
Abstract
Background and Aim:
Vitamin B-12 plays a role in normal growth and development in childhood and adolescence. In this study, the effect of vitamin B-12 on attention was investigated.
Method:
A total of 138 participants who were admitted to the pediatric clinic during a three-month period between June 15, 2021, and September 15, 2021, between the ages of 9 and 16 years, who had their vitamin B-12 levels measured and met the inclusion criteria of the study were included in our study. D2 Attention Test data were obtained from the participants.
Results:
While 24.5% of the group with low vitamin B-12 levels had pathology according to the D2 Attention Test, 5.9% of the control group had pathology according to the D2 Attention Test. The percentage of pathology in those with low vitamin B-12 levels was statistically significantly higher than in the group with normal B-12 levels.
Conclusion:
It was observed that the attention level of the group with vitamin B-12 deficiency was lower. In the follow-up of healthy children, it is recommended to pay attention to the research on vitamin B-12 values.
Introduction
Vitamin B-12 (B-12, cobalamin) is an important nutrient for humans. In B-12 deficiency, neuronal demyelination is observed, affecting both the peripheral and central nervous systems. 1 Vitamin B-12 has been shown to play a role in maintaining the balance between neurotrophic and neurotoxic factors in the central nervous system. 2 Increased homocysteine in vitamin B-12 deficiency can induce neuronal DNA damage.3,4 In a study conducted in adults, spatial copying performance was found to be lower in those with vitamin B-12 deficiency. 5
During childhood and adolescence, attention plays an important role in the social and mental development of children. Neurological findings observed in the case of B-12 deficiency can be listed as sensory changes, paresthesia in the extremities, dizziness, psychiatric problems, memory problems, personality problems, growth retardation, decrease in activity, and developmental delay. 6 In the studies carried out, it was concluded that there is a connection between the level of vitamin B-12 and the neurocognitive development processes of children. In a study, it was observed that the Bayley Scales of Infant Development II (BSID-II) mental development scores increased significantly as plasma vitamin B-12 concentrations increased. In middle childhood, low vitamin B-12 levels were linked to behavioral problems in teenage boys. 7 According to a study conducted in Taiwan, vitamin B-12 levels were significantly lower in children with attention deficit hyperactivity disorder (ADHD) than in healthy children. 8 When compared to the control group, children with ADHD had significantly lower levels of homocysteine, pyridoxine, folate, and vitamin B-12. 9 In a large US study, the Wide Range Achievement Test-Revised and the Wechsler Intelligence Scale were used to assess cognitive function, and no relationship was found between B-12 and cognitive function. 10 There are different results in studies regarding vitamin B-12 and cognitive effects. There are a limited number of studies evaluating attention using the D2 Attention Test in children and adolescents with B-12 deficiency. The study elicited the association between plasma levels of vitamin B-12 and the performance on the D2 Attention Test among children aged 9–16 years.
Material and Method
Participants
The G Power program was used to calculate a sample from the study population. When the power was 0.80, the alpha (margin of error) was 0.05, and the effect size was 0.55, the number of samples needed in a two-way hypothesis was calculated as 53 for the first group and 53 for the second group. We had planned to reach a minimum of 106 people. In this study, we reached a total of 138 people, 53 in the first group and 85 in the second group.
Inclusion Criteria
The clients who applied to the well-child clinic where they underwent routine check-ups and developmental control and participants who had their vitamin B-12 level measured, volunteered to participate in the research, and were between the ages of 9 and 16 years were included in the study.
Exclusion Criteria
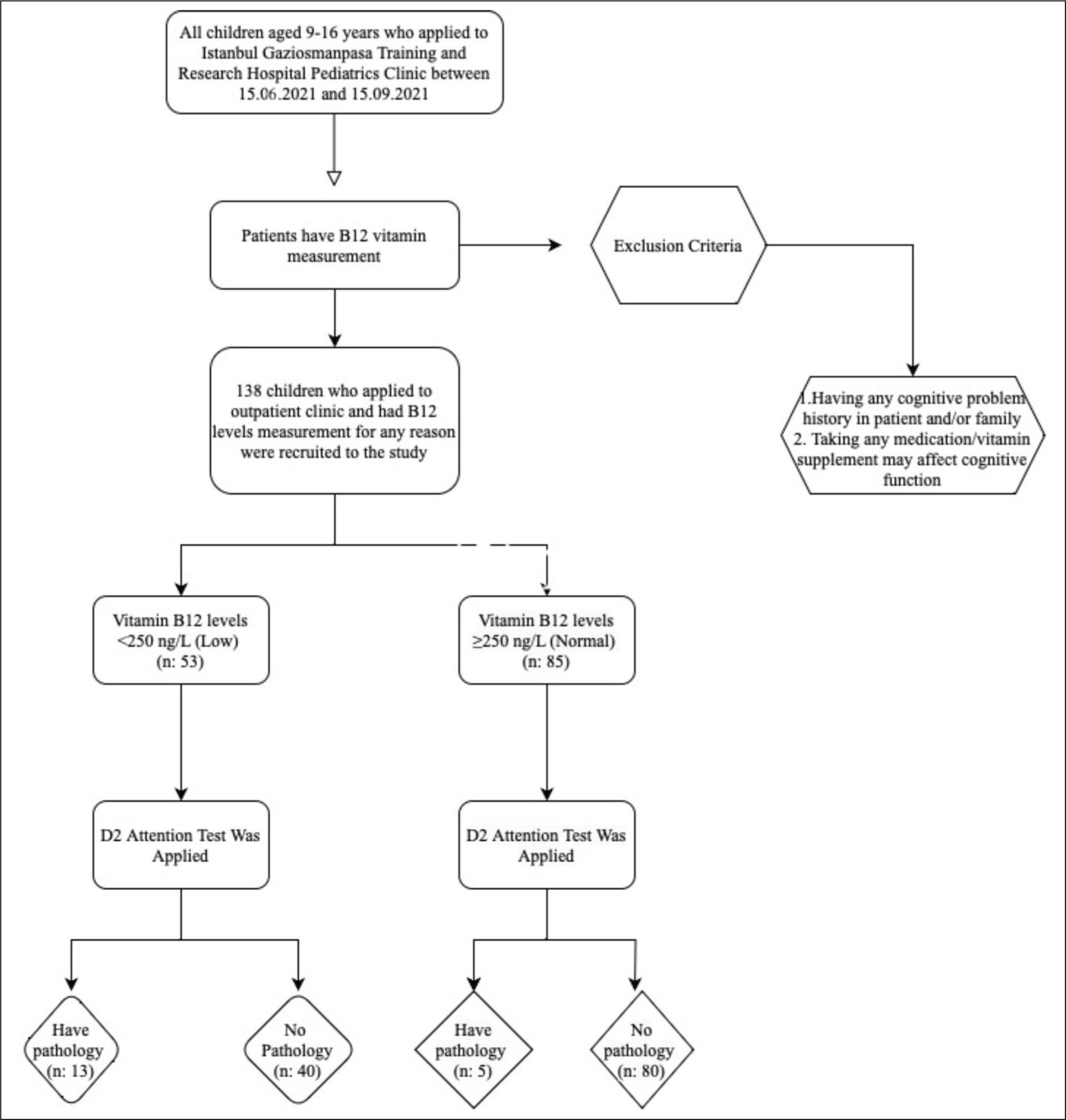
The presence of chronic diseases (metabolic syndrome, genetic disorders, chronic cardiac problems, endocrine disorders, etc.), having a history of any disease that causes a problem in cognitive function (stroke, head trauma, epilepsy, tumor, etc.), being on any psychiatric medication, and participants already receiving B-12 therapy were excluded (Figure 1).
Study Participant Flow Chart.
Procedure of Recruitment
It was a hospital-based cross-sectional study done between June 15, 2021 and September 15, 2021. Participants aged 9–16 years old who applied to the well-child clinic (in a training and research hospital in Istanbul) and whose B-12 levels were measured were examined. D-2 Attention Test was conducted for these children. A total of 138 participants were selected as the case with vitamin B-12 levels below 250 ng/L and the control group with 250 ng/L and above. A cut-off value was obtained from the reference article. 11
Confounding Factors
During routine check-ups, all complaints at the well-child clinic consisted of fatigue, loss of appetite, inability to gain weight, and short stature. Demographic data, age, gender, BMI, number of siblings, family income, and mother and father education variables that may be found as confounding factors did not show any significant difference between groups with and without B-12 deficiency. Variables such as the school type, classroom, and region where the children were educated, which could be other confounding factors, could not be evaluated in our study.
Study Tool
Sociodemographic data and laboratory results of the individuals were recorded. The blood tests used in the study were examined in the training and research hospital laboratory. Sociodemographic data, age, gender, family’s education level, economic status, and questions were designed to be filled in by the family and child during the application by taking a physical printout. The data collected by the researcher according to the statements of the families consisted of the following: children’s physical activity; type of sportive activity (normal sporting activity or professional sports activity); activity duration (less than half an hour a day or more than half an hour a day); meat consumption status (every day, per week, per month, and does not consume); school grade point average (last six months); and average daily screen exposure time (hours).
Evaluation of Attention
Data were obtained by applying the D2 Attention Test to the participants. The D2 attention test allows to measure selective attention in a time-dependent manner. It can be applied to people between the ages of 9 and 60. At the end of the test, six points were obtained: TN (total number of marked lines), E1 (number of unmarked omitted figures), E2 (number of incorrectly marked figures), CP (total number of marked lines), TN-E (test performance), and E% (rate of errors). 12 When calculating the TN-E score, the TN-(E1 + E2) formula was used. The FR score corresponding to the TN-E score obtained was checked. If it was above 25%, it indicated normality; if it was below 10%, there was pathology; 10%–25% was considered low attention; 25%–75% was normal; 75%–90% was good; and 91%–97.1% was high attention. The test was carried out by a child development specialist.
Brickenkamp created the D2 Attention Test, which gauges selective attention based on time. 13 Toker translated the D2 test into Turkish for children aged 11–14. 14 Following a reliability analysis and a test-retest procedure three months later, it was discovered that TN-E (total performance) had a value of r = 0.77. In the validity study, a significant (r = 0.44) correlation was found between the Wechsler Scale and the D2 test sub-dimensions. 15
Statistical Analysis
Analyses were conducted using version 22.0 of the SPSS (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL) program. In order to compare categorical variables between groups, chi-square (Pearson and linear by linear) analysis was utilized. The Kolmogorov–Smirnov test was used to assess the conformity of continuous variables. In the comparison of paired groups, the Mann–Whitney U-test was used. Spearman correlation analysis was used when evaluating the relationship between two continuous data. The analysis’s P = .05 cutoff for statistical significance was approved.
Results
The study included 53 children with vitamin B-12 deficiency as a case group and 85 healthy control groups. Of those in the group with vitamin B-12 deficiency, 31 (58.5%) were female and 22 (41.5%) were male. In the control group, 51 (60%) were female and 34 (40%) were male. The mean age of the vitamin B-12 deficient group was 13.6 ± 2.3, and the mean age of the control group was 12.8 ± 2.6. There was no significant difference between the groups in terms of gender (P = .861), age (P = .09), height (P = .114), weight (P = .065), BMI (P = .254), and BMI percentile (P = .528). Also, 13.2% of those in the vitamin B-12 deficiency group and 6% of those in the control group were born prematurely. The mean number of siblings of the vitamin B-12-deficient group was 2.2 ± 1.1, and the mean number of siblings of the control group was 2.2 ± 1.2. There was no significant difference between the groups in terms of prematurity (P = .214), the number of siblings (P = .632), family income (P = .052), parents living together (P = .766), mother’s education level (P = .759), and father’s education level (P = .930). Moreover, 94.3% of those in the vitamin B-12 deficiency group and 94% of those in the control group were breastfed. The mean duration of breastfeeding was found to be 17.7 ± 7.5 months in the vitamin B-12-deficient group and 18.6 ± 9.0 months in the control group; 23.1% of the vitamin B-12-deficient group and 30.6% of the control group did regular physical activity. The school grade average for the last six months was 75.9 ± 14.7 (75.5) in the vitamin B-12-deficient group and 79.2 ± 12.5 (80.0) in the control group. There was no significant difference between the groups in terms of breastfeeding (P = .943), breastfeeding time (P = .697), regular physical activity (P = .341), sportive activity type (P = .591), activity duration (P = .858), meat consumption status (P = .122), and school grade average (P = .201).
There was no significant difference between the B-12 deficiency group and B-12 normal group in terms of blood values (P > .05) (Table 1).
Comparison of the Laboratory Parameters of the Groups.
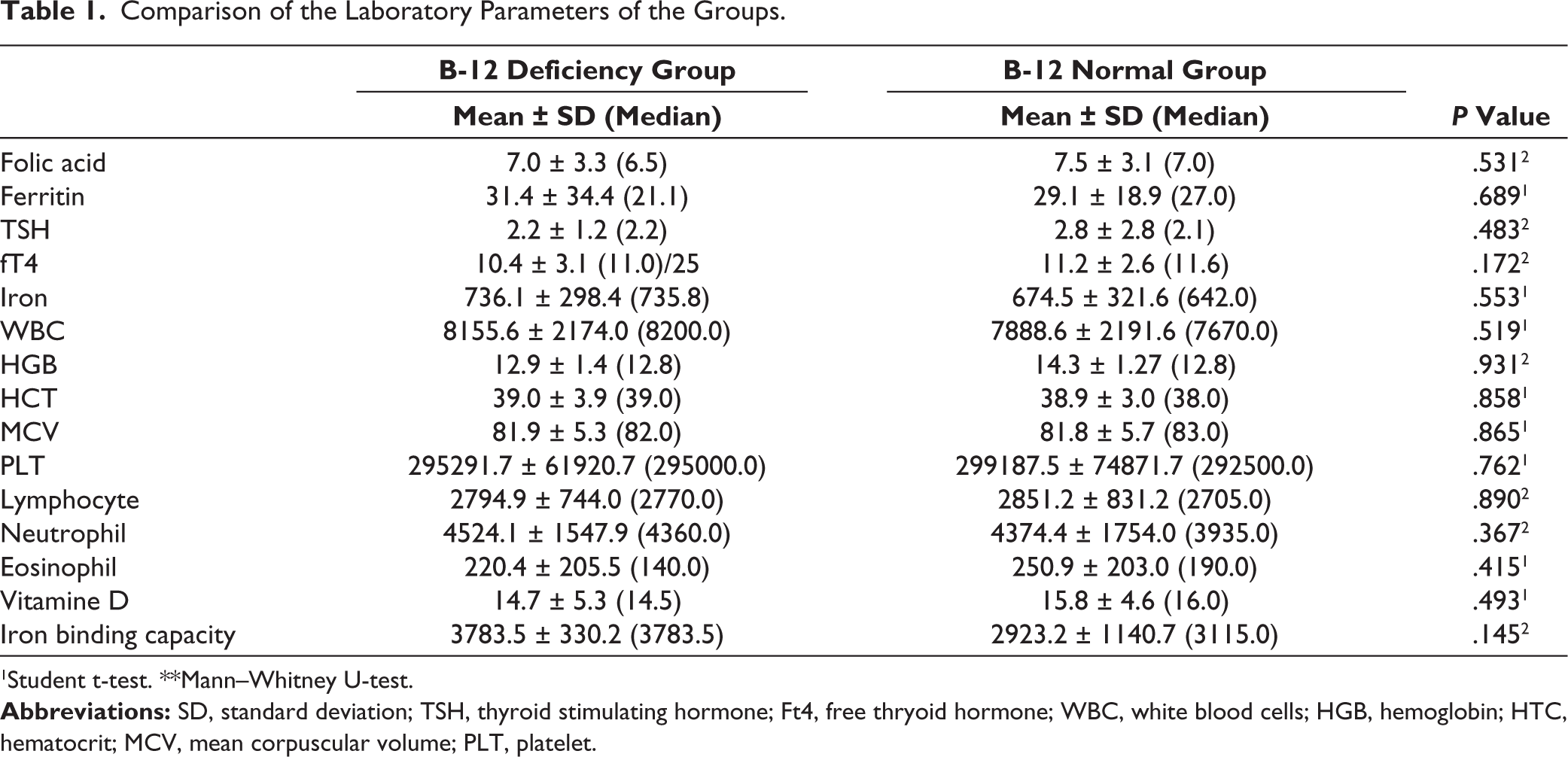
1Student t-test. **Mann–Whitney U-test.
When divided into two groups—those with pathology in attention and those without pathology in attention—the mean B-12 in the group with pathology (238.9 ± 92.3) was lower than that in the other group (299 ± 105.6) (P = .007). B-12 level was found to be statistically significantly different in both groups (Table 2). In the attention level assessment grouping created by looking at the TNE score, 24.5% of those in the group with low vitamin B-12 levels had pathology, while 5.9% of the control group had pathology (P = .029) (Table 3).
Comparison of Attention Groups with Parameters.
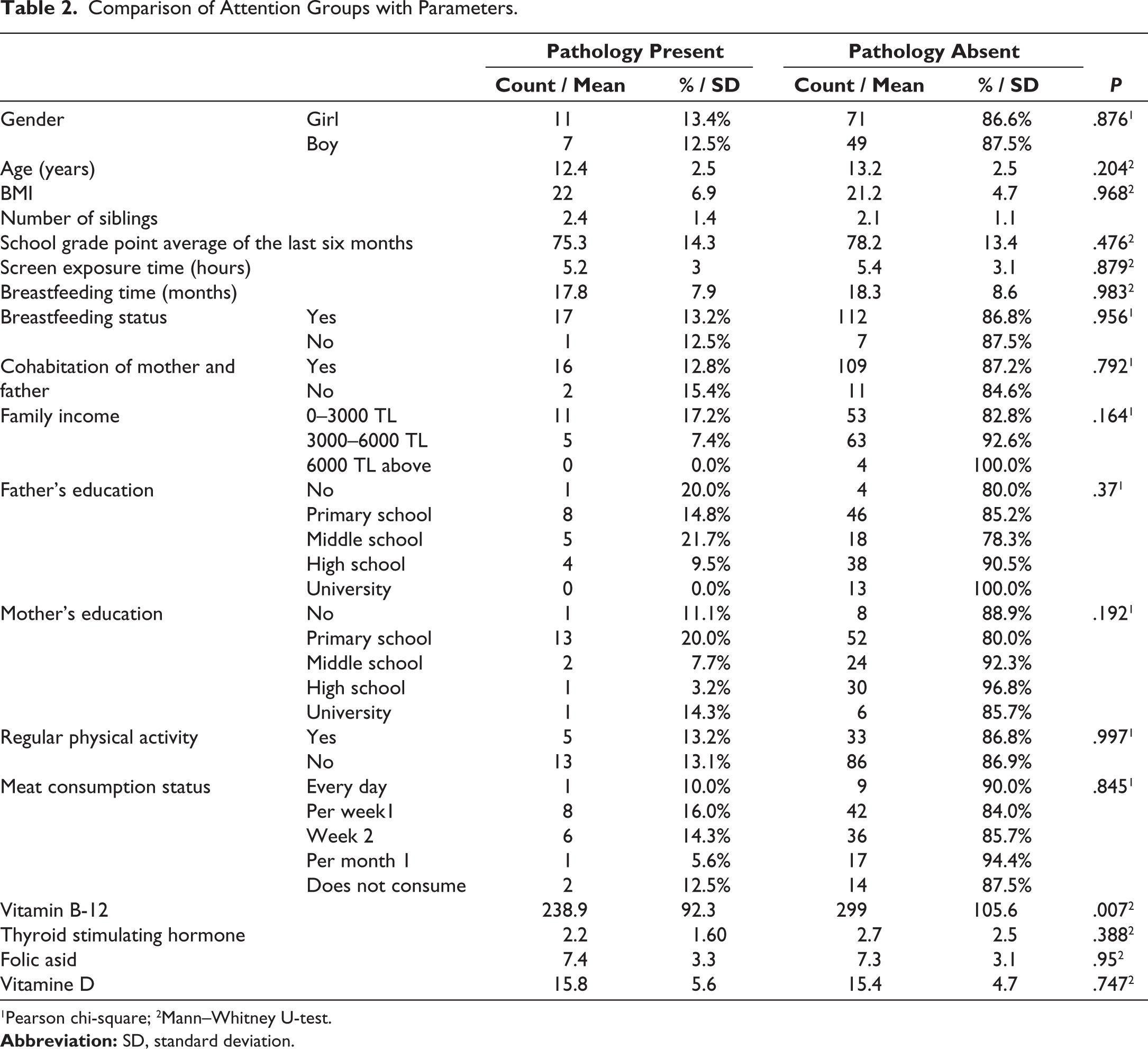
1Pearson chi-square; 2Mann–Whitney U-test.
Comparison of Attention Groups with B-12 Level.
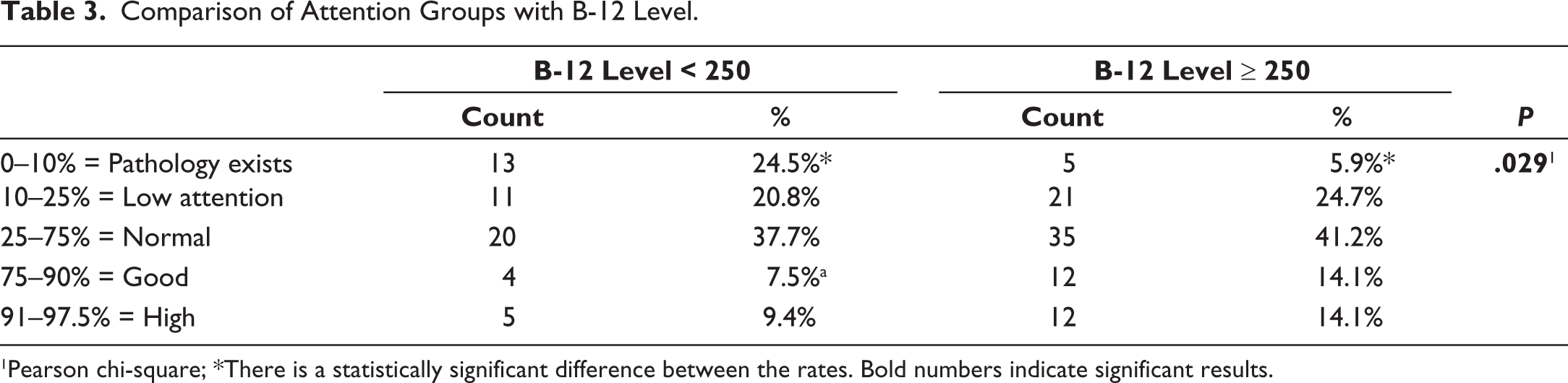
1Pearson chi-square; *There is a statistically significant difference between the rates. Bold numbers indicate significant results.
There was no significant difference between attention groups in regular physical activity, meat consumption status, genders, grade point average for the last six months, screen exposure time, and other blood values (Table 2).
In the attention test, when the group with pathology and the group with low attention were evaluated together and compared with other groups, it was found that the prematurity of the child had an effect on attention. Pathology in attention and low attention was observed in 66.70% of the children who were born prematurely and 32.80% in the children who were born maturely (P = .019).
Pathology in attention and low attention was observed in 60.00% of the children of fathers who were uneducated, in 44.40% of the children of fathers who were primary school graduates, in 34.80% of the children of fathers who were secondary school graduates, in 31.00% of the children of fathers who were high school graduates, and in 15.40% of the children of fathers who were university graduates. When the course was evaluated using the linear-by-linear analysis, it was seen that as the father’s education level increased, the rate of low attention and attention pathology in the child decreased (P = .021) (Table 4).
Comparison of Attention Pathology and Low Attention Groups with Other Groups.
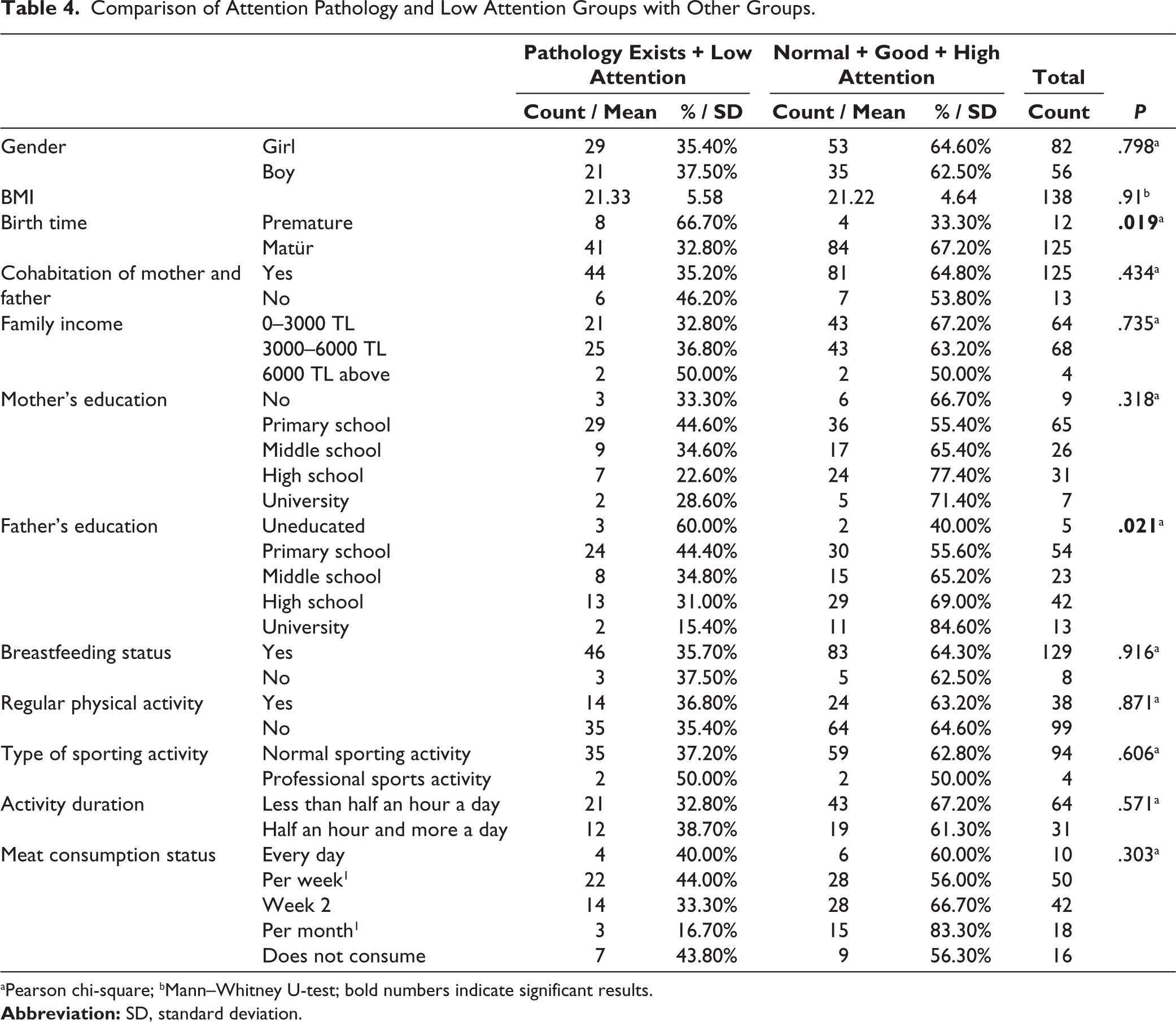
aPearson chi-square; bMann–Whitney U-test; bold numbers indicate significant results.
The total number of marked lines and age (positive), number of unmarked omitted figures and number of siblings (positive), rate of errors and age (negative), total score and HCT (positive), and correlation were observed (Table 5).
Correlation of Attention Test with Other Parameters.
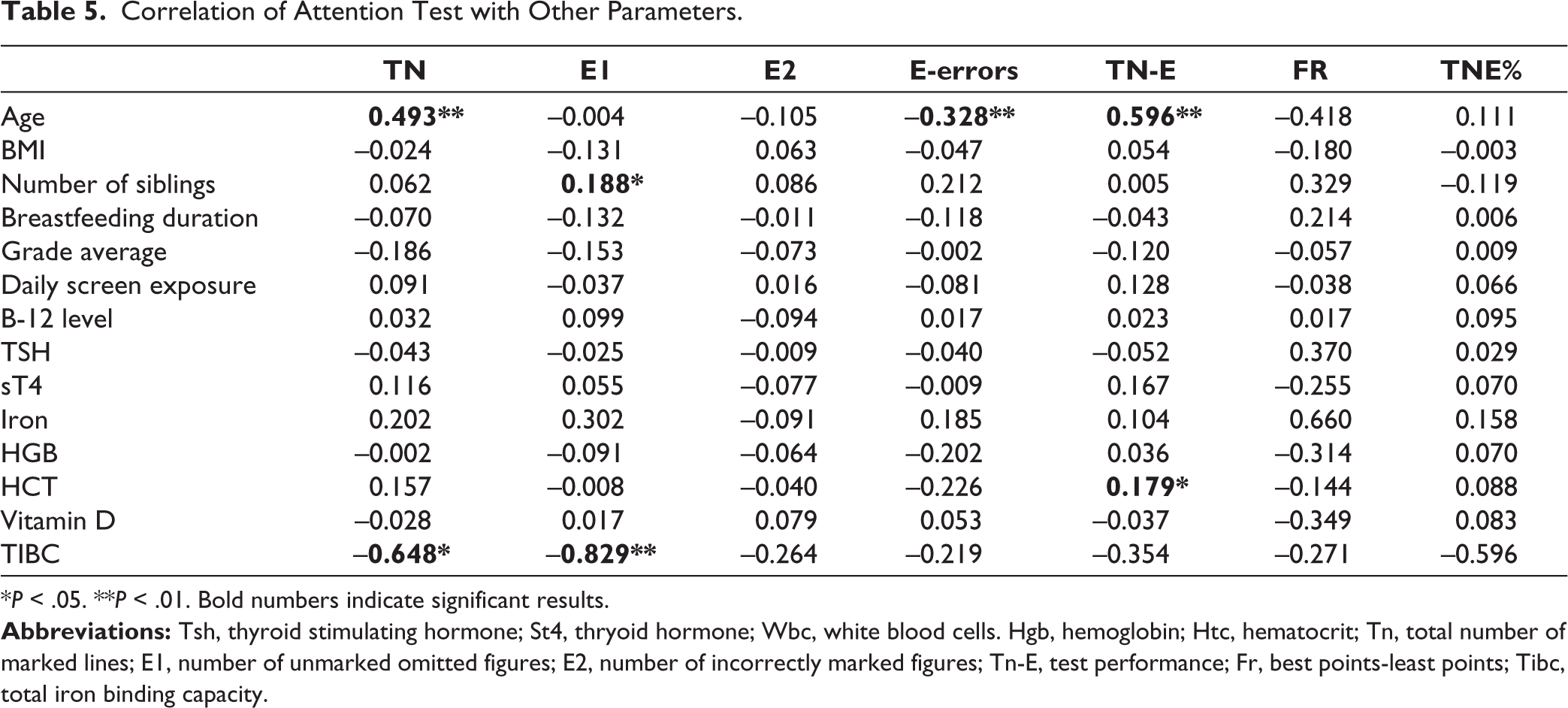
*P < .05. **P < .01. Bold numbers indicate significant results.
Discussion
Attention, with its most general definition, is a “neural system” activity that helps to deal with the many stimuli in the environment that it needs only at that moment and in line with its goals. 16 This study aimed to determine whether there is a relationship between vitamin B-12 deficiency and attention. In a study conducted by Meins et al., behavioral and psychological symptoms of groups with and without vitamin B-12 deficiency were compared, and in this study, no significant difference was found between the groups in terms of age and gender. 17 In our study, there was no significant difference between the case and the control group in terms of gender and age. This enabled the elimination of independent variables that could be a confounding factor in comparing groups in terms of attention.
Some molecules, such as iron, thyroid hormones, and vitamin D, play an important role in the development of attention in children. During iron deficiency, a decrease in attention is observed as a result of neurophysiological changes, the cause of which is unknown. 18 Moreover, a negative correlation was observed between Phyto-iron and zinc intake and ADHD scores. 19 Our study is the first to directly measure only the relationship between attention and vitamin B-12 in children, keeping other blood parameters constant. When the effects of other blood parameters on attention were examined in our study, total score and HCT (positive) correlation were observed. In other words, as HCT increases, the total score success increases.
According to Allen et al., cobalamin insufficiency was linked to impaired neuromotor and cognitive functioning, as well as poorer academic results, lower teacher evaluations, and more attention issues. 20 Vitamin B-12 deficiency, which is in the micronutrient group, can affect cognitive function. Studies in children are limited, especially in early childhood. Strand et al. looked at the association between cognitive function in 12- to 18-month-old North Indian infants and plasma concentrations of folate, cobalamin, total homocysteine, and methylmalonic acid. The mental development index score rose by 1.3 points for every twofold increase in plasma cobalamin content. 21 Eight Norwegian secondary schools (n = 415; age: 14–15 years) were asked to take fish dishes, meat dishes, or n-3 LCPUFA supplements three times a week for a total of 12 weeks, involving adolescents. 22 Attention performance was evaluated with the D2 Attention Test, and there was no difference between nutritional status and D2 Attention Test scores. 22 Meat consumption did not affect attention in our study. As can be seen in the literature, studies have been conducted based on nutritional habits in general, and conflicting results have been observed. It is also important to reveal the results with a valid and reliable test.
Studies show that there may be a relationship between school success and intelligence and vitamin B-12 level. However, this relationship has not been fully proven. A prospective study found that vitamin B-12 intake was positively associated with memory test scores in Kenyan school-aged children, whereas in cross-sectional National Health and Nutrition Examination Surveys in the United States, vitamin B-12 concentrations were not associated with reading test scores in children aged 6–16 years.10,23 In a study conducted by Duong et al., it was found that vitamin B-12 deficiency is a risk for both school failure and school absenteeism. In a cross-sectional study conducted in Israel, including 67 primary school children (9–11 years old), children’s serum vitamin B-12 concentrations (serum vitamin B-12 < 200 pg/mL) were compared with their academic achievement. In this study, it was determined that one quarter of the children had low serum vitamin B-12 concentration, and a significant positive relationship was found between vitamin B-12 concentration and academic achievement. 24 In our study, it was observed that the GPA (grade point average) of the case group with vitamin B-12 deficiency was lower than the GPA of the control group, even though it was not statistically significant. The reason that the relationship between GPA and attention could not be determined may be because children are educated in different places and types of schools and classes. The children were in different classes and at different ages and went to different educational institutions. Due to these differences, GPAs may not reflect school achievements objectively. Many different reasons can affect attention, such as the economic situation of the country. In a study conducted in South Africa with 835 children between the ages of 8 and 12 years, children infected with soil-transmitted helminths had lower selective attention, lower school grades (academic achievement scores), and lower cognitive strength. 25 Sleep patterns may also have an effect on attention. In a study, the success of students who slept one hour more per day in the “Mathematics Continuous Performance Test” and the “D2 Test of Attention” increased. 26
As age increases, there are changes in attention. In the study conducted by Çağlar and Koruç, it was observed that as age increased, psychomotor speed, total test performance, and concentration performance scores also increased. 15 In a study conducted by Culbertson and Sari, it was found that there was a significant positive correlation between the ages of the children and their psychomotor speed and concentration performance scores. 27 Schaefer et al. found that the psychomotor speed and total test scores of the D2 test of older gymnasts were significantly higher than those of younger gymnasts. 28 In our study, a positive relationship was found between age and TN score and TNE score, and a negative significant relationship was found between age and E-error score. As age increases, positive performance on the D2 Attention Test increases. Since the children included in the study were close to adolescence, their physical and neurological development continued, so it was expected that the attention test scores of older children will be better.
It is clear that attention is a very complex phenomenon, and many physical factors and even birth history can be effective. In our study, in the attention test, it was found that the prematurity of the child had an effect on attention. In one study, the cognitive profiles of 12 students with obesity were compared with their normal weight peers. Children with obesity performed worse on the D2 and Wisconsin tests. 29 There was no relationship between BMI and attention in our study. Moreover, it has been shown that improving physical fitness can support the development of different aspects of cognitive functions and, in particular, attention. 30 In a study conducted with children aged 10–12 in Spain, the group that performed more weekly physical activity took less time on simple and complex reaction time tests. 31 In a study examining the academic success of sports in children using the D2 Attention Test, it was observed that school lessons were positively affected by sports. 32 In another study conducted in Spain, in which the effect of physical activity on attention in adolescents was examined with the D2 Attention Test, regression analysis showed that oxygen consumption was the best predictor of attention parameters. 33
Families’ approach to children is very important in their spiritual and physical development. The education level of the family may be important in the family’s approach. In our study, it was seen that the educational status of the father was effective on the child’s attention. It was observed that as the education level of the father increased, the state of pathology or low attention rate decreased. In addition, family approach may have an impact on children’s communication style. In a study involving primary school students, positive relationships were found between assertive communication style and D2 Attention Test performance. Kids who communicate assertively tend to pay attention better than kids who communicate passively or aggressively. 34 In our study, the number of unmarked omitted figures and the number of siblings were found to be (positively) related; that is, as the number of siblings increases, the number of unmarked figures errors increases. When the number of siblings increases, the amount of time parents spend with the child decreases, which may cause the error to increase.
As we found in our study, it is noteworthy that screen exposure is quite high in children aged 9–16 years. Families should be educated about the limits of screen exposure, proper and regular nutrition, and factors affecting attention in children. It is necessary to increase parents’ interest and follow-up about the child’s school success and academic and social activities and to encourage them to consult a professional in cases where problems are observed in the child.
Strengths and Limitations
Since the study was conducted with participants admitted to the hospital, a full community representation may not have been achieved. Since it is not a prospective study, the inclusiveness of our study is lower due to the nature of the study. Attention span is also influenced by a range of other factors, which were not controlled in the study. It can be affected by many factors, such as genetic status, family conflicts, environmental effects, national and regional effects, school type, and education level. Among the participants who came to the well-child clinic, those with symptoms had complaints of fatigue, loss of appetite, inability to gain weight, and short stature. This may affect the reliability of the test. No standard tool was used to assess diet and exercise parameters. Information was obtained by asking the parents whether the participants engaged in normal sports activities or professional sports activities. The type of sport and the type of meat consumed by the participants were not elaborated upon.
Conclusion
In the follow-up of healthy children, it is recommended to pay attention to the research on vitamin B-12 values. It is necessary to inform pediatricians, family physicians who follow up with healthy children, and child psychiatrists about the D2 Attention Test and to increase attention test screenings in children. Our study has once again demonstrated that primarily organic causes should be investigated in children and adolescents with low attention levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Gaziosmanpaşa Training and Research Hospital Clinical Research Ethics Committee (09.06.2021/Approval No.: 291). The Declaration of Helsinki was followed when conducting the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
We received written informed consent from the participants and for publishing the study.