
Abstract
People who seek therapy often view the problems they are experiencing as reflections of something internal, which could lead to a sense of helplessness over the problem, ideas of blame, and negative self-worth. Narrative therapy is a respectful, non-blaming approach to therapy that centers people as the experts in their own lives and views problems as separate from people. Externalizing conversations are a facet of narrative therapy that seek to separate individuals from these “internalized” understandings or ideas of a problem, place the problem in the social context, and construct preferred stories that align with their values and skills to re-author problem stories. The problem stories people bring into therapy may often focus on perceived failures, weaknesses, or feeling overwhelmed with the problem. Externalizing conversations can play a role in deconstructing these narratives and therefore challenge the negative perceptions of self and identity associated with the problem.
The stories presented in this article by three narrative practitioners working in the Indian context revolve around their therapeutic work with three young people, with a focus on the use of externalizing conversations to de-pathologize LGBTQIA+ identities, work with experiences of violence and abuse without retraumatization, and deconstruct the diagnosis of ADHD. Here, externalizing conversations serve as a framework to deconstruct ideas of internalized blame, shame, and guilt for young people with different problems, ages, and socio-cultural contexts. Weaving these distinct stories together and reflecting on the use of externalizing conversations in the therapeutic context, this article seeks to explore and discuss dominant ideas about problem stories and therapeutic intervention and create paths to reauthored stories with a focus on individual agency and social justice.
Introduction
We make stories and stories make us. 1 We make sense of this world through stories; they help us make meaning of our lives and world. More than describing our experiences, they also shape our experiences. When people consult therapists, inevitably, a problem story has taken a dominant place in their life. They start measuring their worth through it, which at times ends up isolating them and robbing them of agency of their own life. In narrative practice, therapists take a deconstructive position and do not locate the problem in the person but in the socio-cultural and political context. 2 Psychology and psychiatry have a dark history of pathologizing people’s suffering and encouraging practices that propagate a dominant culture of oppression. As Michael White, co-founder of Narrative Therapy, puts it, “without doubt, the psychologist and psychotherapy play an entirely significant role in the reproduction of the dominant culture.” 3
In narrative therapy, we engage with people by “externalizing” the dominant problem story and inviting their agency to explore richer, preferred counter-stories. It assumes people want to live their life consistent with their values, beliefs, hopes, and commitments. Narrative therapy is a respectful, non-blaming, non-pathologizing approach to working with people that centers people as the experts in their own life. 4 It also believes that people have many skills, competencies, and abilities that will assist them to reduce the influence of problems in their lives and move forward toward their preferred future. 1 Most importantly, narrative therapy is rooted in social justice. It has been informed by cultural anthropology, intersectional feminism, postcolonialism, and queer studies (to name a few influences). Though narrative practice has its origins in the West, it has been adapted to various cultural contexts, including Asia and Africa, with remarkable innovation. It provides a vocabulary, politics, and vantage point to invite transformative conversations in therapy space and the community.
It is based on the principle that a person is not the problem; the problem is the problem, and the problem is mostly social. 5 It works at deconstructing and addressing how different levels of discrimination such as gender, sexuality, neurodivergence, race, religion, and caste intersect, multiplying to cause marginalization and problems in people’s lives. 6
Externalizing conversations or practices are used in response to the “problem stories” that people share in therapeutic spaces. As mentioned above, by the time people may reach out to therapists, the problem they are facing has become a “dominant narrative” in their life and has often become internalized. People begin to see themselves as the problem, which can often be seen in statements such as “I am depressed,” “Why am I like this?” “I am just an anxious person,” and so on. Externalizing the problems that have become internalized in people’s lives plays an important role in taking the deconstructive “person is not the problem” approach, as described above. This can be achieved in different ways, including asking questions in which we personify a problem, intentionally asking questions, or framing our responses in order to change the adjectives people use to describe themselves, 7 for example, responding to “I couldn’t do anything today because I’m depressed” with “What else does the depression make you think about yourself?” or “What does the depression stop you from doing that you would like to do?”
In this article, three narrative practitioners from our organization, Children First, present stories of practice that visibilize externalizing practices and politicize the acts of social injustice, turning the gaze back on normative judgment and acknowledging acts of resistance, care, protests to invite personal agency, and rich counter-stories. 8 Informed consent has been secured from all participants prior to their involvement in this research study.
Externalizing Conversations as a Way to Work Toward De-pathologizing LGBTQIA+ Identities and Exploring Alternative Stories
Arsh (14 years old) came into therapy with experiences of anger, isolation, and self-harm. They had recently come out as bisexual to their family and friends, who Arsh did not see as very supportive toward them. Hearing “this is just a phase” repeatedly and losing friendships had led to a great deal of anger and hurt for them. While discussing the anger, Arsh recognized that feelings of isolation and loneliness would often arise when thinking about their sexuality and the responses to “coming out” they had experienced. They often asked questions like, “Why do straight people get to understand each other when I have no one who understands me?” Arsh also shared that they had begun questioning their gender identity around this time.
Through their process of questioning their gender, they settled on they/them pronouns and the label “genderqueer.” On one hand, they spoke of this label and these pronouns as “feeling right.” On the other hand, there was a persistent question of “I don’t know how gender is supposed to feel, so how do I know that I’m not cis?” They spoke of feeling dysphoric but not being sure about it and asked, “What is my gender, how does it function? And how do I tell what it is?” To explore that question, we spoke about the word “gender dysphoria.” This became a point for Arsh to begin reflecting on their experiences with their gender identity, including understanding dysphoria and its effects on their life. The dysphoria would often try to convince them that “if I did things that normal straight kids do, I would be normal too and not anxious all the time” or “if this disappeared, my problems would disappear, but this is a part of my identity and I don’t know if I want it to disappear.” Parallelly, we also spoke of preferred narratives, particularly gender “euphoria” and “belonging,” 9 as things Arsh would like to experience in the future.
Externalizing Dysphoria: Statement of Position Map 1
Using externalizing conversations through Statement of Position Map 1, we worked on externalizing dysphoria for Arsh. White and Morgan 10 describe this “map” as a useful way to “unpack externalising practices in teaching contexts, and to describe the preliminary steps in the sort of rich story development that is founded upon ‘unique outcomes’ or ‘exceptions.’” In narrative practices, maps have been referred to as “constructions that can be referred to for guidance on our journeys with the people who consult us about the predicaments and problems of their lives.” 4 This journey of exploration begins by exploring the “character” of the problem through questions around how the person would name and describe it, followed by questions exploring the effects of the problem on the person’s life. Questions around the position they take on it and what is important to the person that is impacted by the problem then seek to invite agency into the dominant narrative around the problem story. Table 1 is a visual representation of Arsh’s statement of position map for dysphoria, characterized by them as “Gloop the Gender Dysphoria Cat.” This map uses “experience-near” language—the language that Arsh uses themselves to describe the problem, without interpreting it in any way.
Externalizing Map of Gender Dysphoria, with Categories of Inquiry 1–4 from the Bottom to the Top.
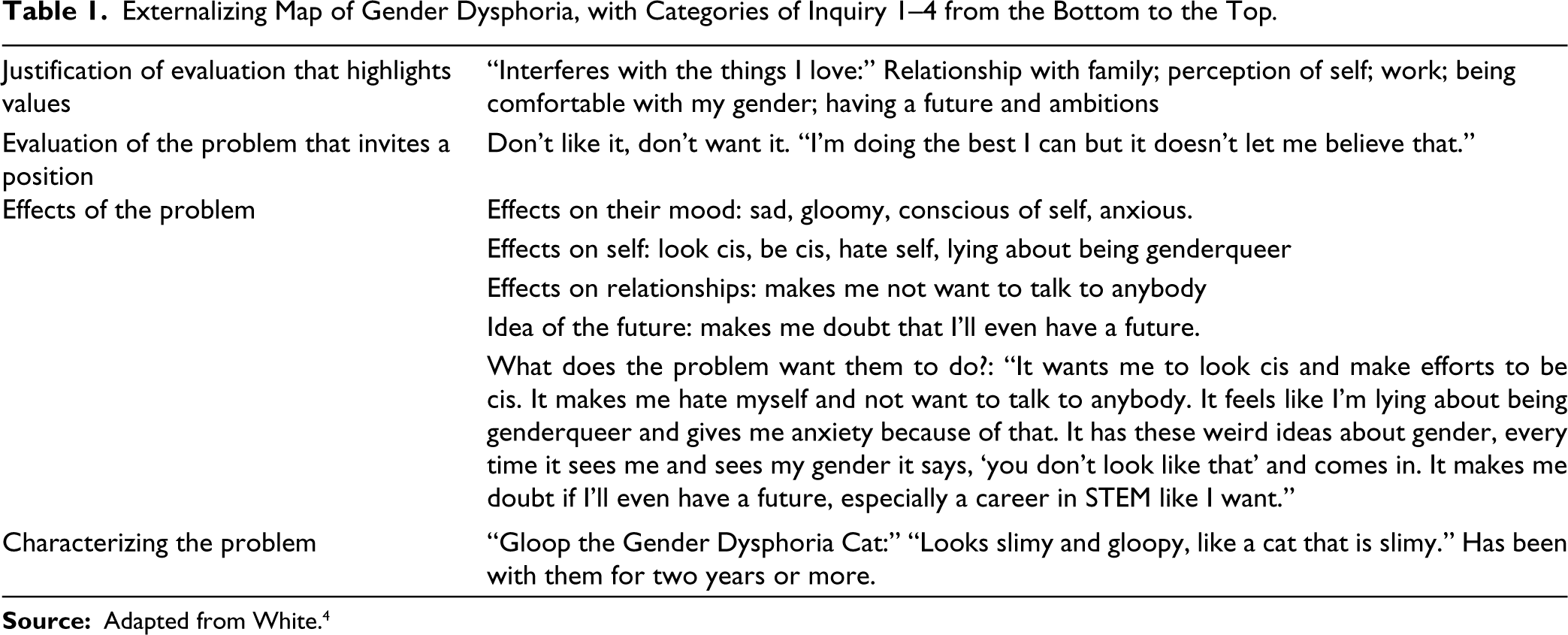
Exploring the impacts of Gloop on Arsh’s life through this lens, using language like “How has Gloop been affecting your mood?” helped look at the dysphoria as separate from Arsh. Arsh began to look at things that were not affected by Gloop or that they were able to achieve in spite of Gloop’s impact on their life. This included becoming a class representative, working hard even when dysphoria would not let them, and being able to experience and recognize moments of gender euphoria. Over time, Arsh cut their hair, started wearing clothes that they felt were more in line with their gender identity, and started playing as a man in the video games they enjoyed. In the face of dysphoria so intense that it would often bring back the self-harm thoughts they had initially struggled with, these were moments that felt genuinely like euphoria to them. Arsh also explored the idea that while gender dysphoria was not something they wanted in their life and euphoria was much preferred, both things could exist simultaneously. Rather than viewing them as antidotes to each other or seeing if euphoric experiences would “cancel out” dysphoric ones, Arsh would speak of both as coexisting. With euphoria being named and picked up on more frequently, they felt able to focus more on the things that they valued and felt were important.
Why Were Externalizing Conversations Used?
Language that is taught to mental health professionals can be pathologizing and even harmful toward LGBTQIA+ individuals,11, 12 including the strong focus on ideas of dysphoria and suffering that are centered when talking about LGBTQIA+ mental health. LGBTQIA+ clients who access therapy can often feel the need to share a certain image of the “ideal” LGBTQIA+ person and highlight only very specific issues to receive the care they need. Using externalizing conversations to take a position on dysphoria as well as introduce the idea of experiencing gender euphoria and belonging was something that helped Arsh explore their gender identity in an “experience-near” way and challenge pathologizing discourses on gender dysphoria.
Using Externalization to Work with Experiences of Violence and Abuse: Re-authoring Narratives Without Re-traumatization
While growing up, Sunaina (20 years old) was close to a cousin who was a warm and supportive figure in her life. After an incident of sexual assault perpetrated by this cousin, Sunaina was left distraught with nobody to share the ordeal with. She courageously tried to share her experience with her mother; however, she was told not to talk about it, for it would bring dishonor to their family. This invited a lot of “blame” and “doubt” that Sunaina started to carry with herself, which presented itself in the form of anxiety and trauma, for which she decided to seek therapy.
Through externalization, Sunaina started perceiving the lies that blame and doubt told her and collectively named them “Pinocchio,” for they often lied to her. The name itself strengthened her efforts to distinguish between her voice and that of blame and doubt (Pinocchio). She started addressing the many lies and tricks of Pinocchio, such as blaming her for the abuse and making her believe that she is alone and is undeserving of romantic relationships. She did not have to recall each and every detail surrounding the abusive event, yet she attributed the effects to the problem rather than herself.
Therapist: How does Pinocchio make you “doubt” yourself?
Sunaina: It makes me think that since I didn’t stop the abuse, I let it go on.
Therapist: The idea that you let it go on because you didn’t stop it, is that your voice or Pinocchio’s?
Sunaina: Pinocchio’s
Therapist: Where did Pinocchio pick up such an idea?
Sunaina: I didn’t fully understand the difference between sex and sexual assault. Just because I didn’t stop, it doubts that it was an assault.
Why Were Externalizing Conversations Used?
Traumatic experiences such as abuse can be painful to revisit and potentially re-traumatizing. Narrative therapy attempts to identify alternative ways to engage in traumatic conversations that address the effects of the problem as well as focuses on how individuals reclaim themselves from its effects simultaneously. When young people come in, their understanding of how they are dealing with the effects of abuse is often thinly layered. Using externalizing language that separates the person from the problem, and places the problem in its social context, helped to not increase the blame for what Sunaina is already experiencing and also encouraged collaboration to identify what she is doing to reduce the effects of the problem. 9 David Denborough’s work in creating frameworks of inquiry and documentation for trauma experiences 13 and Angel Yuen’s work in challenging discourses of “victimhood” in work with young people who have faced trauma 14 have influenced efforts to prevent the possibility of re-traumatization, particularly in terms of facilitating questions with care and in responding to their stories.
The effects of externalization can unfold in a dynamic manner. While unpacking the blame and doubt, Sunaina also traced its history back to a particular belief:
In films, often perpetrators are strangers or they show women who have been abused would have strength or resources to talk about their experiences. I lacked both of these scenarios. If people would have heard me, I would have accepted what happened. It is like my voice has been taken away.
Sunaina called it the idea of a “perfect victim” that took away her voice to recognize it as abuse and instead placed the “blame” on her for the act. Since the perpetrator was known to her and she had not attempted to stop the abuse, Sunaina considered herself an “active participant” in the abuse. Along with this, the cultural idea of abuse bringing family dishonor also invited blame. Through these larger conversations that externalization enabled, Sunaina could place the problem in a socio-cultural context without going into the details of the event or identifying with the cause of it. The distinction that externalization provided further opened up what Sunaina prefers for herself as opposed to blame and doubt, preparing a landscape for re-authoring that Sunaina is actively responding to reduce the effects of the problem.
I went for public stories of other women, where she was shocked too, or was not able to comprehend what was happening to her. This sometimes helps me to counter my “doubt.” I try to tell myself, “I am not alone in this.”
Therapist: “How come you decided on this action rather than something else?”
Sunaina: “I thought if it was the documentaries and people which implied it was my fault, I could take to the same material like videos and books that talked about it differently. I have stopped hurting myself and I want to continue to not. I want to understand the younger Sunaina. One has to be continuously in search of people and space that is comfortable.”
Therapist: “You would like to understand the younger Sunaina? Is this important to you?”
Sunaina: “Ya, I don’t want to feel alone like I had said before.”
Therapist: “Does this say something about how you are negotiating with Pinocchio?”
Sunaina: “Maybe that I don’t want to be defined by my past ?”
Here, Sunaina could be seen attempting to connect with experiences of other women who responded similarly to the abuse as she did and even attempted to engage with information and resources that challenged the idea of being a “perfect victim.” This was one of the dominant ideas that internalized blame and doubt, and her efforts can be viewed as acts of resisting these ideas. “Just Girls” 8 is one such collective through which there is an attempt to collectivize experience, insider knowledge, and skills of living for young women negotiating with the unique problems they face. Through her work with young women who have experienced trauma and gender-based violence, particularly in the Indian setting, Sen 8 emphasizes how collectivizing wisdom could create opportunities to identify and resonate with alternative stories that give power over the problem. Sunaina, through her act of collectivizing, could once again be perceived as actively responding to reduce the presence of “blame” and “doubt” in her life.
Using Externalization to Look Beyond Horizons of “Inattention:” Deconstructing the Diagnosis of ADHD in Young Adults
ADHD has often made me feel like the smartest and the dumbest person at the same time.
This was one of the first descriptions of ADHD shared by SK when we began therapeutic work in 2020. SK (25 years old) was consulting with us to understand her recent diagnosis of ADHD, which in her words “was a light bulb moment and felt like a hammer hit the nail.” Growing up, SK shared that
The traditional ways of being and learning are very rooted in my life … always made me question “Aise kaun focus nahi kar sakta” (how can one not pay attention?), “main effort nahi daal rahi hungi pakka” (I must not be making an effort); “Potential hai but pahunchana kaise hai?” (I have the potential but how does one reach it?).
These questions started to become stronger as the demands of work increased in higher grades, while struggles with “inattention” remained camouflaged behind socio-emotional struggles. This was partly a result of environmental experiences, including the focus on performance and a one-size-fits-all approach to curriculum and assessment usually seen in the Indian academic context. The effect of undiagnosed ADHD posing questions on SK’s abilities was also reflected here.
This section hopes to highlight the nuances within the neuroscience of neurodiversity, laying focus on stereotypes that influence symptomatology, the impact of a late/adult diagnosis of a neurodevelopmental disorder, and the use of narrative practices in making meaning of an ADHD diagnosis through an intersectional lens. Describing ADHD as an “invisible barrier…it felt like running a track and feeling like running at one spot without moving forward,” she shared how her journey began while researching about ADHD after her brother received a diagnosis and being taken by surprise at the resonance she experienced.
While the externalization began with exploring the effects of “the invisible barrier” (ADHD), it was observed that it was actually the “experience of ADHD” that came forward. This led to an introduction to anxiety, guilt, and procrastination as prominent “characters” that responded to this “barrier” and shared a close relationship with SK. We further attempted to map the long-standing effects of their respective roles in either aiding or limiting the experience with ADHD:
Therapist: “Would you say anxiety and guilt present themselves together? What is their relationship like?” SK: “I think guilt is constant vs. anxiety is free floating” Therapist: “What would their relationship be like with a task at hand?” SK: “Guilt sometimes has been an enabler, especially during a deadline, but has been a hindrance in the backseat, more than a driver.”
15
Therapist: “How has that experience been for you?” SK: “‘It’s like having a CNG cylinder when my car runs on petrol’—‘I’ll keep it to pacify me’, guilt would say ‘It’s better for the environment’ … playing the devil’s advocate constantly.” Therapist: “You used the term ‘devil’s advocate’ for guilt, did the devil’s advocate have a voice or make you believe in certain things?” SK: “I think it led to an internalizing voice which sometimes were ‘lazy’, ‘stupid’, ‘I don’t know this’ … could not trust my own intelligence which led to background anxiety.” She added that “I felt I managed my anxiety so well that I internalized it. When my ADHD started receiving intervention, the awareness around anxiety increased and it latched on to ADHD.” Therapist: “Did this experience get in the way of things you valued?” SK: “I think I never displayed what I loved, didn’t have the energy to fight critics. Maine kuch karra hi nahi (I didn’t do anything) …to protect myself from the daant (scolding) …The voice I found in college helped in talking to oneself, developing a new vocabulary and starting my mental health journey….” Therapist: “How would you define your relationship with them at the present? How do you feel about their presence in your life—okay/good/bad?” SK: “They are treasures of my mind now, Want to maintain a relationship with them but set some health boundaries now that we are all adults.” Therapist: “You mentioned that ‘I found my voice in college’, what helped discover this voice and how was this important to you?” SK: “College was a space to reclaim confidence. ‘I found my voice’—have friends who share interests like me, creating a space for acceptance, I fully went on the journey of finding my voice after college where I actually spoke up—this was a very coming of age kinda thing.”
This almost gave a glimpse into parts of her “club of life,” memberships and spaces that have been important in her journey. 3
In a subsequent session where we revisited this conversation, she shared a visual of procrastination as follows:
SK: “Procrastination is like a bad crazy friend who shouts ‘boring’ the whole day and doesn’t shout when am not doing anything. Mocking me ‘ye toe sab karlete hai’ (everyone can do this). I feel procrastination was also raised with discipline and structure and now its adult version is being a boring rebel.”
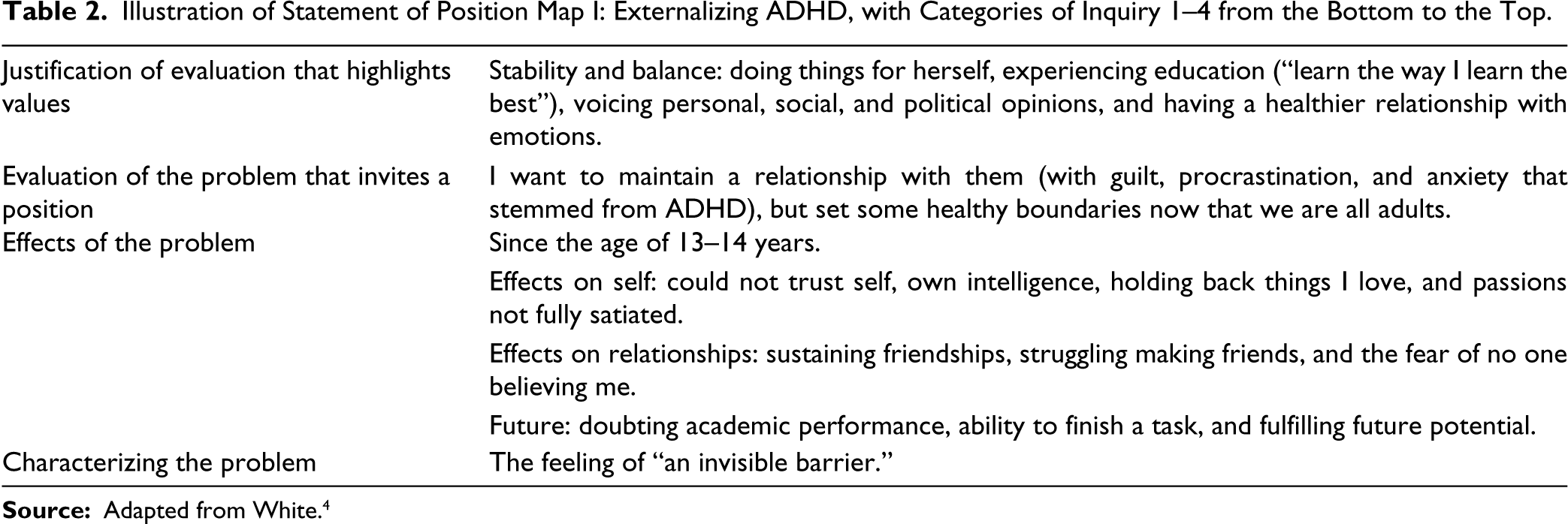
Over the next few sessions, different sections of our conversation, along with a document of summaries after each session, led us to move along the Statement of Position Map 1 on Externalizing Conversations (Table 2). 4
Illustration of Statement of Position Map I: Externalizing ADHD, with Categories of Inquiry 1–4 from the Bottom to the Top.
Why Were Externalizing Conversations Used?
We further explored these experiences within the wider ecosystem of SK’s journey. Creating a distance between the person and the problem is often a challenge when a diagnosis is deeply embedded in neurobiology and understood through the disability model that places “the problem” internally. Often, these discourses emerge from societal norms and institutional barriers, which may perceive a “difference as a deficit.” According to David Nylund, 16 “Naming the problem brings ADHD closer to experience” and engaging in “creative dialogues makes it easier to have some control over it.” When she shared that “A major learning during covid was customizing things my own way. … Finding a difference between How I need to live vs. how it is supposed to be lived,” it highlighted an opportunity where she was able to identify and resist dominant discourses (of learning, communicating, performing, etc.) and move toward strengthening her preferred story.
Discussion
When a problem gets externalized, it enables us to identify the dominant and powerful ideas, beliefs, and practices that sustain the problem, an approach that narrative therapy in a post-structuralist understanding is able to facilitate. Freedman and Combs
2
shared,
We believe it is our responsibility as therapists to cultivate a growing awareness of the dominant (and potentially dominating) stories in our society and to develop ways of collaboratively examining the effects of those stories when we sense them at work in the lives and relationships of the people who consult with us.
How does this effectively play out in work with individuals, especially as narrative practitioners in the Indian setting?
When externalization helps to trace the history of a problem, there is scope to encounter a multitude of social factors in the Indian context, such as caste, class, families, religion, politics, education, etc. It is important to listen to the effects of the problem keeping in mind these intersections. This helps in understanding the dominant social discourses unique to the survivor’s experiences, reiterating that “the person is not the problem, the problem is the problem, and the problem is social.” This gets overlooked in a society rooted in placing the problem within the individual, thus giving rise to many emotions of shame, guilt, doubt, and blame, as it did for Sunaina. Hare-Mustin 17 had beautifully highlighted the potential of the therapy room in either serving to maintain the oppressive dominant discourses that sustain the problems or in questioning and uprooting them.
The therapy room is like a room lined with mirrors. It reflects back only what is voiced within it. When there is a one way mirror and reflecting team, they too reflect back what is being provided. If the therapist and family are unaware of the marginalized discourses, such as those associated with members of the subordinate gender, race and class groups, those discourses remain outside the mirrored room.
Sunaina identified the role of “patriarchal narratives” in the lack of support she received from friends and families: “patriarchy doesn’t allow stories of women to be told verbally or in writing.” This made it difficult for Sunaina to rely on her own judgments. However, through tracing the history of the problem to these narratives, she was able to reduce the internalization of blame. Sunaina’s mother comes from a background where she has had less access to education and resources to understand sexual abuse. Similarly, notions held by male peers, the cousin who perpetrated the abuse, and her father, who often took an unheeding position, were all located in the system of patriarchy, particularly as it plays out uniquely in the Indian context and reinforces oppressive narratives. These were necessary threads to address as we continued to unpack the problem stories.
Stories and language have also historically played a very important role in the lives of queer, trans, and gender diverse individuals as a tool of both oppression and reclamation. Tilsen and Nylund 18 have spoken of “queering” as a point of resistance to fixed identities and normativity, rather than just a descriptor of one’s sexuality, while Reynolds 19 describes queer theory as inviting “fluidity, movement from the fixed and certain to the confused and unstable.” Queering therapeutic spaces through our use of language can then be seen to be a form of “imperfect allyship.” 19 In the therapeutic space, taking a step back from our decentered and influential position—such as to share information about our therapeutic practices—can be seen as a way of subverting dominant Western psychological discourses. 20
For Arsh, who had visited other therapists before, a lack of knowledge and awareness in these spaces was also noted to be as impactful on anger and dysphoria as acts of hatred or ignorance. They spoke about the importance of things like therapists introducing themselves with their pronouns, a relatively uncommon practice in the Indian context, sharing that they felt able to begin to explore dysphoria and its effects in conversations through observing this act. Similarly, when therapeutic conversations move away from the “known” of suffering in the lives of LGBTQIA+ individuals to exploring the relative “unknown” of gender belonging or euphoria, it can also be seen as a subversion of dominant discourses about therapy with LGBTQIA+ individuals. In that vein, a part of our work while “queering” therapeutic spaces may necessitate us to take a brief step back to take up positions of allyship in therapeutic spaces with queer people. This might include navigating conversations with the families of young people in the face of backlash, 19 exploring gender-neutral or gender-euphoric pronouns in different Indian languages, sharing our own pronouns as a form of practice, asking influential questions to illuminate alternative stories, introducing terms like “trans-talented” 9 if deemed appropriate, and sharing resources or documentation, letter exchanges, and outsider witness conversations with other queer and trans individuals.
Through our training and education, we have been taught to rely on knowledge and empirical practices. “Every act of declared knowledge is an act of oppression against someone.” 21 Having its roots in neurobiology, the diagnosis of ADHD often carries various systemic voices of assumptions (about its presentation, expression, experience, as well as intervention), posing a risk of “declared knowledge” carried among mental health professionals as well. David Denborough states that “with a focus on changes in the brain, there is a risk that studies could inadvertently conceal more than reveal,” 22 strengthening the narrative of the internalization of ADHD. The concept of “neuro-conceal” elaborates on the neuro-scientific understanding of disorders that promote a limited field of vision for a problem by minimizing the impact that social, cultural, and political identities have on the problem. According to Beaudoin and Zimmerman, 15 narrative conversations can provide an opportunity to create shifts in the affective experiences of a memory. Over the course of time, SK shared that “Things that were seen as character flaws have been described by ADHD—It felt like unwrapping a gift versus hiding trash. I set myself up for things which weren’t made for me, I feel free of those shambles now,” honoring her experience of the past and of the future. It is also critical to note that externalization helped to stay close to not just SK’s unique experience but also the distinct language she uses to make meaning of her experience, such as the use of the word “daant” (scolding). Externalization made it possible to unpack the problem in an “experience-near” manner close to its vernacular roots, facilitating further space for SK to exercise agency.
As therapists, the pathway that can be built through insider knowledge 23 helps in “leaning in,” described by Reynolds 24 as a process of inviting collaborative accountability rather than individual responsibility in the therapy room. Accountability toward our work then lies not only in furthering our own education but also in continued forms of learning and unlearning (widening our understanding of symptomatology, of presentation based on age and gender, and holding sensitivity to social/cultural/economic identities). It also includes intentionally moving away from the harm of singularity or a single story 21 and toward building narratives through an intersectional, post-structuralist, and social constructionist lens.
We are “cultural receivers of stories of suffering” (Waldegrave et al 5 ). While engaging with these stories, holding on to the possibility that healing goes beyond the individual to create ripples can take therapy outside the confines of the “mirrored room” 17 and work toward addressing larger issues of social justice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed assent and consent were obtained from the patients and/or their parents respectively whose case material has been discussed in this paper.