
Abstract
Family therapy is often indicated in the treatment of adolescents with mental health difficulties. The family context is often seen as a predisposing, precipitating, perpetuating, or a protective factor for a wide range of child and adolescent mental health concerns. Several approaches to family therapy are now recognized as evidence-based treatments for different psychiatric presentations. In this article, we hope to describe the relevance of family therapy for families with adolescents in India, present case illustrations on commonly used approaches to family therapy, and propose clinical practice guidelines.
Introduction
Families caring for adolescent children with mental health vulnerabilities are perhaps most receptive to all types of treatments offered. Family therapy is one of the major treatments they are referred to, globally, and there is robust evidence of its effectiveness in reducing relapse rates, admission duration, and overall positive outcomes for presenting problems. 1 Literature shows several specific family therapy models for specific problems (substance use, delinquency issues, 2 and suicidal attempts 3 ) in adolescents with good research evidence for their usefulness.
A recent review 4 of the current evidence base including meta-analyses and systematic reviews suggest, that for various child-focused problems including sleep, feeding, and attachment problems in infancy; conduct problems; recovery from child abuse and neglect; somatic problems; eating disorders; and first episode of psychosis, family therapy offered independently or in conjunction with other modes of therapy is effective. Apart from those, a trans-diagnostic view of several presenting problems of adolescents encourages the use of family therapy in a wide range of situations with adolescents. In India, while parents are often involved in treatments, systemic family therapy principles are underutilized for this population. This article covers some of the relevant aspects of family therapy through case illustrations and clinical practice guidelines for further growth of this field in India.
Family therapy involves all immediate family members in addition to the “identified patient” and addresses interactions and relationship dynamics (such as communication, cohesiveness, flexibility, and so on). The aim is often to treat relational distress and improve family health and functioning. 5 Psychiatric symptoms are understood as resulting from a bidirectional influence between the individual and the interpersonal family environment. In family system theory, 6 a family is considered to function as a unit embedded in and reciprocally interacting with other units in the society. Members constantly interact with each other to maintain a healthy system. Problems in interactions can predispose, precipitate, and/or maintain psychiatric symptoms. Hence, improving family functioning also impacts family members’ health and functioning, which in turn can lead to positive changes in the family going forward. 7 Family members were first included in psychotherapy in the early 1890s when children in child guidance clinics commonly presented with problems linked to their family context. 8 Over the years, family therapy has evolved as a key evidence-based treatment of choice for many child- and adolescent-focused problems. 4
There are various schools of family therapy that differ in the importance they give to specific aspects of family dynamics and their target for intervention. Structural family therapy, 9 for instance, emphasizes hierarchy, boundaries, and roles in the family, whereas strategic family therapy 7 places importance on the symptoms’ functionality, communication, and cybernetics, which refer to feedback loops in interaction among members and often play a role in maintaining problems in the family. Additionally, Bowenian family therapy believes in working to reduce emotional reactivity and triangulation among members and increase healthy differentiation of self.
Meanwhile, psychodynamic and object relation approach to family therapy aims to develop a more conscious understanding of experiences among family members such that unresolved intra-psychic conflicts, unhelpful internal representations and projective processes can be addressed and expressed adaptively interpersonally. 10 A related perspective is that of attachment, which focuses on the emotional aspects of interpersonal relations. Cognitive-behavioral family therapy focuses on beliefs and behavioral exchanges among members. 11
The Satir model of family therapy, on the other hand, is a process-oriented approach that draws from humanistic assumptions and stresses on the therapist making emotionally authentic contact with the family. An experiential attempt to make sense of and change dysfunctional family patterns is made with the use of metaphor, drama, and the “self of the therapist.” 12
Families progress through different stages marked by predictable life events and transitions such as marriage, parenthood, launching children out, etc. 13 Like developmental tasks, there are certain stage-specific tasks that families are confronted with, and their ability to withstand the changes and effectively perform the tasks are a measure of its functioning. Some of the tasks that families with adolescents must work on are creating a shift in the parent–child relationship with a balance of granting freedom and holding adolescents accountable for their responsibilities. Parents may also need to address mid-life issues that can crop up in their marriage, career, as well as in their families of origin such as ailing parents. This forms the backdrop of the identity formation and separation-individuation challenges14,15 for the adolescent. With separations, divorces, blended families, families with adopted children, or other changes in the family structure, systemic and intra-psychic interplay can often trigger behavioral difficulties in the adolescent. 16
Families that are struggling with the tasks of adolescence can present with concerns such as separation anxiety, parental roles being taken on by the adolescent (“parentified” child), and the adolescent yielding disproportionate power in the family system. 17 Family therapy has been found to be a powerful process through which healthy development can be facilitated in such cases. Additionally, it is also indicated when families seek help for stressors related to atypical or non-normative family arrangements, such as identity issues related to adoption and ethnicity 18 and strengthening bond with a parent in single-parent families. 19
Certain forms of family therapy have been studied in relation to specific mental health conditions. Table 1 provides an overview of the different types of family therapy and some of the conditions that research suggests it is indicated for. For treating internalizing and externalizing mental health conditions among adolescents, structural-strategic family therapy has been found to be useful and was also found to improve family cohesion and healthier parenting. 20
Summary of Types of Family Therapy.
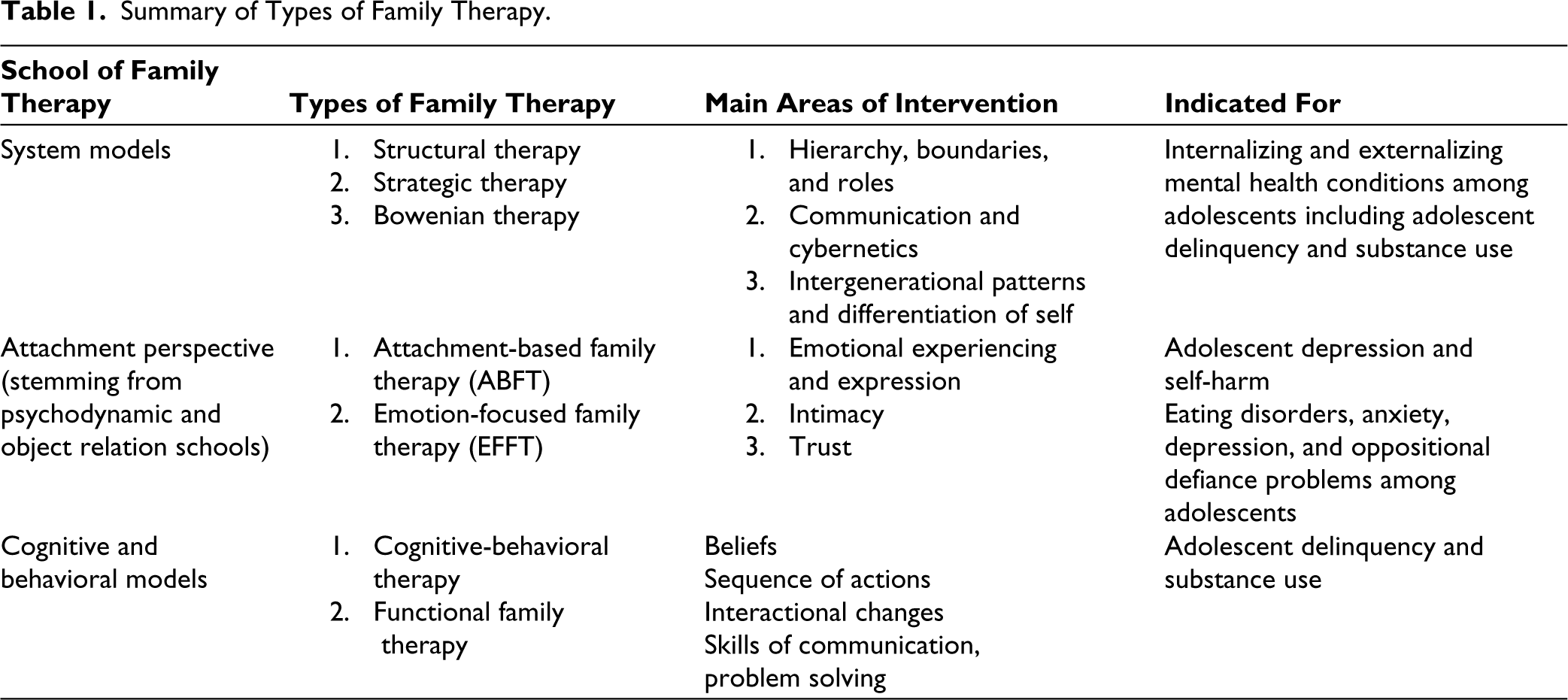
Diamond et al.’s 21 attachment-based family therapy (ABFT) is efficacious in treating adolescent depression and self-harm. 22 The focus is on repairing ruptures in the adolescent–parent attachment or facilitating re-attachment. This is done by supporting the members to access their emotions and desire for greater intimacy and engage in respectful dialogue about past concerns and present conflicts, which serves to rebuild a sense of trust and closeness. The adolescent is then encouraged to pursue developmentally appropriate endeavors, and the parents are empowered to act as the secure base and provide encouragement and support.
Emotion-focused family therapy (EFFT), which aims to bring in change by increasing parental self-efficacy and removing emotional blocks such as fear of incompetence, self-blame, etc. so that parents can play a positive role in the recovery process of adolescents, is also a research-backed intervention for eating disorders. 23 It has also been found to be helpful in supporting families with anxiety, depression, and oppositional-defiance problems. 24 After a two-day EFFT intervention for caregivers and parents of children with mental health difficulties, participants reported feeling more hopeful, having fewer negative emotions, and feeling more confident to try new behaviors to support their child. 24
Other conditions wherein family therapy has been shown to be effective are bipolar disorder (adjunct to pharmacological therapy), anxiety disorders, and psychosis, where psycho-educational family therapy is widely used. 22 A lot of work has also been done on family therapy for eating disorders among adolescents, 25 with evidence for better status at follow-up compared to individual interventions. 26 A meta-analysis 2 on adolescent delinquency and substance abuse shows that the four family therapies (brief strategic family therapy, functional family therapy, multidimensional family therapy, and multisystemic therapy) have statistically significant but modest effect on outcome compared to treatment-as-usual and other treatments but were not found to be relatively different from each other.
Hogue 27 examined manualized family therapies for 11- to 14-year-olds with conduct and substance use issues. They analyzed 196 cases and 302 sessions of multidimensional family therapy, brief strategic family therapy, and functional family therapy with the aim to find flexible and trans-diagnostic core elements of family therapy. Factor analysis showed four categories comprising 21 techniques (interactional change: six treatment techniques; relational reframe: seven techniques; adolescent engagement: four techniques, and relational emphasis: four techniques). Interactional change refers to therapists assessing family dynamics, guiding in-session interactions, helping communicate meaningfully, and improving relational skills. Relational reframe is about therapists’ efforts to help them view problems in relational terms rather than adolescent-focused clinical terms and to seek relational change as the primary clinical solution. Adolescent engagement are interventions in which therapists seek the adolescent’s unique perspectives and motivate on personal goals connected with family as well as the outside world. Relational emphasis is about focusing on the family, assessing systemic attributions, and improving overall family functioning.
While manualized family therapies have a lot of strength and are indispensable in research and training contexts where structure and uniformity are crucial, implementation is rarely possible in routine clinical care due to costs and difficulty in availing specialized therapists, along with considerable heterogeneity in the demographics and needs of client population, which warrant customized and integrated care. Additionally, specific discussion on creating and maintaining therapeutic alliance is missing in literature despite evidence that alliance plays a significant role in family therapy outcomes. 28 This article aims to synthesize the fundamentals and key principles of practicing family therapy with adolescents based on research evidence and clinical experience. Two cases from the Family Therapy Unit at the National Institute of Mental Health and Neurosciences (NIMHANS), a tertiary mental healthcare center in urban Bangalore, will be discussed to illustrate the concepts and intervention strategies commonly used. The cases and guidelines are also illustrative of the kinds of integration and blending of techniques that are often required for this population.
Case Illustrations
Case Illustration 1
Mr. N, a 15-year-old student of the 10th grade, from an upper socioeconomic background, and younger of two siblings, presented with reassurance-seeking behavior and repetitive washing of hands for a duration of three years and school refusal, stubborn and demanding behavior, mood fluctuations, and anger outbursts for a duration of six months. The onset was insidious, and course was progressive. Significant family history of suicide in grandfather and cousin was present. The boy experienced chronic bullying in school; it began in the fifth grade regarding his skin color and short stature. He had no friends at school. He, however, continued to study in the same school, though he had repeatedly asked his parents to change his school, and when that did not happen, he stopped attending classes. His diagnosis was obsessive compulsive disorder and adjustment disorder-depressive type, and he was hospitalized for treatment.
Family Assessment
The father’s family was from a lower socioeconomic status, and thus faced financial difficulties, and the parents had marital discord, along with heavy drinking and anger issues in the grandfather and an authoritarian parenting style. The paternal grandfather died by suicide (impulsive hanging following a quarrel with his wife). The father worked alongside his studies. The mother was from a financially secure family, was the youngest of four children, and was overprotected. The maternal grandfather died due to liver failure when she was 18 years old. The couple knew each other since high school and had a secret relationship as they feared resistance from their families due to differences in socioeconomic backgrounds. They got married when he was 21 and she was 19 and kept it a secret. They continued to live with their family of origin until their families accepted their relationship. In subsequent years, differences cropped up between them. The father lost his job, and the mother was treated for depression when the first son was born after three years. Things improved when the second son was born. However, the father was stressed due to job insecurity and had issues with anger, resulting in frequent fights making the home atmosphere tense. The father was a strict disciplinarian, and the children were closer to the mother. The eldest son was more independent but would complain that the younger son was getting all the attention from parents. The younger son was anxious and more dependent and clinging to parents. He was also more emotional and required a lot more support from parents to manage his academic and personal goals.
Systemic Hypotheses
Anger issues of the father and paternal grandfather can be seen from an intergenerational lens. Domestic violence was present in the father’s family of origin. Parents’ interpersonal issues, particularly anger of the father toward the mother, created a chaotic and fearful home environment with a high noise level that disregarded the child’s needs. This resulted in the family facing difficulties with their teenager and in launching the young adult. Autocratic decision-making by the father also conflicted with the adolescent’s need for independence and individuation. The younger boy’s temperament, being bullied in school, and the family dynamics made him more vulnerable to psychopathology. His demanding behavior and anger outbursts resulted from neglected needs and invalidation of his emotions by his parents, as seen in their refusal to change schools despite his bullying experiences. The intergenerational pattern that he learnt from his father’s side was also an important aspect. The conflict between parents and the parent–child subsystem caused the symptoms in the child.
Therapy
Fourteen sessions of behavioral family therapy drawing elements from structural family therapy and intergenerational family therapy were conducted with good outcomes for symptoms and family relationships.
The short-term goals were to: (a) strengthen the therapeutic alliance, particularly with the father, to be able to engage him in therapy, (b) improve their listening skills and encourage them to wait for their turn to respond rather than react and reduce blaming and high noise levels in the conjoint sessions, (c) help them have a longitudinal understanding of the various factors that had contributed to their difficulties and also maintaining them, (d) facilitate consensus and discussion on couple goals and parenting goals for the younger son, and (e) handling individuation with healthy connectedness for the elder son. The father also needed a few individual sessions to learn to manage his anger and regulate his emotions better. This happened concurrently with conjoint family sessions. A long-term goal that was discussed with the couple was also to work deeply to enhance the emotional connection between them and improve greater cohesion as a family.
Case Illustration 2
Mr. V, 17-year-old male in the 12th grade but not attending school currently, from a low socioeconomic background presented to the hospital after a suicide attempt following a fight with his father. The chief complaints at the time were a feeling of heaviness in his chest, present for one and half years, and pervasive low mood, lack of energy, irritability, anhedonia, and suicidal ideation for four months. He had a history of psychogenic coughing, which improved after psychotherapy. He had a slow-to-warm-up temperament and was on medication for asthma. There was a family history of psychiatric illness with multiple second- and third-degree relatives with psychiatric disorders. He is the only child born from a non-consanguineous marriage, and he has an emotionally close relationship with his mother and a distant relationship with his father. The father was punitive and the mother permissive in their parenting styles. Both had high expectations from the son. His diagnosis was severe depression, and he was admitted for treatment. He showed increased irritability primarily toward his father, and toward the mother when she was perceived to take the father’s side. He also had frequent anger outbursts at home and in the hospital, which the parents had trouble managing.
The boy was initially not inclined to family sessions as he reported feeling very angry at the father and said that he had no problems; it was the father who should be treated.
Formulation
After a detailed assessment of the family dynamics, the case was formulated using structural family therapy concepts. 9
The hierarchical structure of the family was not found to be optimal. A clear hierarchy is said to be one “where there are consistent rules about who is in charge of what.” 29 (p236) In this family, the ideal hierarchical structure would involve the parents’ subsystem having greater authority to make rules than the child. However, in the present context, the child seems to have more power, where because of his anger outburst, he can supersede the rules set in place by the parents. At the same time, the father through his expression of anger tries to gain back the power. Moreover, the mother seems to be taking a passive stance in the family, with the hierarchical distribution being in flux constantly, shifting from the father to the child and vice versa, leading to a disorganized structure.
The functioning of the subsystems was found to be inadequate at the time of assessment with concerns over boundaries. Parents were unable to create an effective boundary; a hypothesis about the same can be made based on the current functioning of the system. The couple was disengaged with each other, and the communication was need-based, with most of the conversations happening in the context of the child and not about each other. The parental subsystem comes into the picture in families when the couple has a child. The parental subsystem in this case was struggling to function effectively. While the parental subsystem was trying to set the rules for the child for their safety, there was inconsistency in their communication and adherence to the rules between the mother and father, leading to ineffective regulation.
For example, when the child was trying to watch something on the screen late in the night, the father was very stringent about it and took away the device from the child from time to time; however, when the child got upset about this and either got angry or sulked to show his dissatisfaction, the mother handed him the device for a limited time; both parents seemed to be trying to set rules for the child, but the lack of consensus between them led to an inconsistent pattern of rules.
Additionally, boundaries refer to the rules that define “who participates and how much,” and these can be physical as well as psychological. They define the separation between people and subsystems in the family. In this family, there was a diffused boundary between the mother and the child, which means permeability was high and the relationship was characterized by enmeshment. The boundaries between the husband and the wife, and the child and the father were rigid, characterized by distance and very stringent rules of engagement.
The couple had difficulty relating to each other; though both were trying their best to function well as parents, they were not able to find comfort in each other. Both were going through the struggles of parenting their child independently, depending more on sources outside of the family. For the father, it was his friends, and for the mother, it was her sister. However, they both were unaware of the struggle they were going through.
Furthermore, there were major deficits in communication and problem-solving in the family, which in turn were related to the dysfunctional family structure, which was also a focus of intervention.
Therapy
The focus of the 14 sessions was on psycho-education and contingency management for behavior problems. Communication between parents was worked on and problem-solving strategies were also briefly introduced to help parents and the child have an equitable say in the decisions affecting the child. Critical goals achieved during the initial phase of therapy were improved communication between the father and son, increased frequency of positive interactions and nurturance, and enhanced individuation in the boy, which strengthened the parental subsystem by helping parents complement each other in their roles as parents.
In the later phase of therapy, we worked to achieve increased self-efficacy of the system while encouraging the family to continue practicing the skills learned, encouraging positive and meaningful engagement of the family members with each other, and helping the family and the identified patient gain more support while continuing to be a consistent source of tertiary support for the family.
Toward the time of termination of sessions, the child and the family were doing well. The frequency and intensity of anger outbursts and irritability had significantly reduced. Furthermore, the parents and child were able to communicate equitably, where the parents were not putting undue pressure on the child but also communicating their thoughts and expectations, which were better received by the child. Following discharge, telephone-based sessions were conducted on an outpatient basis twice a week as the family did not have access to a smartphone.
The above two cases illustrate the relevance of family therapy principles while treating adolescents. In the following section, several guidelines are presented for similar application of family therapy in this population.
Therapy Practice Guidelines
Several basic family therapy principles can be blended with specific targets for families where an adolescent is the identified patient. An understanding of the role of family in mental illness; 30 clinical experience with the family therapy population in O’Leary, Heyman, and Jongsma’s work; 31 and sections on psychotherapy with children and adolescents in Massey and Massey’s book 32 have influenced the guidelines presented. In addition, Krueger and Glass 33 have published guidelines for integrative psychotherapy, including systemic CBT for child and adolescent population. At NIMHANS, Frank Dattilio’s work on cognitive-behavioral family therapy 34 and Susan McDaniel’s psychotherapy video 35 on family therapy with an adolescent girl in a blended family have been powerful influences on the training and practice of family therapy.
Fundamental Principles
An organized understanding of mechanisms of change and common factors across treatments can be used to provide a sound scientific basis for productive psychotherapy work with this population. Viewing the work from a preventive perspective is relevant, no matter how difficult or challenging.
A high level of investment in psychotherapies with good outcomes could reduce mental health challenges for the identified patient and others across their future family life cycle stages. The benefits can extend to the family of procreation later for the identified patient as well. This viewpoint is the best professional attitude for the team while starting work with any child or adolescent family case.
Creating a working therapeutic alliance with each family member close to the treatment setting, being directive, and not using patient-driven principles for the overall therapy plan are essential. A therapist’s capacity to handle therapeutic alliance ruptures and repairs in an authentic manner, as emphasized by the Satir model is also critical. Using relevant dimensions of therapeutic alliance across sessions, as well as during different segments of the sessions, will strengthen the therapeutic engagement of everyone.
Bringing out good intentions of those adults toward the identified patient before focusing on dysfunctional behaviors, interactions, beliefs or cognitions, attitudes, and emotional responses is a good way to support changes through therapy. Developing and holding a respectful attitude toward the family is the hardest yet crucial for this population.
Guidelines for Formulation and Goal Setting
The following points can be used to develop an informed impression of the family and identify goals for intervention.
Apart from the presenting problems and symptoms of the identified adolescent patient, arguments about parenting and other matters, lack of agreement or ineffective use of strategies for negative adolescent behaviors, and lack of support from the other parent on parenting styles are the standard problem definitions for these families. These can become short-term goals of family therapy with this population. Therapists can discover long-term goals after a deeper understanding of the family system and collaboratively articulate this with the family over time.
During assessment, it is helpful to obtain facts about the index family composition throughout the relevant family life cycle stages. Members with high interaction with the adolescent should be part of themes and conversations in family and individual sessions of the patient and family member(s).
Initial impressions of the clinician about significant subsystems involving the child or adolescent need to be used. The form of the subsystems is less critical than boundaries and affective dynamics in the family. One can target changes in boundaries and hierarchies as the adolescent may often be caught between conflicts among adults.
It is important to diagnose systemic vulnerabilities even if not involving the child directly, especially in the present (e.g., illnesses, the mental health of family members, conflicts with other systems, etc.). The welfare of various family members must form the background of the interest of the identified patient.
If more than one family member has mental health vulnerabilities, family therapy is essential, irrespective of individual treatments or therapies. The goals should focus on mutual support of family members regarding mental health issues. Narrative therapy and behavioral principles may be helpful to stabilize and empower the members regarding illnesses, labels, inadequacies in roles, implicit blaming of members individually or as a whole family by professionals, social networks, or any other experiences that may have disempowered the family members.
While the above forms the knowledge base for the clinician, specific case details will influence the work across sessions.
Guidelines for Intervention
There are many schools of family therapy that offer perspectives on why the problems have developed and what can be done to activate change. It is important to choose the orientation and techniques based on the unique needs of the family, the context in which treatment is being offered, the skill level of the therapist, and so on. Structural, cognitive-behavioral, and emotion-focused theories offer a good set of perspectives and techniques that can be either used as a singular approach or blended using principles of psychotherapy integration, especially assimilative integration.
Using resources that the family brings to treatment, current structural diagnosis, emotional development, affective and attachment aspects, and development of social-emotional skills are emphasized in structural family therapy. Short-term clinical goals can be symptom relief, whereas long-term focus is on growth-promoting practices. 25
Cognitive-behavioral family therapy can be used in varied ways. Focusing on beliefs may be a better starting point in family sessions rather than concentrating on interactional changes initially. This strategy could promote more participation and less defensiveness from everyone. In sessions with certain subsystems, interactional changes in sequences of specific interactions may be explored and encouraged. Connections between the two themes across the types of sessions help alter rigid patterns of thinking and acting.
Emotionally focused family therapy principles can be used to help families identify attachment needs, express them, and promote positive cycles of interactions around these.
Additionally, for work with this population, directive interventions like psycho-education are beneficial. The therapist can recommend that adults practice some privacy on conflictual themes and refrain from conversations about differences in the younger generation’s presence. This practice is critical even if there have been no secrets from the child. Often, a focus on this alone is quite common over several contacts with parents, especially at the beginning and end part of the sessions.
Furthermore, the family’s adaptability resources for conflict resolution and problem-solving can be improved through even one member or parent. Use of circular questioning is effective to alter various adult members’ skills in the above and encourage them to communicate content to others in their dyads.
Phases in Therapy
Family therapy with adolescents can be planned in a phase-wise manner with the following points to keep in mind.
Initial Phase
This phase aims to discover specific maintaining factors for the presenting problem and initiate tentative interventions for trial systemic changes. At least one family system domain should be focused on to test its flexibility and promote resilience and strength in the least complicated part. The hope-building style of the clinician or therapist is critical along with paying attention to therapeutic alliance.
In two-parent families, in conjoint sessions with the parents, the therapist can examine relevant here-and-now aspects of their family functioning, a typical day’s routine, examples of interactions on holidays and vacations, descriptions of their interactions, and concerns about other children (if any) or other family members.
Moreover, they must be helped to appreciate each other’s qualities in various relationships before making them elaborate on their disappointments with each other, if any. Children or adolescents need not be part of these sessions. Such initiatives could facilitate healthier intergenerational boundaries in the long run.
If only one parent is available to the clinician, one should avoid bias toward the other. Chronic marital difficulties may have often contributed to coalitions against the absent parent, and these may continue to expand and engulf any system in the family’s proximity, including the clinician.
In interviews, therapists must often address non-dominant themes with concentrated effort. Spontaneously brought up content and clarifications surrounding those are inadequate for developing a systemic view of the family. Conversations about the future of their relationships and psycho-education about what healthier and adaptive interaction could look like can be gently initiated in the sessions.
If couple therapy is indicated for the parents, increasing their motivation for new goals for their relationship and showing the importance of stabilizing relationships between adults and identified patient irrespective of conflicts among adults are essential steps. Often, with the overall welfare of everyone in the forefront, the vulnerable parent also usually gets comfortable with individual evaluation and therapy once the dialogues in the family make each one feel safe with the family members.
In single-parent families or atypical families, a systemic understanding of all those who live under the same roof, a description of their interactions, shared goals and strategies, communication, problem-solving sequences, etc. can be obtained in initial sessions. This agenda may be done through whichever family member is available. A typical systemic hypothesis and evaluation may not be beneficial. Post-modern approaches or affect-focused perspectives could be used before behavioral or interactional guidance.
Middle Phase
The more the sessions can be organized involving adult members, the better for the family system. Younger generation subsystems can be in therapeutic connection but only necessarily be engaged in tasks in the sessions if the session tasks are to improve communication styles. Periodic family sessions, including children, will make changes tangible, systemic, and closer to the reality at home.
However, suppose there is an exceptionally high degree of family pathology involving abuse, violence, secrets, etc.; in that case, empowering the younger subsystems and building more robust networks for safety and growth can become the primary agenda in designing sessions. Finding resources from the family of origin through siblings, cousins, friends, neighbors, etc. for the lone parent engaged with the clinician would be beneficial when dealing with young children.
Generally, the long-term availability of the treating team or therapist must be mentioned clearly for this population. Helping everyone develop their mental health index over their life course and responsibility toward one’s welfare and the welfare of others in the family need to be emphasized. The family members are free to choose to maintain these goals from within-family resources, self-help books, or guidance from well-wishers or professionals, provided they monitor the outcome and take steps accordingly. The discussion must include generic systemic and mental health perspectives regardless of the short-term or long-term goal(s) during this phase or the type of techniques/theory.
Termination Phase
Termination can be guided by the adult or parent attending the family sessions, as they can judge the appropriate dependency they have on the therapist and where they are somewhat self-sufficient. Follow-ups can often be frequent after termination, which helps them feel supported with engaging in any new learning. The identified patient’s points of view can be valued to the extent that they choose to participate or not in the session.
Conclusions
Literature on family therapy with the adolescent population is not free of controversies. For example, the effectiveness of certain well-established models like functional family therapy used mostly in high-income countries is not established yet. 36 RCTs report a good outcome for suicidal ideation but not for depression. 37 . Moreover, several terms such as “family-focused treatment,” “parent management training,” “attachment-based family therapy,” “systemic family therapy,” “structural family therapy,” “brief-strategic family therapy,” “psycho-education to family about identified patient’s illness,” “family-focused CBT,” etc. create heterogeneity in research plans and conclusions. Yet, there is no doubt that these psychotherapies are integral to treatments for adolescents.
Interestingly, while the field of family therapy grew from the child and family therapy clinics in the West, in India, the child and adolescent services use only a limited aspect of the family system. Nevertheless, psychotherapies that utilize family resources differently for the benefit of this population have a lot of scope in cultures like ours where there is limited or no support systems for children and adolescents other than families.
Footnotes
Acknowledgements
The authors acknowledge trainee therapists Ms. Samridhi Pahalwaan and Ms. Silpa and the families for inspiring the case reports.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
As the article is not a single case study and details have been used for illustration purposes, patient/family consent was not obtained. The article focuses on the therapist’s account and academic submissions and their contributions have been acknowledged.