
Abstract
Aim:
Dissociative disorder is a common and distressing condition seen in children and adolescents, especially in the Indian population. It is associated with impairment in routine functioning, school absenteeism, and a significant distress and economic burden on the caregivers. There is scarcity of outcome studies in the Indian population. This study aimed to evaluate the sociodemographic and clinical profile of children and adolescents with dissociative disorder and find the outcome with treatment as usual at the end of one month.
Methods:
This was an observational study conducted in a tertiary care hospital over a period of one year. Fifty-one children and adolescents with mean age 14.2 years (± 2.050) with dissociative disorder (International Classification of Diseases, 10th revision [ICD-10]) were included in the study. Sociodemographic and clinical details were assessed using semi-structured proforma and Children Global Assessment Scale (CGAS), and Clinical Global Impression-Severity (CGI-S) were used to assess baseline functioning. After one month of treatment, as usual, outcome was assessed either face-to-face or through telecommunication using CGAS, CGI-S scales.
Results:
Dissociative stupor (37.3%) was the most common type of presentation followed by dissociative convulsions (21.6%). Most prevalent stressor was familial (39.2%) and parenting style was authoritative (19.6%). Slow-to-warm-up temperament was most frequent (39.2%) in study subjects. At the end of one month of treatment as usual on CGAS, the percentage of subjects with obvious or serious problems reduced to 7.9 from 35.3% which was statistically significant (P <.05). On CGI-S 56.8% of the participants significantly improved on follow-up (P < .05). On CGI-I, 51% had much improvement, 19.1% showed very much improvement from baseline, whereas, 31.4% had minimal improvement.
Conclusion:
Dissociative disorders are common in adolescent age and most commonly associated with familial stressors and authoritative parenting in our study. We found a significant number improved at the end of one month with treatment as usual indicating good short-term outcomes.
Introduction
Dissociative disorder is a common child psychiatric condition characterized by a partial or complete loss of the normal integration between memories of the past, awareness of identity and immediate sensations, and control of bodily movements. 1 Even though the prevalence in Western populations is low (2.3–4.2 per 1 lac in Australia and 1.30 per 1 lac in the UK & Ireland) 2 studies in India have shown higher prevalence. Outpatient prevalence of dissociative disorder was found to be 14.8% in a tertiary hospital in South India. 12 While the outcome in both populations is generally good, with rapid resolution within a week to a month9,12 and good one-year outcomes, 2 longer-term studies indicate that patients may be at risk of developing depressive and anxiety disorders even after resolution in dissociative symptoms. 7
Literature on the clinical profile of dissociative disorders in children and adolescents is limited, with regard to stressors, treatment received, and short-term outcomes. With this in mind, we intended to study the clinical profile and short-term outcome of children and adolescents with dissociative disorder presenting to tertiary care hospitals.
Methods
This observational study was conducted in a tertiary care hospital in southern part of India over a period of one year from January 1, 2021 to December 31, 2021, following ethical clearance from the institute. The study included 51 willing children and adolescents, with a mean age of 14.2 years (± 2.050) (0–18 years), and majority (66.7%) of patients were female. These participants, who presented directly or were referred to the child and adolescent psychiatry service, were diagnosed according to International Classification of Diseases, 10th revision Diagnostic Criteria for Research (ICD-10 DCR) and did not have any severe mental illness (including bipolar and psychotic illnesses) or intellectual disability (which were ruled out using clinical interview and ICD-10 criteria). A semi-structured questionnaire was administered to collect sociodemographic details and patient characteristics at the time of presentation and described in Table 1. Baseline illness severity was assessed using the CGI-S (Clinical Global Impression-Severity) Scale, 3 while functioning was evaluated with the CGAS (Children Global Assessment Scale) 10 and SDQ (Strengths and Difficulties Questionnaire). 6 Any comorbid psychiatric illnesses were assessed and/or ruled out using a semi-structured interview using diagnostic criteria from ICD-10. Parenting style was assessed using parent interview based on Parental Style Questionnaire based on Robinson et al. 3 and similarly, temperament of the children was assessed using a questionnaire based on the Thomas and Chess classification of temperament. 4 The participants received standard treatment and were followed up after a month through outpatient department (OPD) visits or voice/video calls, owing to the coronavirus disease 2019 (COVID-19) pandemic. After a month, the study participants were reassessed using CGAS and CGI-S and the CGI-I (Clinical Global Impression-Improvement) Scale. 3
Patient Characteristics.
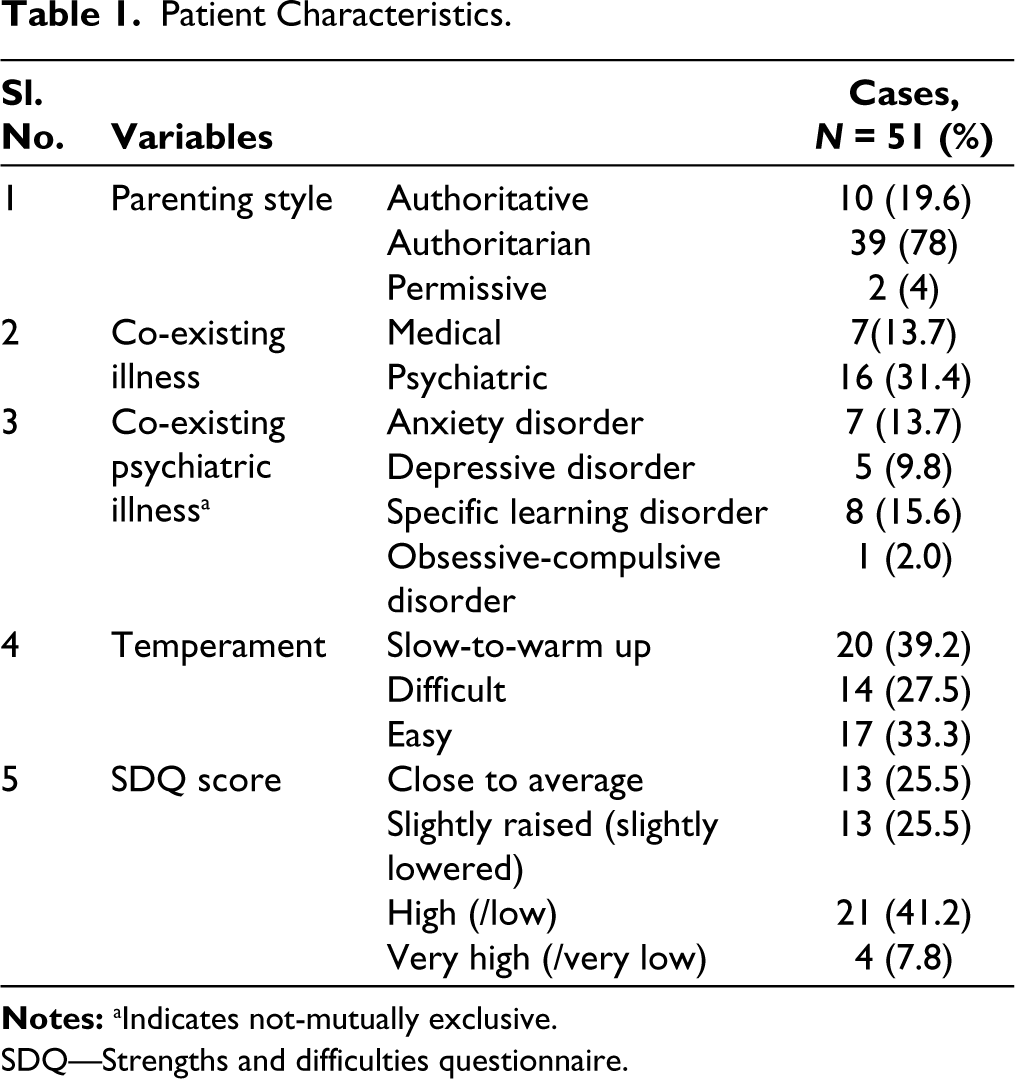
SDQ—Strengths and difficulties questionnaire.
Results
In our study, children and adolescents diagnosed with dissociative disorders were followed up after a month following standard treatment comprising of psychoeducation, family education, medications, and liaison with school wherever required. We found that the most common temperament among these patients was slow-to-warm-up, followed by easy and difficult temperament. Children with slow-to-warm-up temperament may have immature coping skills, which may make them more susceptible to develop dissociative disorders. However, a previous study found that easy temperament was the most common. 8 Nevertheless, there are studies that suggest that easy temperament may be a protective factor.14–15 Most patients in our study had high/low SDQ scores, indicating that they faced more difficulties than the general population. As seen in Table 2, dissociative stupor was the most common type of dissociation, followed by dissociative convulsions. In a similar study, dissociative convulsions were the most common. 9 Majority of patients were referred from either other departments of the hospital or from outside practitioners. In other studies as well, 5 the patients who had duration of illness for more than one year had prior consultation by multiple physicians and neurologists. This was also seen in another study where majority had consulted a local faith healer and/or general practitioner before seeking psychiatric consultation and almost every child was referred to psychiatric services from other departments. 9 Patients mostly received pharmacotherapy, with selective serotonin reuptake inhibitors (SSRIs) being the most commonly prescribed medication.
The baseline CGAS and CGI-S scores of the participants were obtained during the initial consultation, and repeated after one month. As seen in Table 3, there was statistically significant improvement on CGAS and CGI-S scales. On CGAS, at the time of the first visit, 35.3% of the participants had obvious or serious problems, while 64% had problems ranging from some problems to some noticeable problems. However, after one month of treatment, the percentage of obvious or serious patients reduced to 7.9%, and the number of patients who were doing well or had some noticeable problems increased to 92.2%. On CGI-S, at the time of enrolment 78.3% of the participants were moderately or markedly ill. However, after one month of treatment, none of the participants were markedly ill, only 21.6% were moderately ill, and 78.4% were either normal, borderline or mildly ill. This indicates that 56.8% of the participants had improved on follow-up. The CGI-I scores were measured at the time of follow-up. Results showed that the majority of the participants (51%) had much improvement, 19.1% showed very much improvement from baseline, whereas, 31.4% had minimal improvement, and at the time of follow-up.
Illness Characteristics.
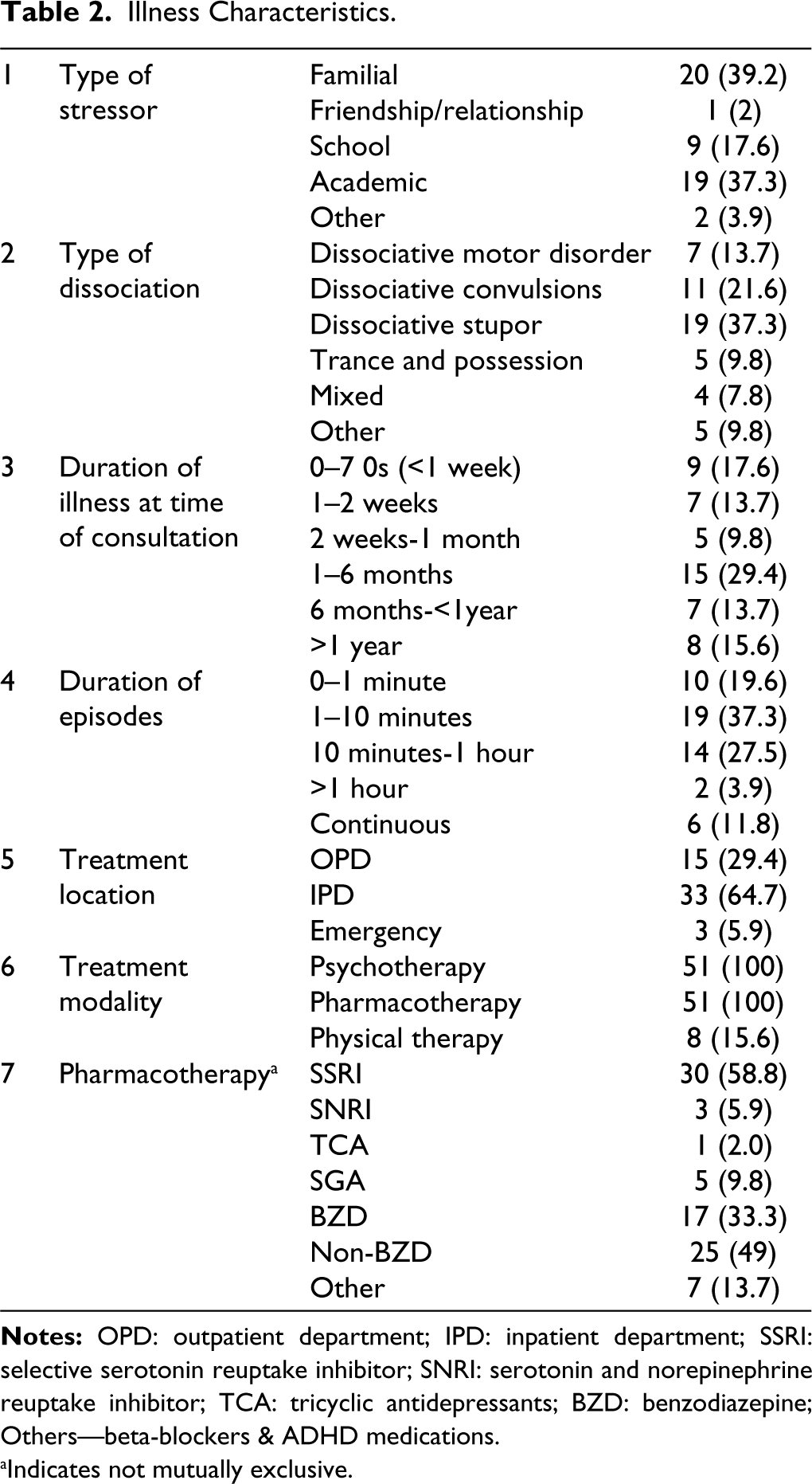
aIndicates not mutually exclusive.
Change in CGAS and CGI-S Score After 1 Month Follow-up.
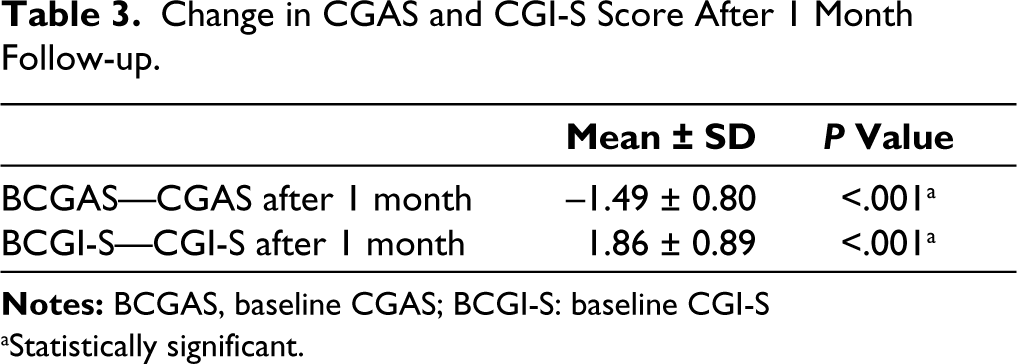
aStatistically significant.
Discussion
In our study, the mean age of the patients was 14.2 years (±2.050), and majority (66.7%) of patients were female. This was similar to Srinath et al. 13 and Sethi and Gandhi, 11 where 63 and 53% were from 12 to 16 age group, respectively. In Malhi and Singhi, 7 the mean age was lower, being 11 years, ranging from 8.2 to 14.6. Ani et al. 2 had median age of 12.5 years with range from 7 to 15 years. In another study by Malhi et al., 8 mean age was 10.2 year with 6–12 year age range. Adolescent age is also time of puberty and growth where they have face new situations, possibly contributing to the higher number. About 66.7% of participants were female as compared to 31.9% of male participants in our study. Only few studies such as Sethi et al. 11 and Ani et al. 2 had comparable female predominance (61% and 75%), whereas in other studies, most patients were boys, with Malhi et al. 8 reporting 60% of patients being boys, Srinath et al. 13 reporting 52% boys, and Malhi and Singhi 7 reporting male to female ratio being 1.6:1. Malhi and Singhi 7 have remarked that being a referral center in North India, where culturally males have preference for seeking treatment, could be a reason for the variance. Most of the patients had intrafamilial (39.2%) or academic stressors (37.3%). This is in line with study by Prabhuswamy et al., 10 where familial stressors was most common and Malhi et al. 7 noted the academic difficulties and parental issues were most common stressors. The preponderance for slow-to-warm up temperament in our study is possibly because these individuals may have deficits coping and adaptive skills, which can also predispose to dissociative disorders. We found a higher frequency of dissociative stupor in our study. We hypothesize that it could indicate higher levels stress in study subjects as stupor induces complete dissociation of conscious processes.
Majority of patients in our study showed significant improvement in their symptoms, as seen in the change in CGAS and CGI-S scores. The mean change in these scores was found to be statistically significant, indicating that more than half of the patients had significant improvement after one month of treatment. The majority of patients also showed some form of improvement in CGI-I scores. In a retrospective study, significant improvement in functioning on CGAS was observed at the end of one month. 8 In our study of improvement levels with CGI-I, 70% of patients had some form of improvement from baseline. This was in line with other studies; a quarter of the total patients had recovered within six weeks and 31.3% recovered within three months. 5 Similarly, in another study 9 93% of participants had complete remission in at one month. However, in these studies, no tools were used to assess improvement objectively. Overall, the outcome at the end of one month appears to be favorable as also in our study majority of patients showed improvement at the end of one-month follow-up.
Our study was conducted in a tertiary care hospital, where cases were mainly identified through referrals from medical and pediatric departments within and outside the hospital. Despite the limited sample size caused by the COVID-19 pandemic, all patients diagnosed with dissociative disorder received some form of treatment. Our study’s major advantage was the use of structured assessment tools, enabling a more objective assessment of outcomes. Additionally, we investigated variables such as temperament, parenting, and illness characteristics that have not been well studied previously. To minimize dropouts, we employed various modes of follow-up, although these tools may not be validated for voice calls. Overall, our findings provide valuable insights into dissociative disorders and can help inform future research and clinical practice.
Our findings are consistent with other studies that found improvement in symptoms after treatment. However, we used objective tools to assess improvement, which was not done in some of the previous studies. Overall, our study provides insights into the clinical profile and short-term outcomes of children and adolescents with dissociative disorders, emphasizing the need for further research in this area.
Conclusion
Our study adds to the limited literature on the clinical profile and short-term outcome of dissociative disorder in children and adolescents. Our findings suggest that dissociative disorder is not uncommon in children and adolescents in South India, and that with appropriate treatment, there can be significant improvement in short-term outcomes (1 month). Slow-to-warm-up temperament may be a possible risk factor for dissociative disorders in children and adolescents, although this needs further study. The study highlights the importance of early diagnosis and intervention, which may help prevent distress and dysfunction in the family. Further studies with larger sample sizes and longer follow-up periods are required to better understand the course of dissociative disorder in children and adolescents and to identify factors associated with good long-term outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee Jawaharlal Nehru Medical College Institutional Ethics Committee on Human Subjects Research. No MDC/DOME/44 dated 25/01/2021. Written/Verbal Informed Consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.