
Abstract
Background:
Lifelong intervention is the mainstay of rehabilitation for individuals on the autism spectrum. The Lancet Commission on care and clinical research on autism has noted the prohibitive cost of intervention services in Low Middle Income Countries and has recommended active involvement of parents in the intervention process. However, there appear to be limited resources for parents to train themselves. The purpose of this qualitative study was to understand the state of Parent Mediated Interventions across India.
Method:
The study was carried out in two phases. In the first phase, professionals from centers across India were interviewed to understand the methods followed in their centers. In the second phase, focus group discussions were conducted with parents of children on the autism spectrum to understand their needs and challenges in working with their children.
The findings from these two phases were then presented to an experienced professionals to corroborate the results.
Results:
Parent-mediated interventions were found to be limited and relying on manuals published in the West. Parents of children above the age of six continued to face challenges in teaching communication and managing difficult behaviors.
Conclusion:
Empowering parents by educating them right from the time of diagnosis of the child will ensure better adult outcomes among individuals with autism spectrum disorders.
Introduction
Autism spectrum disorder is a developmental disorder that results in impairments in social communication and interaction along with restricted thinking. 1 The prevalence according to the latest estimates by the Centre for Disease Control (CDC) is 1 in 54 2 with data from India being somewhat lower. Early, intensive intervention is considered to be the mainstay in rehabilitation measures. Mahajan and Sagar 3 have spoken about the lacunae in field of autism at all levels right from education of professionals and delivery of services. This results in many children falling through the gaps and not receiving timely diagnosis and intervention.
The active participation of parents in the intervention process of children with autism by acting as co-therapists is cited as one best practice in intervention. 4 This allows for improving the intensity of intervention and ensures that intervention proceeds through the waking hours of the child. This also enhances acceptance of the child leading to a better quality of life for the family.
Parent-mediated interventions (PMI) are interventions where there is active involvement of the parent and are generally technique focused. The parents are imparted education about the child’s disorder and the child becomes the indirect beneficiary. These PMI may be primary—where the intervention is carried out primarily by the parent or secondary—where the parents act as co-therapists along with a professional therapist.
PMI can target communication skills, 5 or they can complement center-based therapy. 6 Some PMI target specific maladaptive behaviors (e.g., food refusal 7 ; sleep disturbance 8 ).
The Lancet Commission on care and clinical research in autism 9 noted the prohibitive cost of intervention in low and middle income countries (LMIC) and emphasized the need for moving toward PMI.
Some Indian centers have worked with PMI. Manohar et al. 10 studied the acceptability and feasibility of a brief PMI in a Randomized Controlled Trial (RCT) in resource-limited settings. The emphasis of their study was to address parental stress from a sociocultural perspective. Parents in the intervention group reported less stress than those in the control group at the end of 12 weeks. The program had a high retention rate with attrition of just 6% indicating its effectiveness.
Action for Autism (New Delhi) runs a 3-month Parent-Child Training Program (PCTP), which aims at empowering parents, encouraging acceptance of the child, and decreasing parental stress. 11 They carried out a study using an open-ended narrative method. In total, 40 sets of parents were asked to submit a 5-minute speech sample describing their child with autism, before and after attending the program. After PCTP parents were less likely to compare their children to a desired “normal” and were more accepting of their children.
Another study of PMI was carried out across 2 cities in South Asia—Goa, India and Rawalpindi, Pakistan. 12 In this study, a UK-based PMI called Preschool Autism Communication Trial (PACT) was adapted and called PMI for autism spectrum disorder in South Asia (PASS). In total, 65 children in the 2 cities were randomly assigned to 2 groups and followed up over 12 sessions for 6 months. The PASS group showed better parental synchrony and initiation of communication by the children. However, mutual shared attention reduced in the PASS group which could possibly be a reflection of parenting style and cultural differences. Another difference in the 2 is that PACT was delivered by trained speech therapists while PASS was delivered by nonspecialist health workers.
Srinath and Jacob 13 in their commentary of PMI have noted that teaching mutual shared attention (the ability of 2 individuals sharing focus on an object) appears to be more difficult. They also note the importance of exploring cultural beliefs related to special children in the family. They stress the need to educate parents about the disorder thereby enabling better acceptance of the child.
One review 14 on PMI in India found the number of papers (13 based on their inclusion criteria) on PMI to be limited in India. Of the papers included in the review, most (61%) of them focused children below 6 years of age. The average duration of the programs was around 12 weeks. They found only 1 center offering training to parents regardless of the age of the child and 3 programs extended the training till the child was 9 years old. The programs were mostly based on manuals developed in the West.
The Communication DEALL Family mediated intervention program 15 and the Upanayan 16 were 2 manualized PMI programs that we could find in our internet search, and both focused on very young children.
To understand more about the current status of PMI in India, we undertook a qualitative research study. We also wanted to understand the concerns and challenges faced by parents once the child was past the early intervention stage.
Methodology
The study was undertaken after obtaining the necessary approval of the Institutional Ethics Committee. The study was a mixed-method study carried out in 2 phases:
Phase 1: To understand parent training and PMI from the perspective of professionals and Phase 2: To obtain the parental perspective regarding services available for children beyond the early intervention stage.
Phase 1
In the first phase, we reached out to centers across the country. In all, we approached 20 centers, and professionals from 15 centers consented to be interviewed. These centers were based in New Delhi, Mumbai, Goa, Patna, Kolkata, Coimbatore, Jabalpur, Dehradun, and Bangalore. In-depth interviews were carried out with all the consenting professionals (n = 16). These interviews were carried out online on Microsoft Teams. The interviews were semi-structured with open-ended questions.
Phase 2
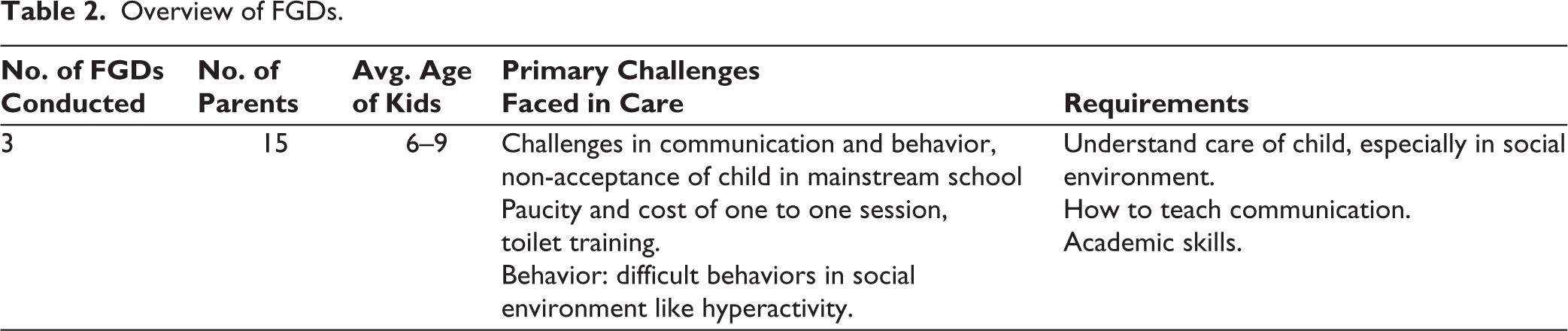
Focus group discussions were held with parents of children on the autism spectrum. We held 3 FGDs with a total of 15 parents. All the parents had children with ASD in the age range of 6 to 9 years. Some participating parents were contacted through professionals who were part of phase 1. Others were recruited through the initial consenting parents (snowball method). All were educated, urban parents. The parents all had children who had been receiving intervention for a minimum of 2 to 3 years. Parents of children in early intervention program were not included. Daley 17 had reported that children can be diagnosed as late as 6 years of age and hence our cutoff age for early years was chosen as 6.
The interviews and FGDs were conducted online via Microsoft Teams. They were recorded and later transcribed. The transcriptions were coded and analyzed with the help of the Dedoose software. The FGDs were moderated by the early intervention specialists. All of them had postgraduate qualifications in their respective fields (1 physiotherapist, 1 psychologist, and 1 speech and language therapist).
Results
Professional Interviews
The professionals interviewed were all running prominent private centers across India. The centers chosen were those that had been providing services for a minimum period of 3 years. Of the 16 professionals interviewed, only 6 were conducting structured PMI programs. In total, 2 of these were from the same center, where one was conducting the World Health Organization’s caregiver program while the other was conducting a PMI based on a manual developed in the West.
Three other centers were also conducting structured PMI programs based on manuals developed in the West. Only 2 centers were conducting PMI programs based on indigenously developed models.
One of the indigenously developed models of PMI focused primarily on young children on the autism spectrum. This model had been manualized.
The second indigenously developed PMI has not been manualized. They worked with families for an average duration of 3 months. They do not have an age restriction and accepted parents with children of all ages. The program involved daily sessions at the center and was called the Mother-Child Program.
The primary focus of the intervention in centers across the country was the early years group. Interventions after this took place in special schools. In the metros, there were schools that were autism focused while in some of the 2-tier cities, the schools catered to children of all disabilities. PMI was more incidental rather than the prime focus. They did not have specific goals for the PMI. The centers also did not have formal parent support groups.
The duration of the PMI ranged from 6 sessions to around 3 months. Except for 2 centers, all of them focused on children below the age of 6. There was 1 center catering to children up to the age of 9 while 1 did not have any age restrictions.
The qualifications of professionals imparting the PMI was varied. All were graduates with some postgraduates in psychology. Some had additional RCI-recognized diplomas in ASD.
Most of the centers did not use structured assessment tools to monitor the efficacy of their PMI. They relied primarily on parental anecdotal reports. Some centers used the Vineland Adaptive Behavior Scales (VABS) to monitor the child’s progress.
The centers in the major metros were all catering primarily to children on the autism spectrum while in the other cities, they were catering to multiple disabilities.
The centers across all cities focused on psycho-education for their professional-led intervention. Some special schools had added inputs from Speech and Language and Occupational therapists, but the work was predominantly carried out by Special Educators.
A total number of 16 professionals were interviewed, and we found that 4 Western models of intervention were used while 2 were indigenously developed models. The rest did not rely on any specific manuals or models and were more eclectic (see Table 1).
Overview of PMI Programs in Various Centers.

Focus Group Discussions
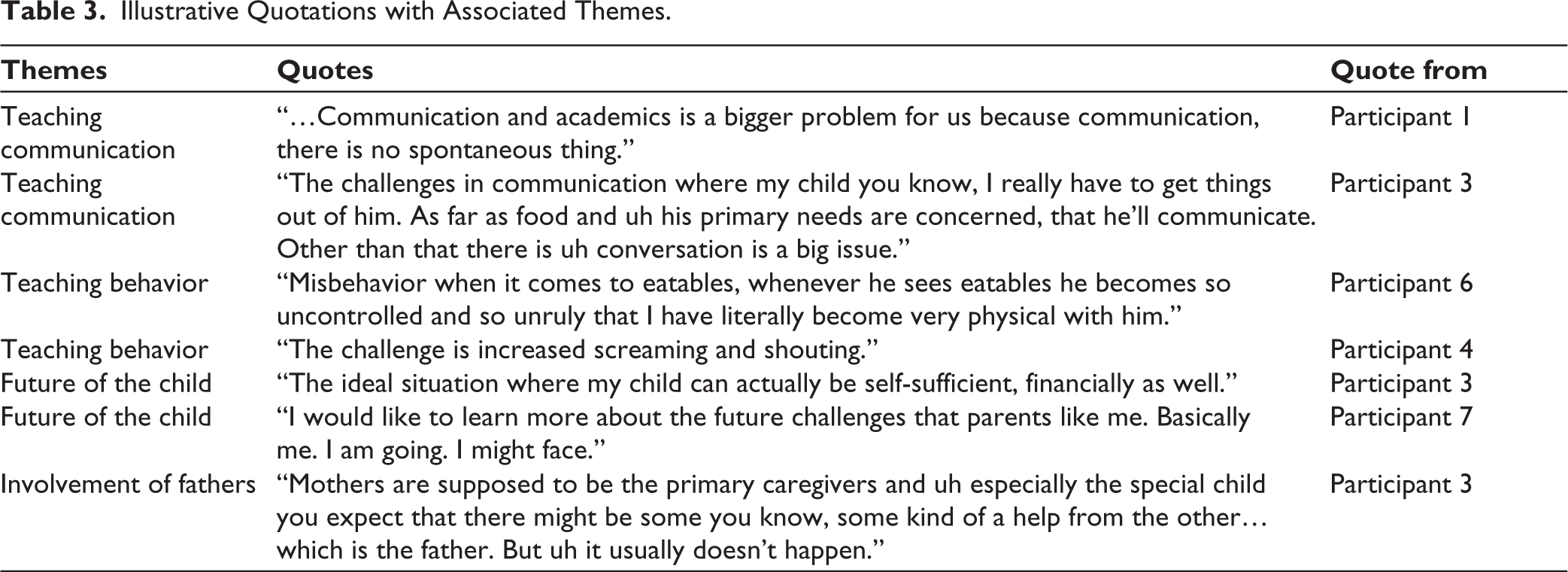
Three FGDs were held with parents having children in the age group of 6 to 9 years. Several themes could be identified as occurring repeatedly across all parents.
Teaching: Continued challenges in teaching their children in all aspects—communication, self-help skills, and managing challenging behaviors
Paucity of centers: Several parents reported difficulties in finding centers willing to work with their children.
Mainstream schools: Mainstream schools willing to accept children with special needs are limited and most of restricted to some of the bigger cities in India. Special schools are often catering to children with different challenges including those with intellectual impairments.
Future of the child: Several parents reported concerns for the future of the child, “…how to plan his future? A future existence also matters, because a big question is there is nobody after me for him.” This concern was amplified in those parents whose children were yet to achieve independence in communication and self-care.
Involvement of fathers: A few mothers pointed out that the onus of the care for the child, fell to them and fathers were largely uninvolved, leading to added stress on the mothers as they essentially acted as single parents (see Tables 2 and 3).
Overview of FGDs.
Illustrative Quotations with Associated Themes.
Expert Validation
To further corroborate our results, we conducted another in-depth interview with an experienced professional in the field. Her impressions were similar to our findings. She agreed that PMI in a structured format is limited across India. Parents continue to face challenges in teaching communication and daily living skills while they tend to hyperfocus on the academic skills.
The shift from early intervention to intervention at ages beyond 6 appears to be still in the nascent stages. Many parents flounder in mainstream schools and return to the special school fold somewhere along the way. This often results in a lack of continuity in their intervention, which leads to a lack of a strong foundation in prevocational skills. Training parents in understanding the need for continued support for the child’s development will ensure that the long-term outcome of the child will improve.
Discussion
While the Lancet Commission 9 recommends increased parent training in LMIC due to the prohibitive cost of intervention and the dearth of therapists, we found that parent training in India is still very much in the nascent stage. A few centers in the metros offered parent training/PMI. However, of these few, only 2 had indigenously developed models. Of these 2, only 1 had been manualized and this focused on toddlers. There were no handy resources for children beyond the early intervention stage and parents were left to navigate this uncharted territory on their own.
Many parents hyper focused on academics to the detriment of life skills development. The effect of this lack of continuity in interventional support is evident from the case series reported by Mamtani et al. 18 Teenagers and young adults spent time in unstructured routines with increasing behavior challenges that resulted in being a barrier to later vocational rehabilitation. Poor parental knowledge and attitude further contributed to this barrier. In addition to this, there was a resistance toward vocational rehabilitation by both the parents and the individuals. This could be on account of the stigma attached to the disorder itself and poor community awareness and acceptance.
This lack of knowledge in parents and difficulty in managing their children often results in increased stress among parents. Daley et al. 19 found that 70% of their sample had higher levels of stress when compared to those reported from outside India. 41% of their sample reported that the children were at home, either because of the parent’s inability to manage their behaviors to take them to structured day centers or because of limited centers offering services. Parent training to teach independence in activities of daily living and in the management of challenging behaviors is necessary to help reduce parental stress which has been seen in studies of PMI.10,11
It is evident that there is a need for continued interventional support for children with ASD as they move out of early intervention. This unmet service can be improved by bringing about an attitudinal change among parents with increased parental involvement and education. This will help improve adult outcomes.
Srinath and Jacob 13 rightly pointed out that parent training in the Indian context needs to be both supportive and educative. It is through proper parent education that we can hope to bring about better acceptance and better decision-making among the parents. The gaps between early intervention and eventual adult outcomes can only be ameliorated by well-informed parents. It would be beneficial to start this parent education process right from the time of diagnosis. Empowering the parent with counseling sessions, offering them appropriate reading material and encouraging them to join parent support groups will go a long way toward enabling the parent to make informed decisions.
PMI in India are still very much in the nascent stage despite the prohibitive cost of specialist interventions. Well-informed parents will ensure better adult outcomes among individuals with autism spectrum disorders.
• Parents of children with autism continue to face challenges in teaching communication and behavior beyond the early intervention stage.
• Mothers are often left to deal with these challenges with little support from their spouses.
• Parent education from the time of diagnosis will be beneficial to the families and long-term outcome of the child.
Footnotes
Declarations of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was carried out after obtaining the necessary approval from the Institutional Ethics Committee of St. John’s Medical College, Bangalore. IEC Code No: 163/2021 dated 04.06.2021. The study was carried out in accordance with the principles enunciated in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Verbal informed consent was taken from all participants at the start of the interview/FGD which was recorded.