions
The strength here is the consideration of individual differences in cognitive constructs and personality profiles. By designing interventions such as PST and CST to specific cognitive and personality factors, the study aims to provide better and potentially more effective treatments.
Single-blind Design
The use of the SNOSE method for patient allocation, coupled with a single-blind design, adds a lot of value and credibility to the research design. This approach reduces bias and ensures that neither the researcher nor the participants are aware of group assignments.
Weaknesses (Anticipated)
Sample Attrition
One potential weakness is the possibility of sample attrition during the course of the study. While we have accounted for this by adding 20% to the initial sample size, real-world circumstances may lead to a higher attrition rate, which could impact the study’s power.
Generalizability
The study will be conducted at the Institute of Medical Sciences and SUM Hospital in Bhubaneswar. This could potentially restrict the applicability of the results to different populations or environments. It is essential to acknowledge this limitation and consider its implications for the broader applicability of the results.
Limited Long-term Follow-up
Given the study’s duration of 12 sessions (with a week gap between sessions), it may provide insights into short-term outcomes. However, the long-term effects of the interventions may not be fully captured within this timeframe. Due to the unique circumstances of this study, which involve the principal investigator who is an international student, there are practical constraints that necessitate the exclusion of long-term follow-up assessments. Engaging in extensive follow-up activities beyond the stipulated study period would potentially extend the duration of the study unduly and could pose logistical challenges. Consequently, it has been determined that focusing on short-term outcomes aligns with the study’s scope and feasibility, while still offering valuable insights into the immediate effects of the interventions on DSH behaviors, cognitive constructs, and personality profiles. This limitation is acknowledged, and the study aims to maximize the depth and quality of data within the defined timeframe.
Conclusion
By examining the relationship between cognitive constructs, personality factors, and the effectiveness of problem-solving skills training and CST in the context of DSH behaviors among youths, the current study aims to fill a gap in the body of literature. This study has the potential to deepen our understanding of self-harm and offer creative treatment options to mental health professionals, ultimately resulting in more efficient and specialized care for young people who are at risk.
Footnotes
Acknowledgements
The authors are highly grateful to the research members of IMS and SUM Hospital, Siksha O Anusandhan (Deemed to be University), Bhubaneswar for providing all the support during the work.
Availability of Data
This is a protocol so there is no data at this stage of the study.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
During the preparation of this work the authors used ChatGPT tool in order to improve the readability of the article. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethical Approval
The study received ethical approval from the Institutional Ethics Committee (No. ECR/628/Inst/OR/2014/RR-20, dated 27th June 2023) and the Scientific Review Committee of the Institute of Medical Sciences and SUM Hospital (Letter No. IMS/SRC/161/2023 and Ref. No. IEC/IMS.SH/SOA/2023/547).