
Abstract
Psychotherapy of different types is recognized across the globe as an essential component of child and adolescent mental health services. At the same time, there are barriers and challenges in obtaining access to this modality that are as widespread as its acceptance. This article reviews barriers to accessing child and adolescent psychotherapy in high-income countries (HIC) as well as low/middle-income countries (LMIC). It also briefly reviews approaches to improve access using different interventions and modalities. We also report on our experience using one particular intervention, case management within pediatric collaborative care, as a promising approach for improving access in underserved populations.
Keywords
Introduction
Despite the evidence in support of the efficacy and effectiveness of child and adolescent psychotherapy, and the growing acceptance of this modality in the general population, there are still significant barriers to accessing this modality in high-income countries (HICs). Growing demand because of high rates of child mental health need, particularly after the COVID-19 pandemic, has resulted in major shortages of adolescent mental health services. It is estimated that, at best, one in three children in the United States suffering from a mental or emotional disorder receive any mental health services. In 2019, 13.6% of U.S. children between the ages of 5 and 17 years had received mental health treatment in the past 12 months, 10.0% of children had received counseling or therapy, and 8.4% had taken prescription medication. Minoritized children were less than half as likely to receive psychotherapy or pharmacotherapy.1, 2 The level of acute need has grown to such an extent in the United States, along with the shortages, that three major organizations (the American Academy of Child and Adolescent Psychiatry, the American Academy of Pediatrics, and the National Association of Children’s Hospitals) declared a national emergency in child and adolescent mental health in 2021. 3
Barriers to Access
Resources and Resource Distribution
There are multiple barriers to access to children’s mental health services in general and child and adolescent psychotherapy services in particular. Though relatively better resourced in terms of workforce, HICs have relative shortages of child mental health professionals, including psychiatrists, psychologists, and other licensed professionals. The United States and other developed nations often have significant problems with the geographic distribution of children’s mental health providers, with the great majority of these being located in urban and suburban areas, leaving both rural and inner-city areas significantly underserved. 4 Financial and sociodemographic disparities are also linked to geographic distribution as well as pose additional barriers themselves. There is often poor reimbursement for child psychotherapy services even under private insurance plans and especially under public insurance such as the Medicaid program in the United States. 5 Oftentimes, experienced and senior child psychotherapists will not accept insurance reimbursement, opting to only accept direct cash payments. This situation is typically better in Canada and European nations, which have some level of socialized medicine, but these disparities are also seen in those contexts. Added barriers to access faced by lower socioeconomic families include lack of mental health literacy and understanding of the role of psychotherapy, inadequate time (due to work schedules and other life demands) and means to transport children to psychotherapy sessions, and frequent interruptions due to personal or family crises/demands. 6
Lack of Training in Evidence-based Models
Although much of the data that has been developed on the efficacy and effectiveness of child psychotherapy has been with more systematic models involving well-trained therapists with established fidelity, much of the children’s mental health workforce that delivers psychotherapy lacks training in such evidence-based approaches, often practicing general supportive psychotherapy that is not focused on the clinical condition being treated. 7 This can often lead to either short-term and frequently interrupted therapy or long-term therapy with limited results, often not achieving the full potential benefits of the psychotherapies.
Stigma
Despite greater social awareness about the value of psychotherapy and mental health, supported by the popular media and messages from health officials, there is still a significant level of mental health stigma in the general population of HICs, oftentimes associated with level of education and economic status as well as with cultural and subcultural beliefs. It is not uncommon that working-class and rural families still experience self-stigma, family stigma, and community stigma around the use of mental health services and engagement in psychotherapy. This is even more pronounced in underserved minority populations, who already feel marginated because of their racial/ethnic background but fear being further stigmatized if they are found to use mental health services for themselves or for their children. 8
Racial/Ethnic Disparities
At the same time, besides all the previously mentioned barriers, additional ones experienced by racial/ethnic minoritized populations are the result of the lack of knowledge and skill by mental health providers in effectively addressing their mental health needs, considering their cultural values, beliefs, explanatory models of distress, and the unique sources of stress and trauma that they have experienced in their collective past and present. These have often led to problems around the acceptability of psychotherapy services being offered and ineffectiveness in their results, further aggravating racial/ethnic disparities in child mental health services, and this proportionately leads to either over-institutionalization or more significant adverse outcomes such as suicidality or contact with the legal system. Provider biases around the lack of benefit from psychotherapy among minoritized populations also serve as significant barriers and prevent even referral or implementation.9–11
Adverse Consequences
The lack of access to psychotherapy within children’s mental health services has also contributed to many additional adverse consequences. One of these has been an over-reliance on pharmacotherapy in the treatment of many childhood disorders, both for mild-to-moderate levels of impairment that could be addressed with psychotherapy and for contributing to excessive long-term reliance on psychotherapy for symptom management. Treatment with pharmacotherapy alone does not impart psychological insight or the learning of effective adaptive skills for children and families with more chronic conditions. Additionally, the lack of access to psychotherapy and an outpatient level of care often leads to the use of more frequent acute and restrictive, inexpensive levels of care for multiple acute episodes, contributing to higher overall costs of mental health services for children.12, 13
Barriers to Access to Child Psychotherapy Within Low-resource Nations: The Case of India
Children and adolescents form nearly one-third of the world’s population, and almost 90% live in low- and middle-income countries (LMICs).14, 15 India, now being the most populous country, is also home to the largest child and adolescent population (CAP), which forms nearly one-third of the country’s total population. Further, nearly half of mental illnesses have their onset in the child and adolescent age groups.16, 17 Epidemiological studies from HICs and LMICs have shown almost comparable rates of psychiatric illness in CAP, that is, in the range of 10%–20%.15, 18 However, the scarcity of research, heterogeneity across the studies, and varying socio-cultural factors and models of health systems in the HICs and LMICs limit the generalizability of available evidence across countries. 19 Furthermore, mental health–related psychosocial risk factors are more pronounced in LMICs, ranging from factors such as poverty, child abuse, displacement, exposure to crime, poor living conditions, lack of education, poor nutrition, and lack of access to health services. Family dysfunctions such as parental neglect, parental divorce, parental loss, poor parenting, domestic violence, etc. negatively impact a child’s mental health.
Practically, research on psychosocial aspects of vulnerable populations (with similarities to the population of LMICs) done across some HICs has been extrapolated for LMICs. Otherwise, most of the currently available research pertaining to interventions in CAP is restricted to psychopharmacological trials, barring a few done for psychosocial interventions. Also, as per a World Health Organization report, significant healthcare gaps exist for the provision of CAMH among the LMICs. 20
In spite of acknowledgment of the pressing need to develop preventive and promotive CAMH services, there exists an enormous discrepancy between the needs and resources. 21 This has been very well highlighted by the WHO Atlas project. 22 More than a decade later, vast differences exist for CAMH services across the HICs and LMICs. The barriers that undermine the provision of accessible and affordable CAMH services in LMICs can be discussed in the form of extrinsic or systemic barriers and intrinsic or patient-related factors. These will be discussed briefly herewith.
Extrinsic Barriers
Shortage of Human Resources and Capital Resources
The existing mental health resources, including CAMH, are limited in LMICs. As per the Atlas survey, the number of beds available for children and adolescents in LMICs is below 0.2/1,00,0000 population. 20 Additionally, there is a poor referral system and an over-burdening of the existing CAMH. The training of therapists to deliver psychological interventions has been a lengthy and expensive process that is often limited by a lack of trained faculty and financial support for developing such training services.17, 23 Further, the resource allocation and utilization for rural and urban population are not the same. Also, the inequitable distribution across the various socioeconomic groups, the lack of health insurance for a significant chunk of population, and out-of-pocket expenses for most of the population make CAMH services inaccessible.16, 19
Poor Access to Child Services
The critical issue for mental health is the pattern of how health services are being utilized by the population. Several factors, such as public awareness of mental health problems, misconceptions about mental illnesses among parents as well as health professionals, poor inter-sectoral coordination, and lack of CAMH services at the primary care level or school level act as barriers to accessing CAMH. Furthermore, the problem is not limited to only LMICs; even HICs face this problem, though to a slightly lesser extent than LMICs.24–26 Other barriers to accessing CAMH include the nature of the illness, median duration of mental illness, delay in seeking care from the time of onset, choice of providers, distance from the health center, and the number of visits to the service provider. It is estimated that <1% of children and adolescents suffering from mental disorders receive treatment.27–29 Moreover, there are several critical disorders, including learning, speech, visual, hearing, and personality disorders, that require multispecialty care that is not available and accessible even in urban areas. Additionally, scarcely highlighted special populations such as orphans, street children, juvenile homes, and rescue homes, where children and adolescents are exposed to a higher risk of mental illness, are seldom approached. 28
Lack of Policy, Political Will, and Community Response
Better progress of CAMH can be accomplished by understanding the hindrances to policy development and thereby the utilization of services. The biggest hurdle in this regard is lack of awareness and consequential social stigma for mental health. In general, community attitude toward mental illness significantly contributes to associated stigma, thereby leading to underreported and delayed reporting of mental disorders, which can lead to severe impairment if not addressed early. 29 From the system’s perspective, one of the most important barriers to developing CAMH policies and programs is the absence of mental health in the mainstream health policy. Although India has a mental health policy, the provisions of mental healthcare for children and adolescents are the least discussed in the policy documentation.30, 31 Moreover, only 0.06% of the total national health budget is allocated to mental health, which is even lower than the average mental health budget in other low-income countries. 32
Lack of Culturally Appropriate Tools/Therapies
Alongside the human and capital resource barriers to psychological interventions, another major limitation is lack of culturally appropriate interventions. Although most of the models of cognitive behavioral therapies evolved in the West, their application to LMICs has been questioned. 33 However, on the contrary, appropriate culturally and linguistically validated therapies developed in the West have been successfully adapted to LMIC settings. 34 With respect to culturally appropriate CAMH assessment tools and psychological interventions, some adaptations have been done across the LMICs, but still, these remain scarce.15, 34
Intrinsic Barriers
Lack of Awareness/Felt Need for Treatment
Children and adolescents are often dependent on their caregivers for their needs, and it has been shown that in view of poor mental health literacy among the CAP as well as their parents/caregivers, they may not perceive the problems and consequently seek appropriate intervention.21, 35–38 Further, certain abnormal behaviors in this developmental phase might be ignored as normal deviations by the parents/caregivers. The problems are further exaggerated in cases of separation from or loss of parents, family conflicts, or a history of mental illness in the caregiver themselves. 39 Other contributory factors include poor parental education, parental neglect, lack of awareness among the teachers, and poor sensitization for the recognition and management of mental health problems among various stakeholders, including health professionals. 37 So, the lack of adequate social support from the caregivers, peers, teachers, and significant others for the CAP may be a limiting factor in recognizing the mental health problems and seeking suitable treatment.
Lack of Resources and Access to Mental Health
A range of patient factors such as poverty, poor or difficult living conditions (such as exposure to wars/conflicts, other forms of violence, displacement, migration, political instability, a wide socioeconomic divide, etc.), homelessness, institutionalization, juvenile criminal activity, child marriage, child labor, out-of-pocket expenses, etc. may prohibit accessing mental health services in LMIC settings.21, 40, 41 As per the WHO Atlas report, the “out of pocket” expenses for availing CAMH services were 71.4% in African countries, in contrast to only 12.5% in European nations. 21 As per Indian data, there would be at least 20 million children and adolescents with a severe mental illness, and only 10% of them would have access to specialist mental health services. 42 Further, most of the CAP services are limited to tertiary care centers, which are mainly located in urban areas, and accessibility to such centers, which are mostly over-burdened, may be difficult. Additionally, in view of the limited services at these centers, psychological interventions might not be offered to a significant chunk of those in need in view of various systemic or patient-related factors.24, 42, 43 The situation is grim when one considers the provision of rehabilitation services for the CAP population in LMIC. Furthermore, the provision of disease-specific (e.g., borderline personality disorders) psychological services may be marred by a very few trained professionals. 44
Psychosocial Factors Influencing Help-seeking
It is a common experience of mental health professionals that adolescents often first approach parents for help. However, often, seeking help from parents becomes stigmatizing as their belief systems are shaken, along with another conundrum that mental ill-health is habitually perceived as personal failure, and as a result, informal help is considered more appropriate to avoid the shame associated with it. The associative disgrace demotivates the parents to seek support from the family, society, or mental health professionals. 35 Furthermore, this society-induced stigma is perceived in a different manner by children and adolescents when compared to adults in view of development of cognitive capacities.45, 46
There also exist cultural differences toward children and adolescents across countries. The CAP is often treated as a part of the respective family rather than a separate individual in a society, and therefore, society often relinquishes its duty to uphold the right to provide CAMH services to the family of a child/adolescent. 47 Further, emphasis is often laid on only physical health, and only schools are believed to be sufficient for a child’s development. Access to CAMH services is often limited to a select few, and only medical models of care are considered to be valid in the management of child and adolescent mental health problems. Moreover, such beliefs and perceptions percolate from the smallest unit of society, that is, family, up to policy makers and hence act as a barrier to the provision of CAMH.
Approaches to and Solutions for Access to Child Psychotherapy in LMICs and HICs
As outlined in the above sections, there are many barriers to accessing child psychotherapy in both higher resource and lower resource environments. Some of these (such as workforce and resource limitations, bureaucratic barriers, provider biases, and family health literacy and beliefs) exist in both settings.
Various potential solutions have been presented to improve access to children’s mental health services, particularly access to psychotherapy. The use of teleconsultation has been one of the positive outcomes of the COVID-19 pandemic, which has served to bridge geographic barriers and connect children and families in need with therapists in distant locations. This is largely happening using personal electronic devices such as cell phones, tablets, and personal computers using common web-based teleconsultation software. 48 The United States has seen a proliferation of web-based services delivering psychotherapy to children and families, at both regional and national levels. The application of technology has been used to improve access to psychotherapeutic services through the development of smartphone applications with algorithms that guide children and families through various skill-building cognitive and behavioral techniques to address both internalizing and externalizing symptoms. 48 Some of these are actively guided by psychotherapists, but some are autonomous and utilize feedback loops for the patient to identify mastery of such skills. There is beginning to be some experimentation around the use of artificial intelligence (AI) in providing psychotherapy, through either interaction with software or voice activation, using sophisticated algorithms based on manualized psychotherapy models. Algorithms have already existed for some time for voice-activated diagnostic interviews. This next step is only natural, may well help bridge much of the access gap, and could potentially be adapted for various cultural populations.10, 48
Some states have moved to fund access to psychotherapy services delivered by trainees in various mental health disciplines, though this has occurred primarily in more progressive areas of the United States. Another approach utilized by other states in the United States has been to train the existing workforce in evidence-based psychotherapies to effectively help children with more complex mental health needs, such as children in state custody (who often suffer from post-traumatic stress disorder), and children and youth with more serious internalizing behavioral disturbances that require more skilled psychotherapies such as trauma-focused cognitive behavioral therapy and dialectic behavioral therapy. 49 With regard to addressing culturally competent care, some states have begun to require continuing education in this area for licensure and re-licensure, though there is a need for much broader reform involving preservice education and training. 10 The latter has been hampered in recent years by some degree of conservative backlash to greater cultural diversity in many Western nations, including the United States.
The use of paraprofessionals in delivering child psychotherapy models has been advocated within both LMICs and high-income nations. The United Nations Children’s Fund has proposed this model as a means to improve access in LMICs, especially through school-based services. There has been much experience with approaches in post-conflict nations where there has been an acute need for therapists to address post-traumatic stress disorders in child victims and combatants, thus reducing the likelihood of the repetition of cycles of violence.50–52 Similar approaches have been advocated as a means to improve both access and cultural competence of psychotherapy interventions with minoritized populations in HICs. 10 The risk of this approach is that it may relegate minoritized populations in HICs and populations in LMICs to a “second class” level of services, discouraging the development of cultural translations of evidence-based approaches, though there is evidence that therapy effectiveness is independent of level of formal training.
Addressing stigma is still another area where barriers to access can be effectively addressed. Some nations have even used public information campaigns to urge their citizens to seek early services for children’s mental health conditions, such as the public education campaigns in Australia around early psychosis and the public education campaigns in the United States and other Western nations around youth suicide. These are often linked to “call in numbers” to provide access to crisis counseling and guidance to identify services. More robust campaigns are still needed to reduce the stigma of providing mental health services in public settings such as schools that are growing but still face community opposition. 8
A few articles have focused on targeted approaches for at-risk populations with lower levels of access. Hansen et al 53 performed a retrospective review of all referrals (n = 1825) for children (0–18) referred for assessment at the outpatient Child and Adolescent Mental Health Service of the North Denmark Region in 2021. They found that children in care (child welfare) were overrepresented in this clinical sample and had an increased risk [adjusted odds ratio (AOR) = 2.54] of having their referrals rejected by child and adolescent mental health services. Referrals from general practitioners were also associated with an increased risk of rejection (AOR = 3.29). Gopalan et al 54 updated a review of the literature on the engagement of families in child mental health treatment. They found that despite ongoing advances in evidence-based treatments and dissemination strategies, engaging families in mental health treatment remains a serious challenge. Within the past several years, a number of technological advances and interventions have emerged to address this problem, such as web-based communication with families as well as text-based appointment reminders. Interventions such as motivational enhancement, parent empowerment and activation, home-based therapy, and linking services to school success have also enhanced parent engagement. Families with children who present disruptive behavior challenges and symptoms of trauma are considered in terms of the unique barriers they experience regarding engagement in treatment, and interventions targeting these groups include parenting psychoeducation and training as well as collaborative care with community entities such as law enforcement.
In terms of using technology, telehealth has been examined further as a method for referrals. Coker et al 55 studied a telehealth-enhanced referral process in pediatric primary care from a multisite federally qualified health center (FQHC) and two community mental health centers using a cluster randomized methodology. They found that children using the telehealth-enabled referral process had three times the odds of completing the initial CMHC screening visit compared with children who were referred by using usual care procedures (80.49% vs. 64.04%; AOR 3.02; 95% confidence interval 1.47 to 6.220). Among children who completed the CMHC screening visit, intervention participants took 6.6 days longer to achieve it but also reported greater satisfaction with the referral system compared with controls. Once this initial access point in referral was completed, 80% of eligible intervention and control participants (174 of 213) went on to an MH visit.
Parental and family factors have also been the focus of some approaches. For example, Haine-Schlagel and Walsh 6 conducted a study of the literature on parent participation and engagement in child psychotherapy. They found evidence of links between parent participation/engagement and outcome improvements across some outcome domains. Strategies designed to target parent participation/engagement were found to be effective overall in improving parent participation and engagement.
Improving Access and Engagement with Therapeutic Referrals: The Case of Collaborative Care
Referrals from primary care have drawn increased attention given the increasing involvement of this sector in child mental health services. For example, Cloutier et al 56 reported a survey to assess physicians’ attitudes and knowledge of mental health services and centralized intake services for mental health within the Children’s Hospital of Eastern Ontario (CHEO) and the Royal Ottawa Mental Health Centre (ROMHC). Of 735 eligible physicians, 388 completed and returned the survey (52.8% response rate). The majority of physicians were aware of mental health services offered by their hospital. Physicians reported lower confidence levels when delivering counseling and psychopharmacological treatments for mental health. Furthermore, over 72% indicated that they did not feel they had time in practice to provide mental health counseling. Over 65% of physicians reported that mental health referrals should have appropriate/defined criteria. The majority (92%) of physicians had referred to specialized mental health services provided by their hospital. With respect to centralized intake services, 57.2% of physicians indicated they were aware of the service, and 73.9% said it should be continued. However, only 34% reported satisfaction with the centralized intake referral service. Auxier et al, 57 examining integrated behavioral healthcare and referral success with adults, reported on results of a multisite card study organized by the Collaborative Care Research Network, a subnetwork of the American Academy of Family Physicians’ National Research Network devoted to conducting practice-based research focused on the provision of behavioral health and health behavior services within primary care practices. Of the 200 patients referred to a behavioral health program, 81% had an initial contact, 71% of which occurred on the same day. Men and women were equally likely to engage with a BHP, although the time between appointments varied by gender. Depression and anxiety were the primary reasons for referral.
Given the above-reported success in integrated behavioral health in improving the success of referrals for behavioral health services, a group in an academic behavioral health collaborative program (AJP, KB, KT) decided to pursue a focused quality improvement project focusing on referrals of children and youth for psychotherapy and other related services. This regional behavioral health collaborative program serves primarily rural underserved children seen within their pediatric practices. It provides telephonic and televideo consultative services to primary care pediatric providers, especially around diagnostic assessment, pharmacotherapy, and treatment planning. As part of this consultation, the program provides case management with referral assistance and support, primarily for psychotherapy as well as other therapeutic services. The case management approach is highly individualized, with our case manager making direct outreach to families and using motivational techniques to engage them in following up with referrals when needed as well as assisting with administrative logistics. We also collaborate with the primary care provider in supporting referral follow-through.
To evaluate the effectiveness of our case management services, we analyzed data from consultative referrals over a series of 104 patients during the first half of a calendar year. We reached out to families from three to nine months since last contact to evaluate follow-through with therapy or other therapeutic services they were referred to. We evaluated follow-through and engagement along demographic (age, gender, race, and/ethnicity) and diagnostic categories.
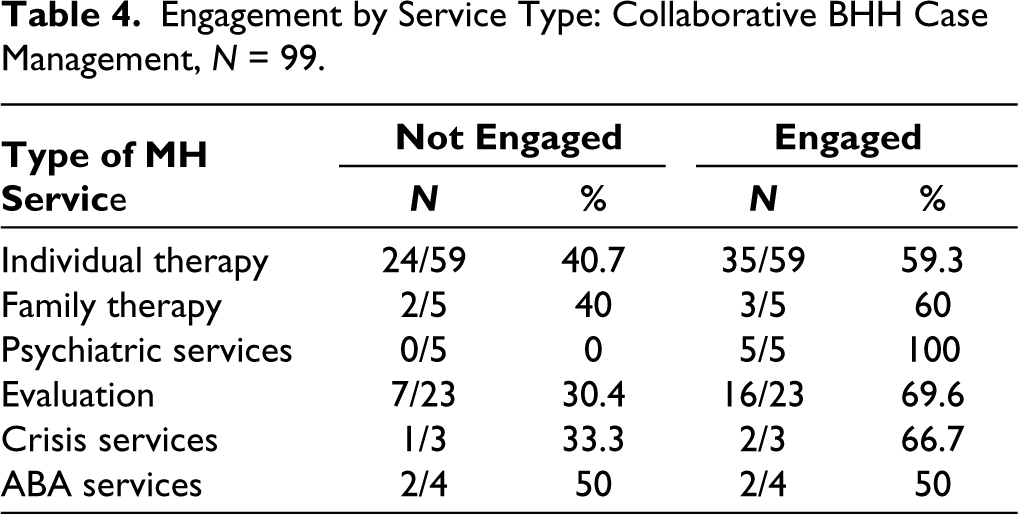
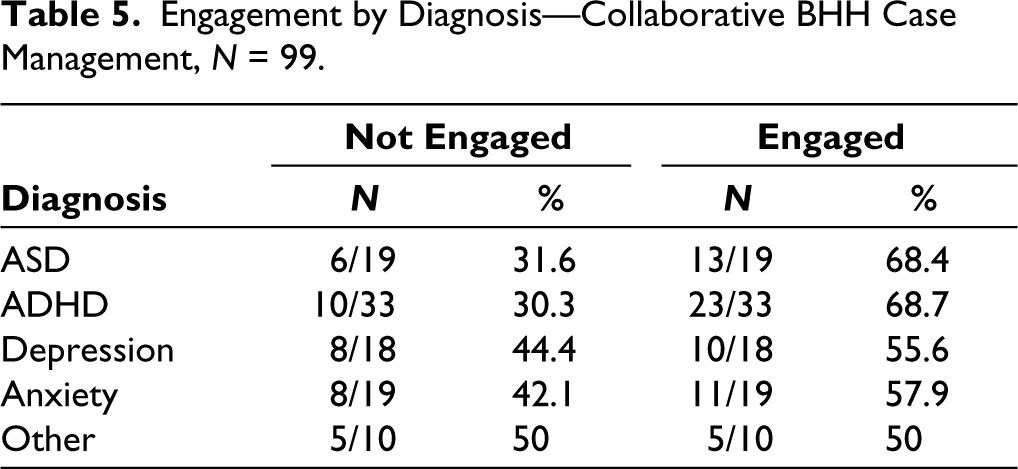
We found that our overall referral success (engagement in the service three to nine months after the consultation) was overall at 64.4%. The highest referral engagement occurred in elementary school-age children, followed by teens, and the lowest in preschoolers (Table 1), about equivalent in gender (slightly higher in females; Table 2). We had a higher level of engagement in minority groups (Black and Hispanic youth and families) than White families (Table 3), which reflected our case manager’s emphasis on cultural competence and acceptability. Among different types of services, we found the highest referral engagement for evaluations, crisis services, and individual therapy in that order, with an engagement rate of 59.33% for psychotherapy referrals (Table 4). Across diagnostic groups, we found the highest engagement rates among families of children with AD and ADHD, less so with internalizing disorders (depression and anxiety; Table 5), suggesting that externalizing disorders may motivate families to follow through more with services even though they may be at least as difficult or more difficult to engage with.
Engagement in Treatment: By Age.

Engagement in Treatment: By Gender.

Engagement in Treatment: By Race/Ethnicity.

Engagement by Service Type: Collaborative BHH Case Management, N = 99.
Engagement by Diagnosis—Collaborative BHH Case Management, N = 99.
Conclusions
This article has provided a comprehensive summary and comparison of the barriers to care for child mental health that exist between the populations of high-income and low-income nations.
In essence, these findings highlight how these barriers to care are directly related to Maslow’s “Hierarchy of Needs” 58 and how each human being should be understood and treated as a unique individual, with a very particular temperament and responding to a unique set of cultural and socioeconomic circumstances, and that the goal of designing “one size fits all” treatment interventions is a total fallacy.
Treatment interventions should be tailored to the particular needs of the child and their family, taking into account the particular socioeconomic and cultural circumstances inherent in each child and family and also taking into account the socioeconomic and cultural circumstances inherent in the part of the world in which they (the child and the family) live. So, designing successful access to future treatment interventions for child mental health should focus, first and foremost, on the child and the family’s socioeconomic and cultural realities and those of the part of the world in which they live.
This article also presents not only a qualitative context but also approaches that address the unique needs found in different parts of the globe and also within so-called HICs. At the same time, it also presents the potential for quantitative approaches that can complement qualitative ones and result in greater accountability for addressing service disparities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.