
Abstract
Objective:
To assess the emotional problems associated with digital-screen exposure (DSE) among 2–5-year-old children in Chandigarh, North India.
Methods:
A cross-sectional study was conducted among 400 randomly selected families with children aged 2–5 years using the validated DSE questionnaire and the standard preschool-child behavior checklist from October 2017 to March 2018. The American (2016) and Indian (2020) Academy of Pediatrics guidelines were followed to define excessive DSE. To estimate the probability for the predictors of emotional problems with DSE, we performed the per-binary multivariate logistic regression model, giving an adjusted odds ratio (AOR), using IBM SPSS Statistics for Macintosh, Version 25.0.
Results:
The mean age of the children was 3.5 years (standard deviation = 0.9). Nearly 15% of children were with borderline/clinical cases of emotional problems. The significant protective factors for individual emotional problems among children were watching learning media content [Oppositional defiant disorder (AOR = 0.39 CI 0.22, 0.72, p = 0.002)], having DSE less than one hour [Attention deficit hyperactivity disorder (AOR = 0.19 CI 0.08, 0.43, p<0.0001)], presence of media rules at home [Sleep problems (AOR = 0.03 CI 0.001, 0.69, p = 0.028)], age of initiating DSE before two years [Total emotional problems (AOR = 0.5, 0.22, 0.93, p = 0.03)], and caregivers DSE of less than two hours per day [Depression (AOR = 0.04 CI 0.002, 0.75, p = 0.031)]. While the significant predictors were playing outdoors almost every day [Total emotional problems (AOR = 2.2 CI 1.06, 4.78, p = 0.034)], average activity of less than 30 minutes per day [Total emotional problems (AOR = 2.4 CI 1.22, 4.73, p = 0.01)], boys [Total emotional problems (AOR = 2 CI 1.08, 3.55, p = 0.028)], children aged less than 3.5 years [Total emotional problems (AOR = 1.9 CI 1.05, 3.59, p = 0.03)] and higher socio-economic status [Withdrawn (AOR = 5 CI 1.19, 20.97, p = 0.028)].
Conclusion:
There was a moderate prevalence of emotional problems among children with excessive DSE. Specific emotional problems were significantly associated with the DSE among children.
Introduction
The digital landscape is evolving more quickly than the research on the effects of screen-based media on the development, learning, and family life of young children. A survey of American parents of 0–8 year olds concluded that children’s access to mobile devices had alarmingly increased from 52% in 2011 to 75% in 2013. 1 Television (TV)-watching time is significantly associated with reduced psychosocial health, emotional functioning, social functioning, school functioning, and total Health-Related Quality of Life among children. 2 A prospective European cohort study in toddlers and preschoolers observed that TV-viewing is perpetually associated with emotional and peer problems. 3 Digital-Screen Exposure (DSE) was observed to be negatively associated with prosocial behavior, but positively associated with hyperactivity, peer problems and conduct problems in a longitudinal study conducted among 6–10-year-old Australian children. A high DSE is also related to the development of emotional behavior problems in younger children, whereas it is associated with development of hyperactivity and conduct problems, in older children. 4
Further, caregivers and parents play an essential role in developing the media habits of children. An Indian hospital-based study on children (less than 15 years of age) observed that children who watched mobile phones excessively developed mental health issues such as temper tantrums (45.3%), becoming anxious (44%), poor sleep (32.5%), irritability (29%), disobedience (26.6%), decreased school performance (21.4%), not mixing up with friends (11%), and fighting with friends (7.3%). 5 A recent review suggested interplay of various factors affecting the behaviors of children at four levels, including the intrapersonal-, interpersonal-, immediate environment- and macro environment-level. 6 Scientific literature also supports the benefits of high-quality preschool programs for improving learning outcomes, 7 enhancing literacy skills, developing vocabulary, and comprehension with interactive media for children aged 2–8 years. 8 Besides, the American Academy of Pediatrics 2016 guidelines recommend age-appropriate, adult-supervised, content-specific, and interactive digital programs for the child’s overall growth and development. 9 Thus, interventions should focus on high-quality media parent supervised content to efficiently reduce DSE among children.
But, the majority of the studies calculated DSE considering only the TV-time. There is limited literature on the cumulative time spent on all electronic devices used by the children, especially among the 2–5-year age groups. Six in ten Indian children (2–5-year-old) have DSE higher than that recommended (more than 1 hour) for their age. 10 The average DSE of American children has risen from 2.2 hours per day at 1-year of age to 3.6 hours per day by 3-years of age. 11 Correspondingly, the period from birth to 5 years is critical for establishing healthy habits of minimal sedentary behaviors and overall well-being. 12 So, it is rational and pertinent to prevent the practices of excessive sedentary behavior at an early age. An Indian study reported a delay in achieving cognitive milestones for children (below 2 years) with excessive DSE. 13
However, most of the evidence pertains to children from developed countries.7,8 A review highlighted that there is a relative lack of evidence on preschool psychiatric disorders. 14 Still, there is limited literature on Indian children in this particular age range. 6 Recently, the Indian Academy of Pediatrics (2020) have recommended age-appropriate permissible DSE limits for children. 15 But the associations of emotional behavior problems with DSE remain unexplored among young children, especially in the Indian context. 9 We hypothesized that it is expected to have higher emotional behavior problems among children with DSW > 1 hour per day. This study aimed to evaluate the emotional behavior problems among children aged 2–5 years, and their association with DSE in India.
Material and Methods
A cross-sectional study was conducted among 400 children of age 2–5 years old in Chandigarh, a Union Territory in North India, from October 2017 to March 2018. The sample size “n” was calculated using the formula “n = 4pq/l2”, where “p” is the prevalence and assumed as 50% of higher DSE, “q” is “p–1”, and “l” is the precision assumed 8. 16 We had assumed a non-response rate of 15% and design effect of two to counter cluster effect to have a final sample size of 360. Nearly 48 families (12%) refused to be a part of this study during household visits. As we had estimated the sample assuming a nonresponse rate of 15%, hence refusal rate was being taken care of at the time of sample size calculations. Also, we had recruited more (n = 400) participants than the calculated sample size (n = 360).
A multistage cluster random sampling technique was used to select the households/families from the study area. A cluster was assumed to be a catchment area catered to by an auxiliary nurse midwife (ANMs) in Chandigarh. Generally, she caters to a population of 4000 to 10000. The list of all the ANMs (n = 219) enrolled under the Reproductive and Child Health (RCH) program in Chandigarh, Union Territory, was obtained from the program officer. In the first stage we selected ten such clusters (nine urban and one rural), so as to represent Chandigarh’s population as per probability proportion to size by simple random sampling technique through generating random numbers on Microsoft excel, version 2019. The first nine clusters of ANMs for urban and one rural cluster were chosen. In the second stage, the annual health registers of the selected ANMs were obtained to identify and list the households with a two-to-five-year-old child, in their catchment area. From this list thirty-six households were selected by simple random sampling from each cluster to meet the desired sample size by computer generated random numbers. If a family was not available, then they were contacted over phone and revisited if they had given consent to be a part of the study. Eligibility criteria was family having at least one electronic device (screen-based media devices for example TV, computer, smartphone etc.). Each family was visited to their homes to obtain data from the principal caregiver of the child. The younger child was recruited in families with two or more children. Only children previously diagnosed with long-term or chronic, or congenital illnesses were excluded. The detailed methodology of the study has been described elsewhere. 10
Data Collection Methods
The lead author visited the selected households and interviewed the primary caregivers of the children face-to-face by using the following questionnaires:
DSE Measurement
A pretested, semi-structured, bilingual (in English and Hindi language) questionnaire called the digital-screen exposure questionnaire (DSEQ) was used. The DSEQ had good internal consistency (Cronbach α = 0.73–0.82) and good inter-rater agreement (kappa = 0.75, 95% CI 0.72–0.78).10,17,18 DSEQ was used to get information from the child’s primary caregivers. The information regarding the digital media content watched by the children was obtained by asking 12 questions included in the pretested and validated Digital Screen Exposure Questionnaire. 17 It was segregated into educational and noneducational digital media content. Educational content included using media devices for completing homework assignments, for learning poems, rhymes, ABC etc., learning math, numbers, tables, to recognize shapes/sounds/colors, to learn letters, words, vocabulary, language, to draw, write, to watch stories etc. Non educational media content included video calling applications to talk to the family/friends, to watch adult programs (soap opera, news, sports, movies etc.), to watch random things for enjoyment (music, advertisements, babyTV, click photos etc.). The questions to assess the level of physical activity of the child were taken from PrePAQ and translated in Hindi. 19
Emotional Behaviors Measurement
A standard Preschool-Child Behavior Checklist (Pre-CBCL) was used to assess the child’s emotional and behavioral development and was proxy-reported by the primary caregivers. It has been validated and used in Indian settings and has good internal consistency (Cronbach’s alpha = 0.95). 20 It is a 100-item screening checklist that is used to identify children with behavioral or emotional behavior problems. Each item (behavior) was scored as 0 (absent), 1 (occasionally present), or 2 (very often present). The pre-CBCL’s categorizes different emotional behavior problems into separate problems scores, as well as composites namely, emotional reactivity, attention deficit, somatic complains, withdrawn, sleep problems, attention problems, depression, anxiety, autism spectrum disorders, aggression, internalizing problems, externalizing problems, attention deficit hyperactivity disorder, oppositional defiant disorder, and other emotional behavior problems. Each emotional problem is further divided into “normal”, “borderline case” and “clinical case” based on computed scores.
Data Management and Analysis
IBM SPSS Statistics for Macintosh, Version 25.0, was used for data management and to perform statistical analysis. For each emotional problem the “borderline cases” and “clinical cases” were combined and compared with “normal” children for easy comparison. Each emotional problem had a separate score range to categories them into normal, borderline case, and clinical case. Emotional behavior problems were total emotional behavior problems (normal = 0–51, borderline case = 52–60, clinical case = 62–200), emotional reactivity (normal = 0–5, borderline case = 6–8, clinical case = 9–18), somatic complains (normal = 0–4, borderline case = 5–6, clinical case = 7–22), anxiety/depression (normal = 0–6, borderline case = 7–8, clinical case = 9–16), withdrawn (normal = 0–4, borderline case = 5, clinical case = 6–16), sleep problems (normal = 0–7, borderline case = 8, clinical case = 9–14), attention (normal = 0–5, borderline case = 6, clinical case = 7–10), depression (normal = 0–5, borderline case = 6, clinical case = 7–20, anxiety (normal = 0–7, borderline case = 8, clinical case = 9–20), autism spectrum disorders (normal = 0–6, borderline case = 7, clinical case = 8–24), aggressive behavior (normal = 0–20, borderline case = 21–24, clinical case = 25–38), internalizing problems (normal = 0–13, borderline case = 14–17, clinical case = 18–100), externalizing problems (normal = 0–20, borderline case = 21–24, clinical case = 25–100), attention deficit hyperactivity disorder (normal = 0–9, borderline case = 10, clinical case = 11–12), and oppositional defiant disorder (normal = 0–7, borderline case = 8, clinical case = 9–12). Based on previous literature this tool has been used for assessing all of the emotional and behavioral outcomes hence, it was used in its redundant form. The data were analyzed based on the total emotional behavior problems, and its sub-categories as categorical (normal versus borderline and clinical cases) and continuous variables (scores). The emotional behavior problems among children were the dependent variable while, DSE of children and its correlates are the independent variables.
The American Academy of Paediatrics, 2016 guidelines had considered DSE excessive if it was more than 1 hour per day by any electronic device.
9
There is evidence that a child’s DSE varied on the weekdays and weekend days.
21
Hence, the child’s average DSE (by all electronic devices) per day on a weekday and separately on a weekend day was calculated. As there are five weekdays [Monday to Friday] and two weekend days [Saturday and Sunday] in a week, the weighted average DSE per day in a week was calculated as:

In the results section, the DSE was expressed as a categorical variable (categorized in two categories, including the proportion of children with excessive DSE of more than 1 hour and less than 1 hour) 9 and a quantitative variable (measured as the duration in minutes).
For the Analysis of Categorical Variables
The average DSE of the child had two categories, i.e., the proportion of children having DSE of less than 1 hour and those with more than 1 hour (excessive) per day. The chi-square tested the significance (P < 0.05) of the difference in proportions between the groups (emotional behavior problems versus DSE exposure). This study considers the level of significance at 95% confidence intervals. To estimate the probability for the predictors of emotional behavior problems (coded as having emotional behavior problems versus no emotional behavior problems), we performed the per binary multivariate logistic regression model giving adjusted odds ratio (AOR). The list of dependent and independent variables has been shown in Table A1.
For the Analysis of Continuous Variables
The correlation (r) test to see linear relations of emotional behavior problems (scores) with a) duration in minutes of weighted average DSE of the child (summing up the TV, smartphone, computer/tablet, etc. viewing-time), b) the weighted average of the level of physical activity of the child on a casual day as per the responses by the primary caregiver and c) average DSE of the primary caregiver of the child (based on the questionnaire). 17
Results
Background Characteristics
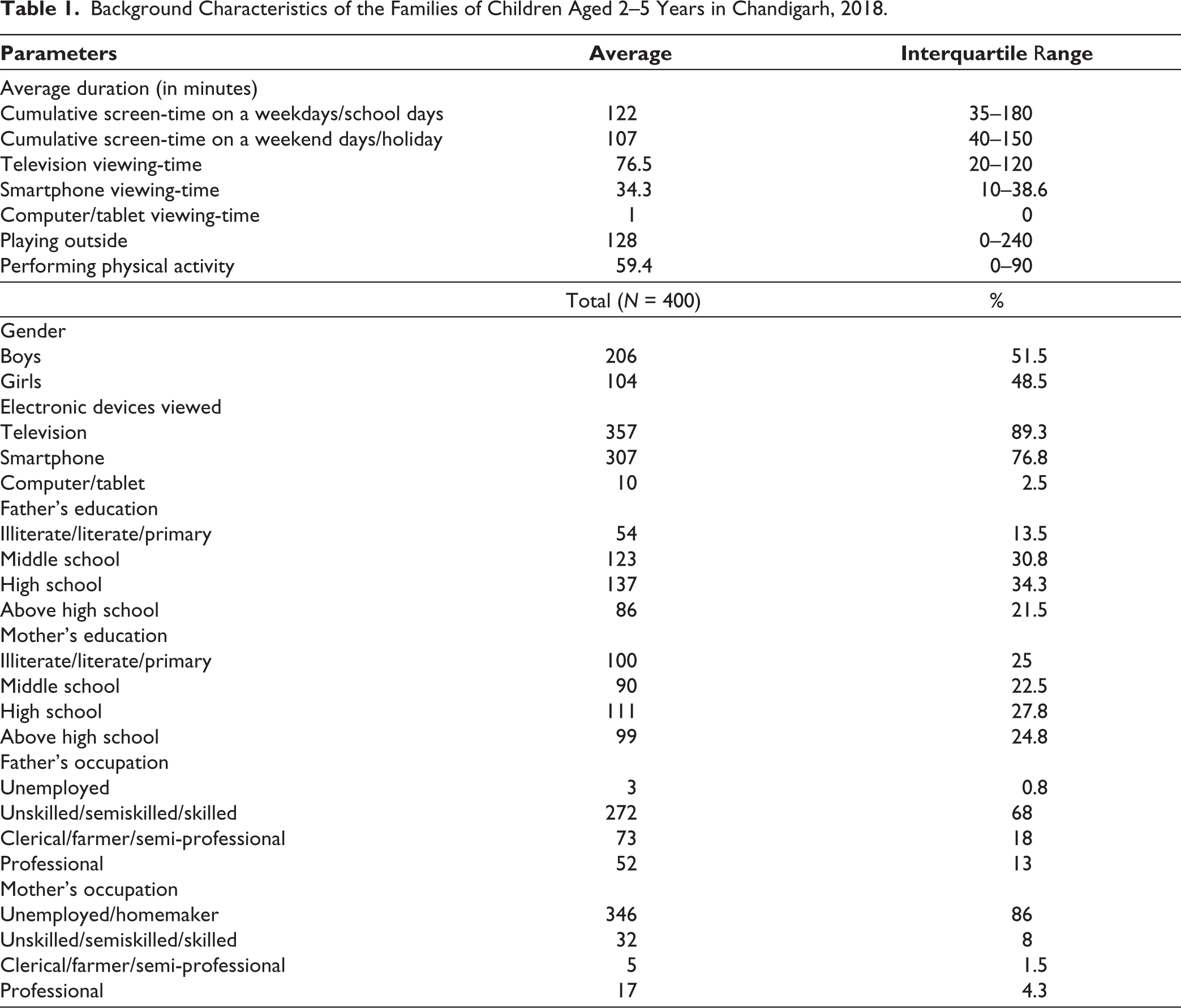
Children were on an average of 3.5 (standard deviation of 0.9) years old. There was an equal representation of boys (51.5%) and girls (48.5%). Most fathers (34.3%) and mothers (27.8%) had education levels up to high school. Fathers were primarily unskilled/semiskilled/skilled (68%), and mothers were homemakers (86%) (Table 1). On a typical (performing the usual activities) weekday, DSE’s average duration was 2 hours, while, on a typical weekend day, DSE’s average time was 1.8 hours. TV was most watched ED (76.5 min per day). Children played outside daily for 2 hours and performed physical activity for 1 hour.
Background Characteristics of the Families of Children Aged 2–5 Years in Chandigarh, 2018.
Prevalence
Emotional Behavior Problems
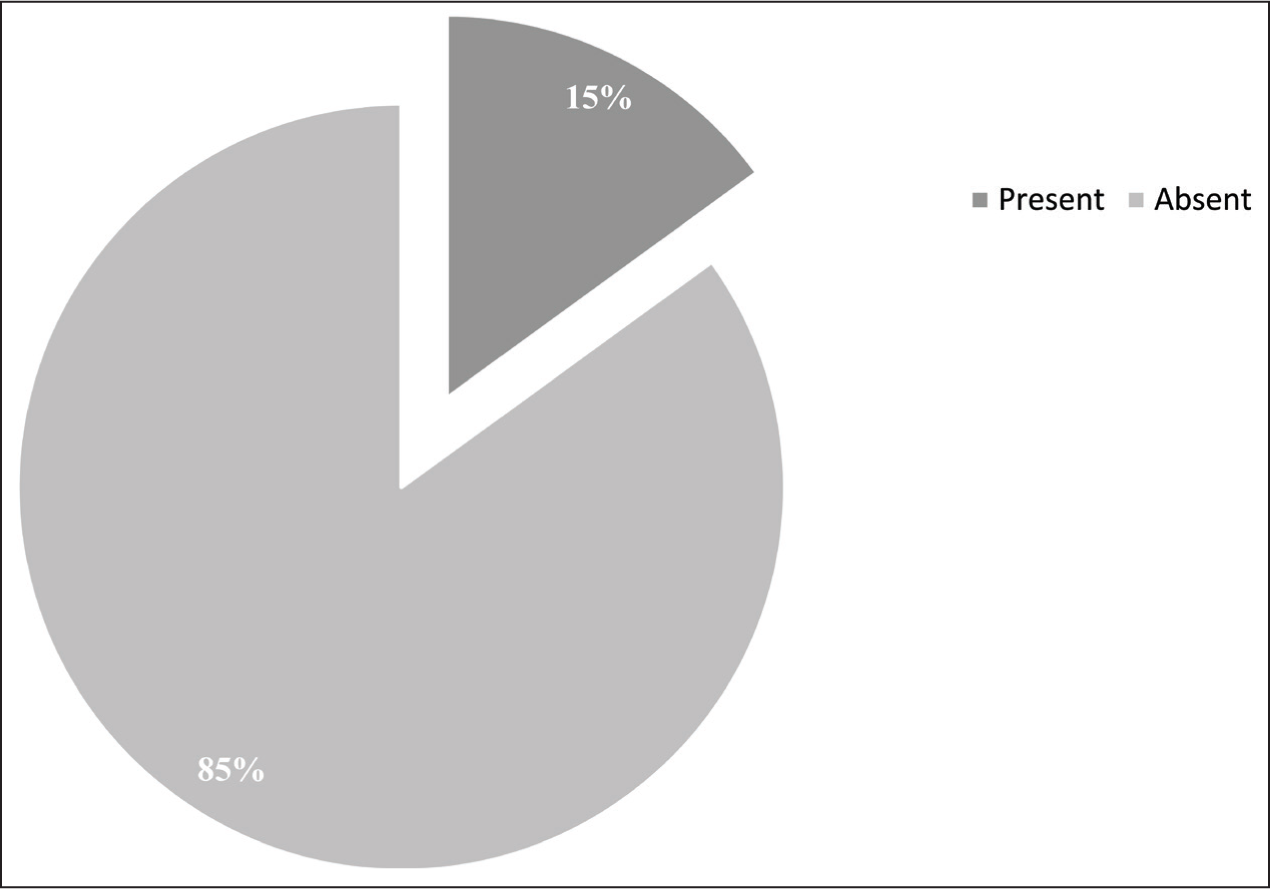
Nearly 15% of children were categorized into borderline/clinical cases of some emotional behavior problems (Figure 1). Out of all emotional behavior problems, most children were suffering from externalizing problems (30%) (Table A2).
Prevalence of Emotional Behavior Problems Among Children.
DSE
About 40.5% of children had DSE within the permissible limits recommended by the American Academy of Pediatrics 2016 guidelines, 9 of watching electronic devices for less than 1-hour duration per day. The results of the prevalence study are given elsewhere. 4
Bivariate Associations of Emotional Behavior Problems with DSE
Excessive DSE (more than 1 hour) was significantly (P < 0.05) associated with attention problems (27.3% versus 17.7%), aggression (26.1% versus 10.5%), internalizing problems (9.2% versus 3.7%), externalizing problems (35.7% versus 21.6%), attention deficit hyperactivity disorder (18.5% versus 4.9%), and oppositional defiant disorder (23.1% versus 11.1%) in comparison to DSE of less than 1 hour (Table A2).
Correlates of Emotional Behavior Problems
This study also examined the associations as a continuous variable (DSE from all devices used routinely in minutes per day) and found a significant relation (P < 0.05) of excessive DSE with total emotional behavior problems (r = +0.31), emotional reactivity (r = +0.31), somatic problem (r = +0.1), anxiety/depression (r = +0.14), sleep problems (r = +0.1), attention (r = +0.2), depression (r = +0.2), aggression (r = +0.3), internalizing problems (r = +0.2), externalizing problems (r = +0.3), attention deficit hyperactivity disorder (r = +0.3), oppositional defiant disorder (r = +0.3), anxiety (r = +0.1), autism spectrum disorder (r = +0.1) and other emotional behavior problems (r = +0.2) (Table 2).
Correlations of Digital Screen-exposure with the Behavioral Correlates of Children Aged 2–5 Years in Chandigarh.
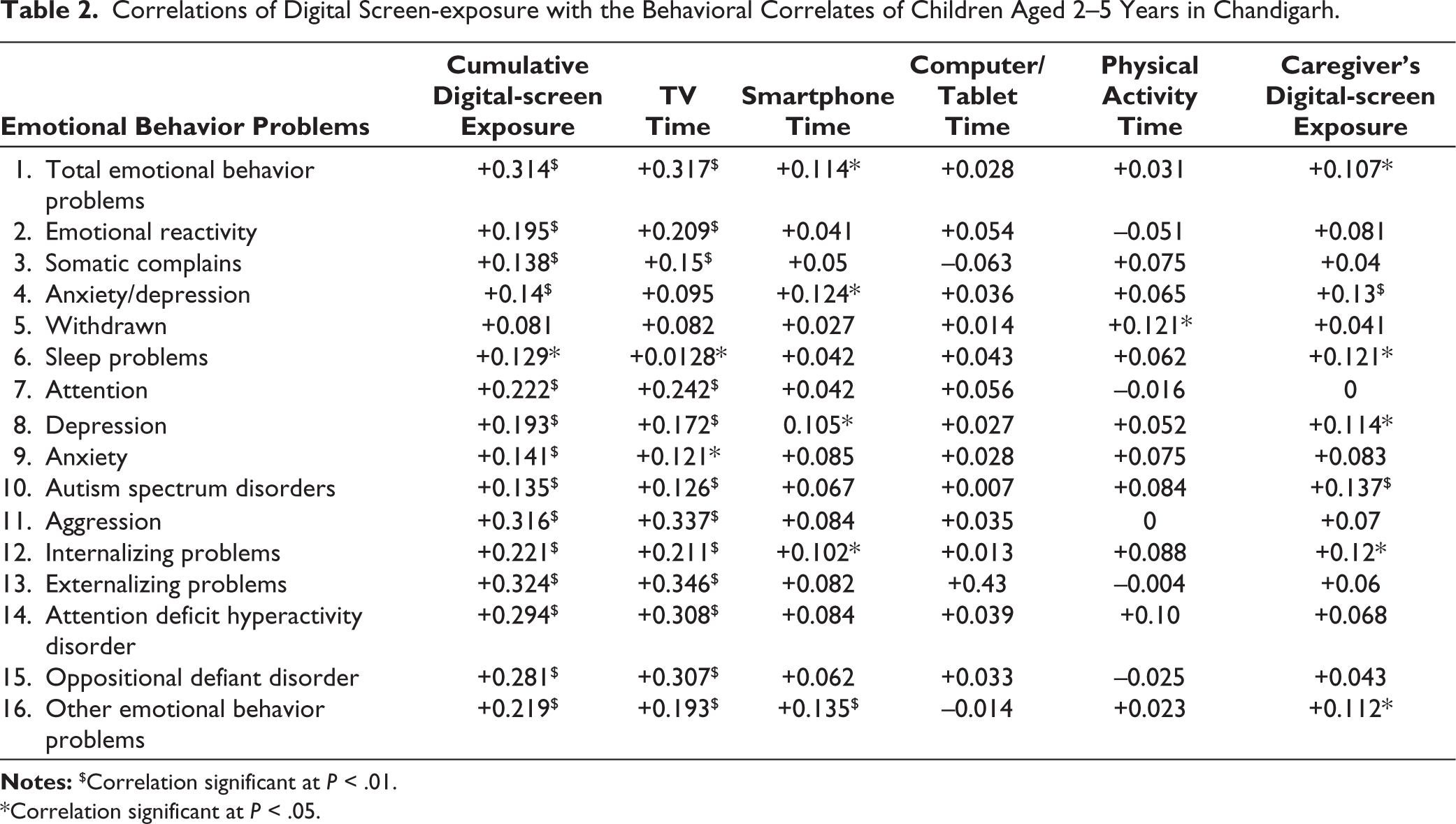
*Correlation significant at P < .05.
Predictors of Emotional Behavior Problems
Watching learning media content, average DSE of less than 1 hour among the child—within permissible limits, presence of media rules at home, initiating DSE after 2 years of age in children, average DSE of less than 2 hours per day among the caregiver’s—within permissible limits were significant protective factors of individual emotional behavior problems in Figure 2 and Table A3.
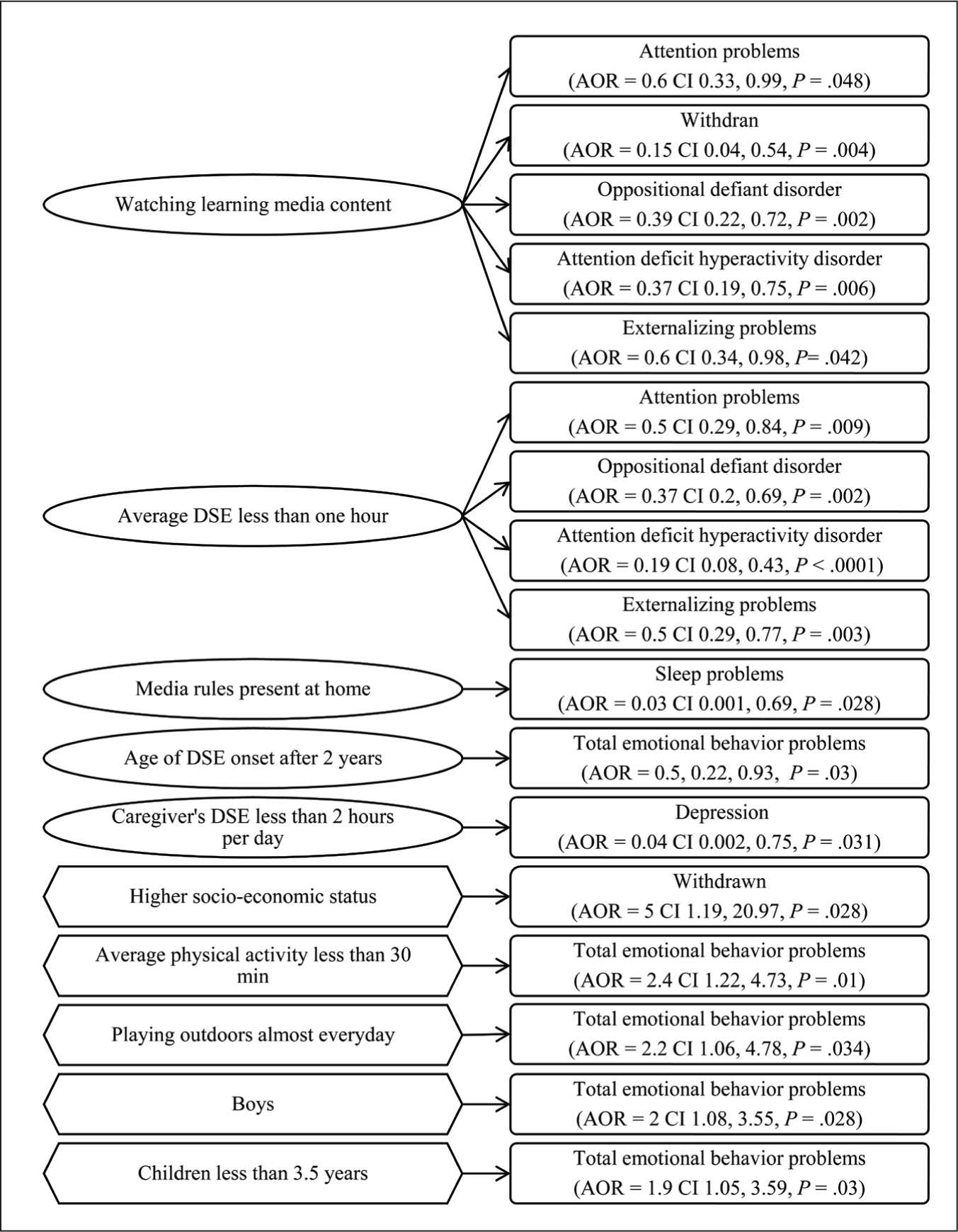
While the significant predictive factors of individual emotional behavior problems among the children as per binary multivariate logistic regression analysis were playing outdoors almost every day for developing total emotional behavior problems (AOR = 2.2, CI = 0.06, 4.78). Boys had more total emotional behavior problems (AOR = 2 CI = 1.08, 3.55). A higher socio-economic status was associated with becoming withdrawn (AOR = 5 CI = 1.19, 20.97 (Table A4)). Age of the child less than 3.5 years was associated with developing total emotional behavior problems (AOR = 1.9 CI 1.05, 3.59).
Discussion
The present research focuses on the social-emotional developmental problems that might arise in children aged 2–5 years due to excessive DSE. Few children were categorized into borderline/clinical cases of individual emotional behavior problems like externalizing emotional behavior problems. Bivariate association of excessive DSE was significantly observed with attention problems, aggression, internalizing problems, externalizing problems, attention deficit hyperactivity disorder, and oppositional defiant disorder. The significant protective factors for not developing an emotional behavior problem as per binary multivariate logistic regression were watching learning media content, average DSE of less than 1 hour among the children (within permissible limits), presence of media rules at home, initiating DSE onset before 2 years in children, average DSE of less than 2 hours per day among the caregiver’s (within permissible limits). While the significant predictive factors of individual emotional behavior problems among were playing outdoors almost every day, being a boy child, belonging to a higher socio-economic status, and younger age (less than 3.5 years).
A longitudinal community study in 9–13 years old American children noticed that nearly one-fourth of boys and one-third of girls had at least one psychiatric disorder, which increased by 16 years of age. 21 Also, a review highlighted that the rates of psychiatric disorders and comorbidity patterns among preschoolers are similar to older children. 14 An Indian study 22 concluded that 22.7% of children aged 6–18 have emotional behavior problems, which was higher than the present study (15%). This difference could be due to age differences among the study participants and differences in assessment instruments. The former research reported that Indian children mostly have anxiety, hyperactivity, argumentativeness, attention-deficit hyperactivity disorder, and externalizing problems. 22 The frequencies of emotional behavior problems were different in our sample, as the former study was done in 6–18-year-olds from Karnataka, which is in South India. American researchers revealed that the range of rates of childhood disorders were: attention-deficit hyperactivity disorder from 2% to 5.7%; oppositional defiant disorder from 4% to 16.8%; conduct disorder from 0% to 4.6%; depression from 0% to 2.1 %; and anxiety disorders from 0.3% up to 9.4%. 14 As externalizing problems are more evident; hence, the frequencies might differ in different geographical areas and home environments. An American study summarized that less than half of youth receive mental health specialty treatment for severe disorders. 23 Besides, Merikangas et al. 23 asserted that young children should be included in epidemiologic surveys to evaluate their psychological and physical health.
TV was the most popular electronic device used by children, followed by smartphones and handheld videogames in this study, which was comparable to the findings of a review by Pearson and Biddle, 24 and studies from Asian countries (India, 5 and Korea 20 ). Nevertheless, a study conducted in 2013 among American children (0–8 years) observed that children had shifted from viewing TV to touchscreen devices. 1 In light of these differences, we studied the relations of individual emotional behavior problems with time spent separately on TV, smartphone, and computer/tablets by the child, average physical activity of the child, and caregiver’s average DSE of the child. The primary emotional behavior problems associated with any type of electronic device were total emotional behavior problems, depression, internalizing problems, externalizing problems, autism spectrum disorder, withdrawn, and other emotional behavior problems. The differences in the association of individual electronic devices and emotional behavior problems were due to the variability in the frequency and time spent on them. However, there are not any studies that compare the individual emotional behaviors with specific electronic devices used by children.
An Australian study among six and 10-year-olds found that high DSE led to emotional behavior problems in younger children, while older children developed hyperactivity and conduct problems. The prime moderators of DSE were household income, parental level of education, and neighborhood socio-economic status. 4 The present study observed gender-based differences in having emotional behavior problems among the study participants. Similarly, a longitudinal community based study in 9–13 years old American children noticed that the risk from a previously diagnosed emotional problem was significantly higher among girls. 21 Also, girls have more mood and anxiety disorders, and boys have more significant behavior disorders, whereas there is an equal gender ratio for substance use disorders. 23 Due to the study design, we cannot comment on the temporal associations of demographic characteristics with emotional behavior problems, but further studies need to explore these associations from a country-specific perspective. In a recent (2017) Canadian study, excessive DSE had negative associations with kindergarten children’s school readiness, which was proportional to the increase in their family income. 25 So, future interventions should focus on young children to limit the progression of mild emotional behavior problems severe forms.
As parents are a liaison between the child and the service providers, mental health issues among children need to be normalized. This would improve pediatric service utilization and lessen the challenges of service providers in delivering sound advice. The prevalence of excessive DSE (59.5%) in our study can be compared to a Malaysian study (63.05%), including children aged 0.5–12 years. 26 However, the prevalence of DSE is notably lower than Canadian children (82%) aged 3–5 years old. 27 These differences in the DSE prevalence in children were probably due to DSE guidelines for nearly a decade (2001), whereas Indian DSE guidelines were recently introduced in 2020. Also, developed countries have better and increased access to electronic devices than developing countries like India. An American study reported that excessive DSE, specific digital-media content, and age of starting DSE were significantly related to poor impulse control self-regulation and mental flexibility of the developing preschoolers. 28 Besides, the American Academy of Pediatrics advises families to make a customized family media plan, including the children in decision-making. 9 However, digital-media content in children was not significantly related to the child’s DSE as very few children watched any educational videos in the current study. Additionally, when the parents have to work in a nuclear setting, they offer the child to watch electronic devices without supervision. Probably this unsupervised and non-specific content watched by the child leads to excessive DSE. While in a joint or an extended family, other family members might aid in caretaking, have other screen-free rooms, and siblings to play with that might act as distractions.
The age of initiation of DSE in children was significantly related to the excessive usage of electronic devices. This can be due to a lack of national guidelines and parental literacy regarding DSE. Since caregivers” perceptions and attitudes play such an important role; hence, researchers need to plan longitudinal studies. Intervention studies have determined successful strategies to reduce excessive DSE along with significant long-term effects in the past. 6 In preschoolers, it is assumed that attentional controls and symbolic thinking are too immature to convey knowledge from screen to actual life. 29 Though scant research has been conducted on children younger than two years. Still, the interactivity of touch screens is limited compared to teaching adults. For infants and toddlers, the primary way of learning from passive or interactive media is through interaction with caregivers (co-viewing, teaching them about the content, and repeating this teaching). So, without involving caregivers while viewing digital media is unlikely to be educational. 30
The American Academy of Pediatrics guidelines strictly recommends involving children in active play after 1 hour of sitting or any stationary activity. 9 In a systematic review, studies learned that higher duration or frequency of physical activity had significant advantageous effects on cognitive development of the child. 31 Furthermore, no studies in this review found that higher duration or frequency of physical activity led to a statistically significant unfavorable effect on the children’s cognitive development. Also, the present study determined that children playing for less than 30 minutes per day and children playing outdoors almost every day were significant predictors of developing emotional behavior problems. Children at home were primarily occupied in sedentary activities (lightly dancing/swaying, singing, talking, acting out the story, role-playing, sitting quietly, playing with toys, writing/drawing, and reading something) while viewing electronic devices or with electronic devices being played in the background (Figure A1).10,19 The role of physical activity and outdoor play frequency on emotional behavior problems emphasizes the need to focus on improving play areas in our study setting. Besides, schools and existing policies can be strengthened to mandate minimum physical activity levels in young children to alleviate emotional behavior problems.
The strengths of our study include the participants being representative of the population; hence, the present study’s results can be generalized to Chandigarh, India. This is the first community-based study on this topic and age group in India that estimates DSE prevalence and its associated factors among children aged 2–5 years. We designed a tool to estimate DSE’s prevalence and covariates with a validated questionnaire used in the Southeast Asian countries. We performed advanced statistical; analysis to interpret individual factors affecting various categories of emotional behavior problems in children. The inclusion of contextual factors provides a broader perspective of DSE on a child’s behaviors. This study’s results might reinforce the role of primary caregivers or parents and digital-media rules at home.6,9 Parents, caretakers, teachers, and healthcare providers need to be aware that an accentuated DSE may associate emotional and social behaviors and the overall growth of young children. However, longitudinal studies need to explore these effects in the long term.
Despite the numerous strengths, the cross-sectional design restricts the study’s generalizability. So, the results should be interpreted with caution among varied populations. In addition, the cross-sectional analyses and dichotomized variables might not examine all the potential explanatory factors. Hence, results need to be interpreted carefully regarding sleep habits for children 2–5 years old. However, as the investigator did not directly observe the participants, there are chances of the parent’s social desirability bias and recall bias. Obtaining information on the specific TV shows/programs and their duration that the child watched last week preceding the survey minimized these biases. Lastly, this was a cross-sectional study that might not conclude distinct causation of emotional behavior problems with DSE. These associations can be confirmed with long-term based temporal studies. Finally, this study was restricted to questioning the parents only, which might not have detected potential cases of sleep problems. So, both parents and children should discuss their views on the child’s ST so that the scope for mental health professionals and experts to execute customized interventions in future studies. Lastly, the present research does not emphasize the underlying causes for parents not seeking health consultation despite confronting sleep-related disturbances in their children.
Conclusion
We conclude that most emotional disturbances are associated with DSE and its covariates among Indian children. Based on stepwise forward binary logistic regression analysis, the current study also concludes that the probability of having emotional behavior problems among the children was higher among boys, younger children (less than 3.5 years), children performing any physical activity for less than 30 minutes per day, children playing outdoors almost every day and children in whom the DSE was initiated before two years. This study addresses an urgent need for systematic information tracking system on children’s mental disorders. Examining the impact of modifiable risk factors of emotional behavior problems on a long-term basis; might help develop effective interventions to reduce DSE among young children.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Ethical permission was granted by The Postgraduate Institute of Medical Education and Research’s Ethics Committee (INT/IEC/2019/000711). Written informed consent was taken from the caregivers.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.