
Abstract
Behavioral parent training is the recommended intervention for young children with disruptive behavior and/or attention-deficit/hyperactivity disorder (ADHD). Parent–child interaction therapy (PCIT) is an empirically supported behavioral parent-training program for families of children ages 3–6 years old.
Behavioral parent-training programs, including PCIT, rely on parents as the primary agents of therapeutic change. Parents who face barriers to adequate engagement with these programs may also struggle to implement the changes necessary for children’s behavior to improve. Parental characteristics that may prevent treatment engagement, however, are seldom considered in the research literature or in clinical practice.
The current case series describes engagement indicators in three mothers taking part in PCIT. Each mother has a history of diagnosed or suspected ADHD, and this series explores their ADHD-related symptoms as they relate to the treatment of their child’s behavior.
Keywords
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by inattention and/or hyperactivity and impulsivity across settings. 1 Parents of children with ADHD are at a higher risk of having ADHD themselves.2,3 As a result, the rates of ADHD in parents taking part in parent training may be higher than the rates of adult ADHD in the general population. Yet, no known studies have examined the relationship between parental ADHD and parental engagement in parent training among families involved in the treatment for preschool children.
Though many studies have examined factors that impact treatment engagement in families of young children, the impact of parental ADHD has not been explored in this population. 4 One study of treatment engagement factors among parents of children aged 7–11 found that parents with higher ADHD symptoms demonstrated reduced treatment homework completion. 5 High levels of maternal ADHD symptomology also have been associated with a lack of improvement in child behavior following parent training with school-aged children. 6 Specifically, mothers who have ADHD continue to utilize less-favorable strategies, such as giving ineffective commands, asking questions, and criticizing their children’s negative behavior, despite treatment focusing on the use of alternative strategies. 7 Understanding the relationship between parental factors and parent behavioral management training success is necessary to promote the best outcomes for children.
Parent behavior management training, including PCIT, is a behavioral intervention with strong research supporting efficacy in reducing childhood disruptive behavior, decreasing parenting stress, and increasing parental self-efficacy. 8 Meta-analytic reviews suggest that in vivo feedback (“coaching”) is one of the most effective components of behavioral parent training. 9 PCIT is novel because the majority of treatment time is devoted to the therapist providing this in vivo coaching to caregivers. For preschool-aged children with ADHD, PCIT is characterized as a well-established evidence-based behavioral treatment. 10
PCIT is composed of two treatment phases. The child-directed interaction (CDI; typically 4–6 weeks) is the first phase, serving to increase parents’ use of positive attending skills and selective attention. The parent-directed interaction (PDI; typically 6–8 weeks) phase of therapy follows, focusing on consistent implementation of discipline strategies for non-compliance to parental direction. Successful treatment completion is predicated on (a) consistent session attendance to allow caregivers to learn the skills through live coaching and (b) daily practice of the skills with their child in a 5-minute therapeutic play session at home. Families progress through treatment when (a) parents demonstrate acquisition of the target skills as evidenced by the therapist’s coding of parent–child interactions in sessions using a standardized coding procedure and (b) the child’s behavior improves to within normal limits on a standardized parent report measure. Most PCIT sessions involve the parent and child interacting together, with the parent practicing the targeted skills while the therapist provides in vivo parent coaching via an earpiece while observing remotely. 11
Understanding the impact of ADHD symptomology on parents’ engagement in PCIT may help elucidate the challenges parents with ADHD face when participating in parent training programs. Identification of specific barriers can help researchers and clinicians develop treatment tailoring strategies to increase effectiveness with parents displaying ADHD symptoms.
Measures
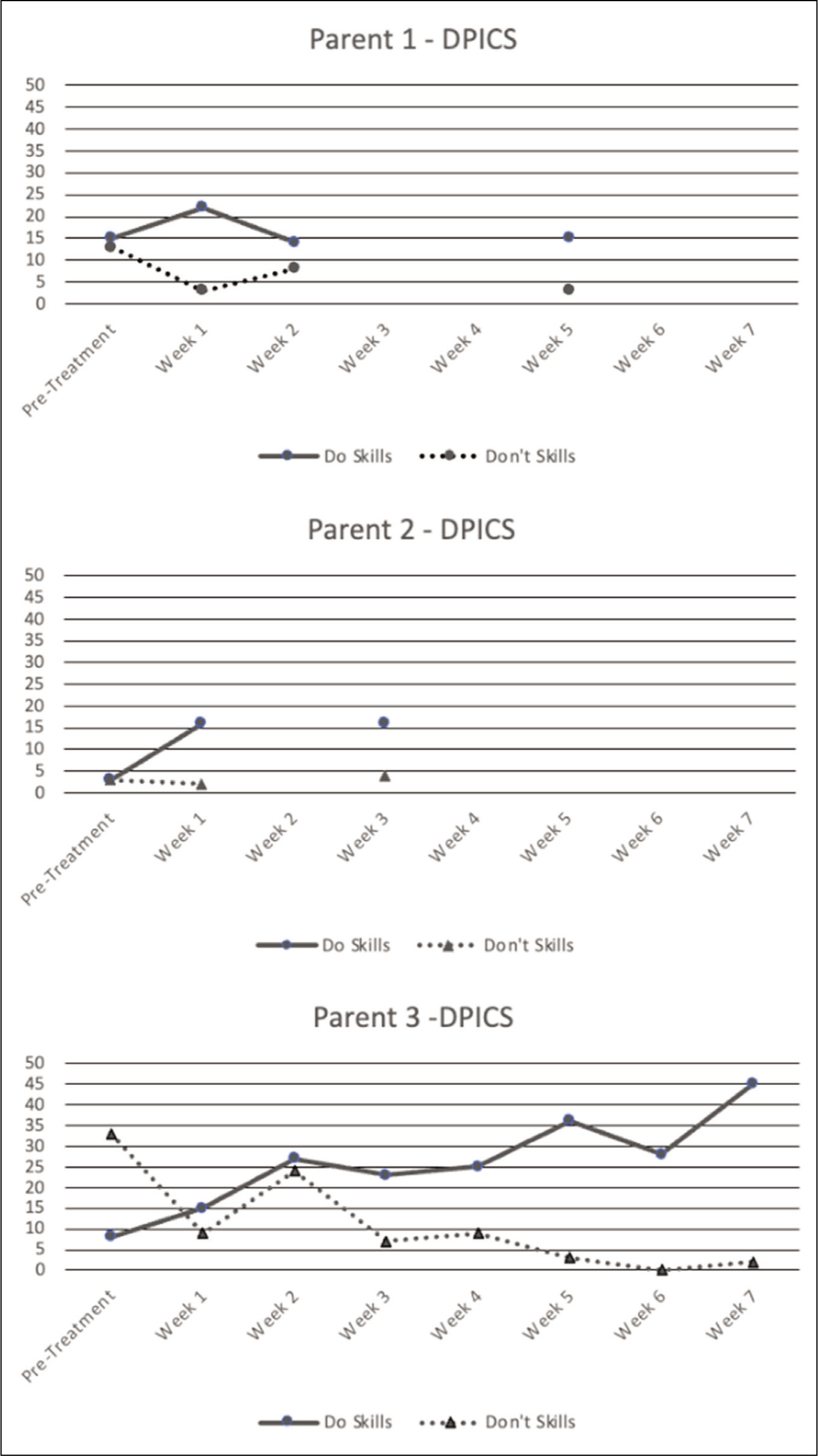
Positive and negative parenting behaviors (referred to as “Do Skills” and “Don’t Skills”) were assessed using the Dyadic Parent–Child Interaction Coding System, 4th Edition (DPICS-IV) 12 at the beginning of each therapy session. Child behavior problems were assessed using the Eyberg Child Behavior Inventory (ECBI), a parent-report questionnaire administered in each PCIT session. 13 To evaluate for parental symptoms of ADHD at pretreatment, parents completed the Conners’ Adult ADHD Rating Scale, Short Form (CAARS-SF), a self-report measure of ADHD symptomology. 14 They also completed at pretreatment the Behavioral Rating Inventory of Executive Functioning, Adult Version (BRIEF-A), a self-report measure of executive dysfunction. 15 All measures have strong psychometric properties and clinical utility in their respective domains.
Case Descriptions
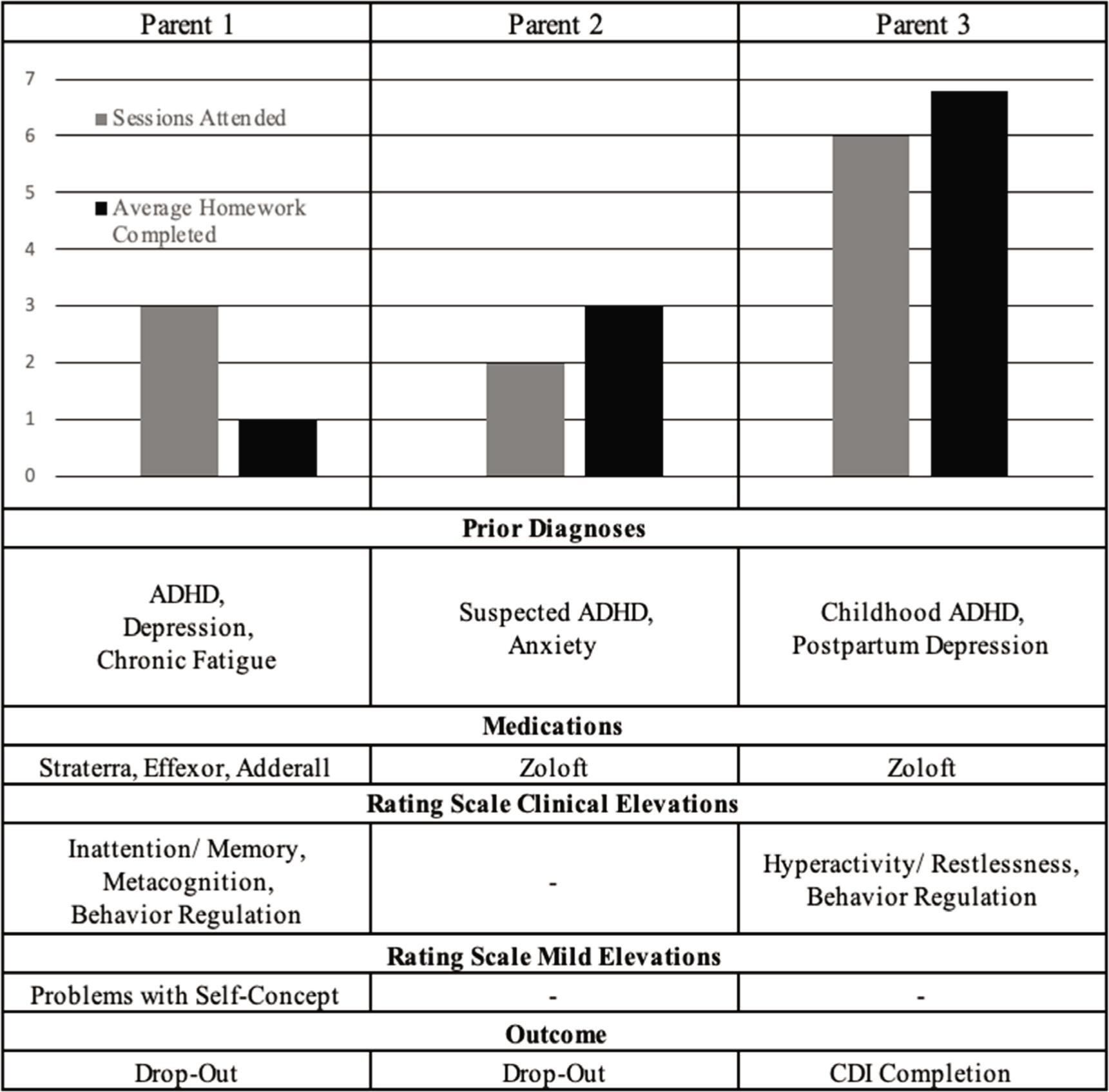
All families included children between 3 and 6 years old with ADHD. Figure 1 provides a comparison of each caregiver. All families received standard PCIT. 11
Summary of Parents’ Treatment Engagement, Diagnoses, and Symptom Ratings.
Mother 1
Caregiver characteristics: Mother 1 was a white, non-Hispanic woman in her early 40s. She was married and had a graduate-level education. She reported prior diagnoses of ADHD and depression. At PCIT initiation, her medications included a stimulant and two serotonin and norepinephrine reuptake inhibitors (SNRIs; one of which is often prescribed to treat ADHD). She also reported that chronic fatigue syndrome impacted her attention and memory. At pretreatment, CAARS-SF results indicated that Mother 1 was experiencing significant symptoms of inattention and/or memory problems, as well as mild concerns with self-concept. Symptoms of hyperactivity/restlessness and impulsivity/emotional lability were not elevated at pretreatment. However, on the BRIEF-A, self-reported executive functioning was problematic, with concerns in metacognition and behavioral regulation noted.
Treatment course: Mother 1 attended three CDI Coach sessions over 5 weeks. After the fifth week, she and her child dropped out of treatment for unknown reasons. She completed an average of 1 day (out of 7 prescribed days) of Special Time homework per week. Her positive parenting skill acquisition was variable, and total values in this area never reached expected frequencies. However, in week 1 and week 5, her use of the Don’t skills was reduced to zero, which met the specified goal criterion. Parenting skill acquisition for all caregivers is presented in Figure 2. Mother 1’s ratings of her child’s behavior on the ECBI increased slightly from 135 at pretreatment to 136 at week 5 (the last attended session). Both of these scores were in the clinical range.
Mother 2
Caregiver characteristics: Mother 2 was a white, non-Hispanic woman in her late 30s. She was married and had a bachelor’s-level education. She reported a prior diagnosis of anxiety and concerns about ADHD symptoms. At the time of data collection, she was being treated with an SSRI. Mother 2’s ratings on the BRIEF-A and CAARS-SF did not indicate clinically significant problems with ADHD symptoms or executive skills.
Treatment course: Mother 2 attended two sessions over the 7-week observation period. She dropped out of treatment after week 3. For the weeks she participated, she completed an average of 4.5 days (out of 7 prescribed days) of Special Time homework.
At pretreatment, Mother 2 used few Do or Don’t skills, and in fact, she made few verbalizations at all while playing with her child. Her use of Do skills increased over the two sessions she participated in, but never reached the goal criteria. Mother 2’s use of the Don’t skills remained low throughout treatment. Mother 2’s ratings of her child’s behavior on the ECBI increased slightly from 115 at pretreatment to 119 at week 3 (the last attended session). Both of these scores are above average, but not clinically elevated, and a four-point difference may not be meaningful.
Mother 3
Caregiver characteristics: Mother 3 was a white, non-Hispanic woman in her early 30s. She was married and had a bachelor’s-level education. She reported a prior diagnosis of postpartum depression and a childhood diagnosis of ADHD. Her ADHD symptoms have not been reassessed or treated since childhood. She was treated with an SSRI at pretreatment, and she reported no other medical conditions. On rating scales, Mother 3 reported significant symptoms of hyperactivity on the CAARS-SF and challenges with behavioral regulation on the BRIEF-A.
Treatment course: She attended seven sessions over the 7-week observation period. She completed an average of 6.75 days (out of 7 prescribed days) of Special Time homework per week. Mother 3 achieved CDI criteria during the observation period. Her use of two of the three Do skills increased quickly, but it was not until the seventh week that her use of all three Do skills met goal criteria (i.e., 10 labeled praises, 10 reflections, and 10 behavioral descriptions during a 5 min coding period). Mother 3’s use of Don’t skills trended down over the observation period, reaching zero at session five and remaining low thereafter. Mother 3’s ratings of her child’s behavior improved significantly during treatment. To account for variability in ratings across time points, score averages are provided for this parent. The average rating of her child’s behavior problems at pretreatment and Session 1 was 169, which is clinically elevated. Ratings from the sixth and seventh sessions averaged 123.5, which is above average but not clinically elevated.
Discussion
This case series described the PCIT treatment trajectories of three families in which the participating mother reported diagnosed or suspected ADHD. Although mothers reported varied timing and degrees of ADHD symptomatology, understanding their experience in PCIT is important considering the lack of data available on treatment engagement among mothers with ADHD who have young children with ADHD. Special attention was given to markers of treatment engagement in these families, especially attendance, attrition, and homework completion.
The experience of the families in our series is consistent with findings demonstrated in the research literature. Studies examining drop-out in PCIT estimate attrition rates ranging from approximately 18% in carefully controlled university efficacy trials to 69% in community effectiveness studies in real-world settings.16,17 In the current series, two of the three families withdrew from treatment within the CDI phase, which aligns with the higher end of these attrition rate estimates. Both families who ended services prematurely attended sessions sporadically before dropping out, which is also consistent with research suggesting that fewer than four attended sessions early in CDI is associated with little improvement and increased risk for attrition. 18 Furthermore, ratings of child behavior problems slightly increased for each of the two families who ended services prematurely, and parenting behaviors showed minimal change. The lack of improvement for the two treatment non-completers in this study contrasts sharply with expected outcomes of PCIT but is in keeping with the challenges that have been observed in other parent-training programs when working with caregivers who have ADHD. 6 This lack of quick improvement may also have interacted poorly with Mother 1’s symptoms of inattention by not providing sufficient reward for effort, leading to early attrition. Notably, however, Mother 2’s ratings of ADHD symptoms were not elevated, but her treatment outcome was comparable.
Conversely, Mother 3 exhibited excellent attendance and homework completion and completed the CDI phase of PCIT. Of all the participants, she rated her child’s behavior as most problematic at pretreatment. This high level of observed disruptive behavior may have contributed to her increased engagement with treatment compared to the other mothers studied. She also demonstrated more of the Don’t skills at pretreatment than the other mothers studied. It is possible that this discrepancy also served to help her remain more engaged with treatment in that she could see a change in her behavior toward her child quickly. Indeed, she experienced a large decrease in the Don’t skills from pretreatment to week 1. Though ratings of her child’s behavior problems decreased from pretreatment to the end of CDI, they remained higher than average. This is consistent with research literature indicating the necessity of both CDI and PDI to achieve optimal treatment outcomes with children in the clinical range for externalizing behaviors. 19
Conclusion
For preschool-aged children, the United States Centers for Disease Control recommends parent training in behavior management as a first-line treatment before initiating medication, and PCIT has a wealth of evidence in this population.20,21 However, parental ADHD adds complexity to this treatment, and these families may require additional support to be successful. To tailor treatment for these parents, therapists may consider dedicating additional time to problem-solving treatment attendance barriers and scaffolding parents’ planning and organization for homework completion. Significant symptoms may warrant referrals to evidence-based interventions for adult ADHD, which include medication management, cognitive-behavioral therapy, mindfulness, and cognitive remediation. 22
Limitations to the current case series include the limited information about participating mothers’ current mental health status and confirmation of ADHD diagnosis. Future research should examine parental ADHD symptoms as they relate to engagement and outcomes in PCIT and other behavioral parent training programs. If these difficulties create barriers to optimal outcomes on a broad scale, treatment adaptations to support these parents would be warranted.
Footnotes
Authors’ Contributions
Each of the four authors of this publication made substantial contributions to the design, conceptualization, writing, and/or editing of this manuscript, and all gave final approval for the publication of this article in its current form. Each author participated sufficiently in the work to take responsibility for the content of the draft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The University of Florida’s Institutional Review Board for human subjects research approved this study (IRB201800348) on December 15, 2018. Written informed consent was obtained from all three participants. The study was carried out in accordance with the principles enunciated in the Declaration of Helsinki.