
Abstract
Background:
Academic anxiety revolves around scholastic work and performance and can be detrimental to students’ health and overall subjective well-being. It has been found to be significantly high in adolescents, leading to consequences that prove to be detrimental to their academic performance, focus, and overall self-esteem. This phenomenon acts as a vicious cycle impacting all aspects of a student’s life.
Method:
The current study aimed to explore mindfulness-based intervention (MBI) as a possible option to deal with academic anxiety in rural adolescent students and improve their overall subjective well-being. A total of 600 students were screened for academic anxiety and a total of 47 students were subjected to an eight-week MBI. MBI aims to bring more present-moment awareness and cultivate overall well-being and thereby works against anxiety. Mixed repeated measures ANOVA was carried out to compare pre, post, and follow-up scores.
Result:
The results indicated a significant effect of MBI on adolescents, suggesting a significant decline in academic anxiety from pre-to-post and an increase in mindfulness and subjective well-being from pre-to-post and follow-up assessments.
Conclusion:
Academic anxiety and subjective well-being improved significantly with the MBI intervention, thereby implication that MBI is a feasible option for rural adolescents with academic anxiety.
Introduction
Poor performance, academic prognosis, and transition to change could often lead to academic anxiety, lack of motivation, and self-esteem among adolescents interfering with their overall performance.1 Parental involvement in academics of adolescents also plays an important role. Academic anxiety is generally defined as being situation-specific and stemming from fear, nervousness, and apprehension. 2
Adolescence can be best understood as a stretch between adulthood and childhood and is marked by changes and growth in biological, social, and psychological aspects of life. 3 Studies on a range of culturally and geographically dense populations report a sharp prevalence of academic anxiety ranging from 16.1% in the United States to 19.6% in Saudi Arabia, with other Asian countries following behind. 4 In India specifically, around 14%–20% of adolescents experience academic anxiety and around 45.5% report high academic stress. Academic anxiety has been found to negatively correlate with subjective well-being. The concept of well-being can be characterized from various perspectives, including subjective well-being and psychological well-being. This phenomenon encompasses positive and negative effects as well as life satisfaction. Hence academic anxiety can manifest itself due to excessive parental involvement, peer competition, and personal factors in the form of lack of motivation, concentration, or poor academic performance. 5
Intervention options for academic anxiety can include certain relaxation techniques, stress management as well and cognitive behavioral therapy, which has been found to be influential in reducing symptoms of academic anxiety. 6 Further, assertiveness training can counter academic anxiety by inculcating decisiveness and building a resource against anxiety.
Mindfulness-based interventions (MBI) counter stress and anxiety while establishing focus and moment-to-moment awareness.7, 8 It is the treatment of choice when searching for an effective preventative technique and a method to develop the ability to handle academic anxiety.9, 10 Research suggests an effective role of MBIs for clinical and non-clinical populations of all age groups for reducing psychological discomfort. 11 With regards to the adolescent population though MBI is effective the available data is mostly from urban school-going adolescents. This, however, remains largely unexplored in the Indian rural context, and very little effort is made to alleviate this psychological issue of rural adolescents while the magnitude of the problem remains almost equal in both populations. A few studies report indirectly a similar pattern of positive effect of MBI on rural adolescents.12, 13 Taking into account these factors the current study aimed to understand the applicability and effectiveness of MBI on academic anxiety and overall subjective well-being in the rural adolescent with academic anxiety through an eight-week intervention program.
Material and Methods
Participants
The sample size estimation was calculated based on previous research of Khesmakhi et al. (2019) and with the help of G power software which on the reported effect size 0.25 with power (1 – β) set at 0.80 and with a 95% of confidence interval suggested approximately 42 participants in each group.
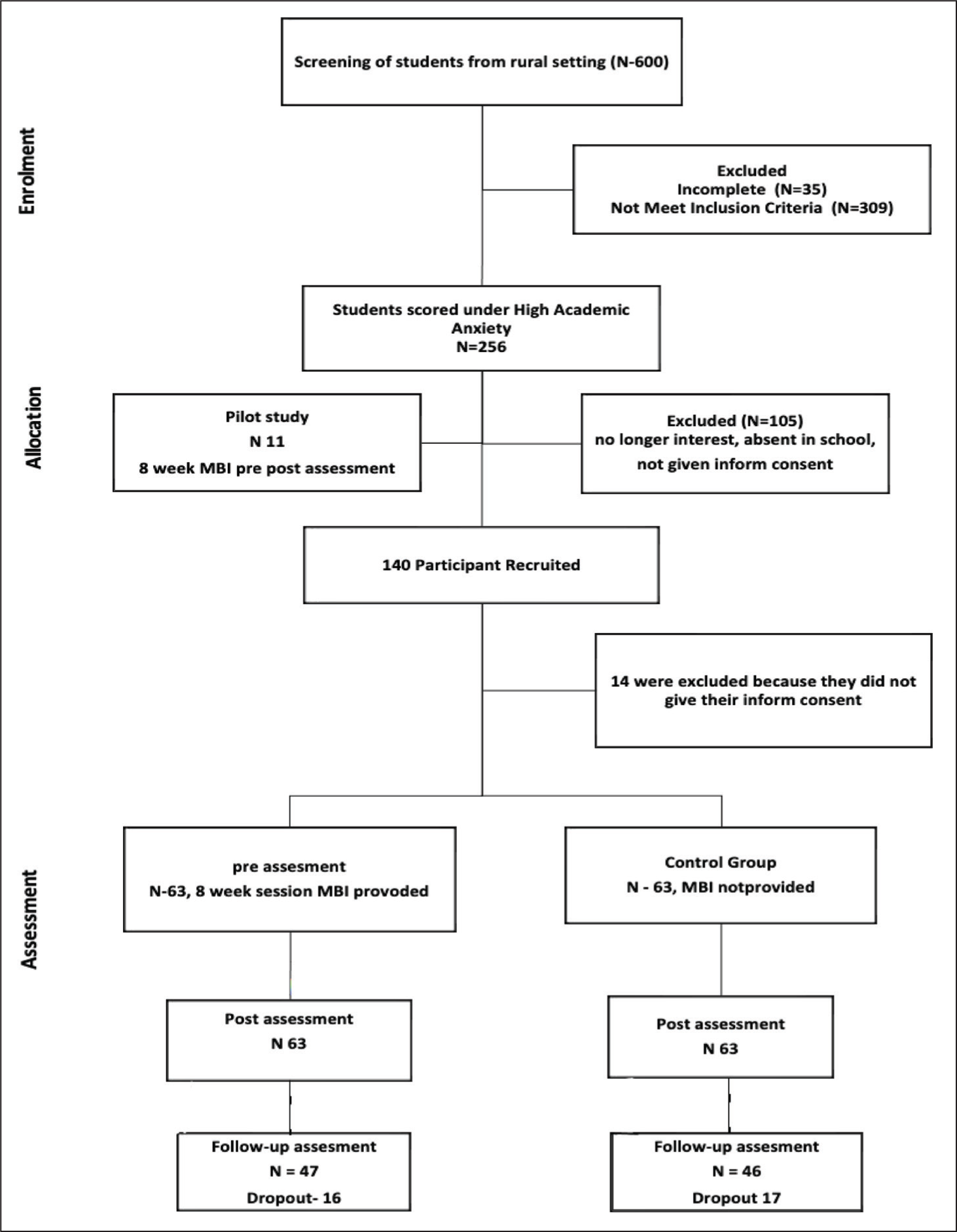
On the basis of sample estimation, 600 adolescents were recruited from the Akbarpur district of Uttar Pradesh in a rural school setting. Screening tools like the General Health Questionnaire (GHQ), 14 Brief Psychiatric Rating Scale for Children, 15 and the Academic Anxiety Scale (AAS; Singh & Gupta, 2008) 16 were used. Expecting a 20% drop in our rate in the therapeutical intervention 126 students, aged 12–17, were selected, with 63 in each intervention and control group, using the lottery method of simple random sampling. A total of 47 participants completed the mindfulness training to the follow-up and 46 completed all three assessments in the control group.
The study participants were male and female adolescents with academic anxiety who were enrolled in a school in a rural setting. Participants with severe medical, neurological, intellectual, or mental conditions, as well as those who did not meet the cut-off for the screening instrument, were excluded and referred to mental health professionals.
Scales
Socio-demographic Datasheet
It is a self-developed semi-structured proforma that combines socio-demographic information with a clinical case narrative format. It has been verified by an expert. It facilitated in the collection of socio-demographic data as well as screening based on exclusion and inclusion.
General Health Questionnaire 14
Goldberg, a British research scholar, developed this comprehensive health-related screening tool in 1972. 17 This has been translated into many different languages, including Hindi. The GHQ-12, a 12-item questionnaire, is used in primary care to assess patients for general (non-psychotic) mental health concerns. This is a self-report rating scale with a cutoff of three, indicating psychological discomfort. The GHQ-12 has a high sensitivity, 18 specificity, 18 and reliability. 19
Brief Psychiatry Rating Scale for Children 15
The existence and severity of nine psychopathologies can be evaluated using this scale, which was developed in 1982 by Overall and Pfefferbaum. The screening tool with a seven-point rating ranging from “not present” to “very severe” 20 can detect children’s behavioral and psychological problems. 21 The newly redesigned and anchored BPRS-C outperforms the old instrument in terms of internal consistency and interrater reliability (Cronbach’s alpha = 0.83).
Warwick–Edinburgh Mental Well-being Scale (WEMWBS) 22
Grover and Dua adapted the scale for use in the Indian context in 2021. 22 It consists of 14 items, including subjective and psychological well-being based on the past two weeks of experience. The scale ranges from one to five, with one indicating never and five indicating always. Cronbach’s alpha is 0.923, which indicates a high level of internal consistency. The test-retest reliability is 0.99.
Academic Anxiety Scale 16
Singh and Gupta designed the AAS in 2008 for use with students in grades seven through 10 (age range: 13–16 years). The initial version of the AAS for children consists of 30 elements. Each test item is assigned a score of +1 or 0; there are two categories of questions: positive and negative. A high test score indicates high academic anxiety, whereas a low test score indicates low academic anxiety. The validity is 0.57 and the reliability is 0.75.
Child and Adolescent Mindfulness Measure (CAMM) 23
The CAMM, 23 developed by Greco et al. (2011), is the first mindfulness test made exclusively to evaluate the mindful disposition in children and adolescents between the ages of 10 and 17. The 25-item CAMM has three components: observation, paying attention to bodily sensations, and avoiding emotions. The CAMM showed adequate convergent and divergent validity as well as good internal consistency (=0.80) in an early validation investigation. 24
Procedure
This study has been approved by the Institutional Ethical Clearance Committee (IRB Approval: CU: RCEC/00297/06/22) after assessing all the ethical aspects. Approval from the research ethics committee of the university as well as consent from the concerned school authorities were obtained before the study project. Screening involved 600 adolescents (12–17 years old) using the GHQ, BPRS-C, and AASC. Selected students and parents were informed about the study and obtained informed consent. Initially, the pilot study was carried out to determine the feasibility and ease of understanding of the intervention. The results showed significant declines in academic anxiety and improvements in subjective well-being and mindfulness. The pilot study yielded increased motivation and assurance for the subsequent main study, demonstrating comparable findings. Later on, further samples were divided into two groups, and the participants were administered CAMM and WEMWBS to establish a baseline for the main study. The intervention group participated in an eight-week MBI program with sessions (group sessions) lasting 45–60 minutes. Completion of intervention required attending at least five sessions. Post-intervention evaluation occurred a week after the program, followed by a one-month follow-up evaluation.
Intervention
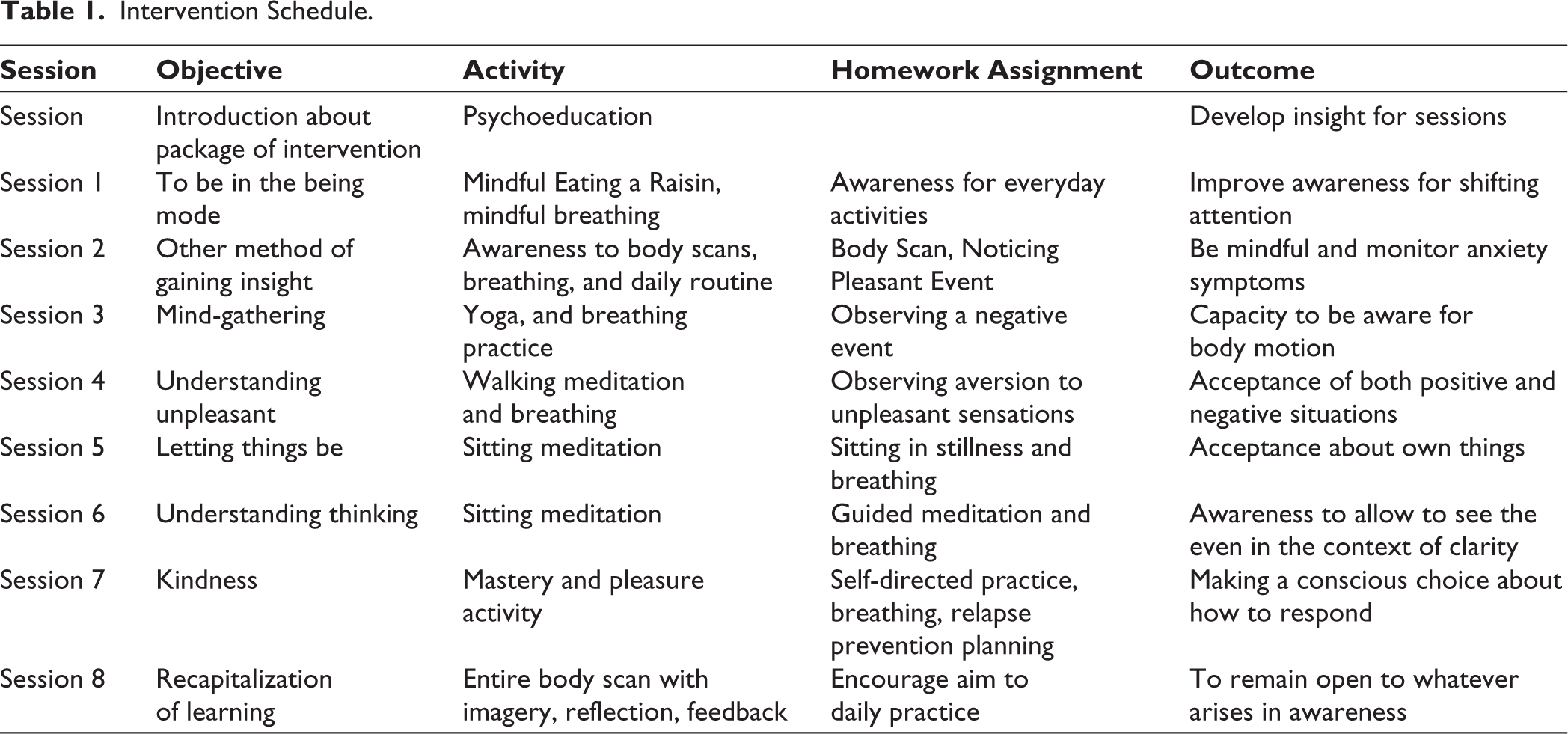
The intervention program was adapted from MBCT (mindfulness-based cognitive therapy) developed by Teasdale et al. (2002). The program spanned across eight weeks and was guided by a trained and licensed clinical psychologist (Table 1). The aim was to apply MBI as a short-term intervention to understand its effect on academic anxiety. Before the administration of the intervention schedule, it was expert validated by professionals in the clinical field for the suitability of content for adolescents in Indian. Since the subjects were from a rural background, the intervention was administered using both English and Hindi language. An intervention plan was implemented within a group including six to eight participants, as this approach was determined to have a more significant effect. Each session lasted an hour to an hour and a half and included homework, insightful comments, and both educational and practical parts.
Intervention Schedule.
Data Analysis
SPSS 28 was used to analyze the data set. The data set was put in order and was subjected to data cleaning to deal with the missing entries. The socio-demographics and data from the clinical interview schedule were subjected to further analysis to understand the mean and standard deviations. The entire data set was then tested for normality. Later, mixed repeated measures ANOVA was carried out to compare pre, post, and follow-up scores.
Results
Ninety-three students (mean age = 15.06, SD = 1.5) were a part of this study, with 46 students in the control group and 47 students in the intervention group. Figures 1–3 depict the graphical representation of the effect of time on subjective well-being, academic anxiety, and mindfulness, respectively.
Study Design Flow Chart.
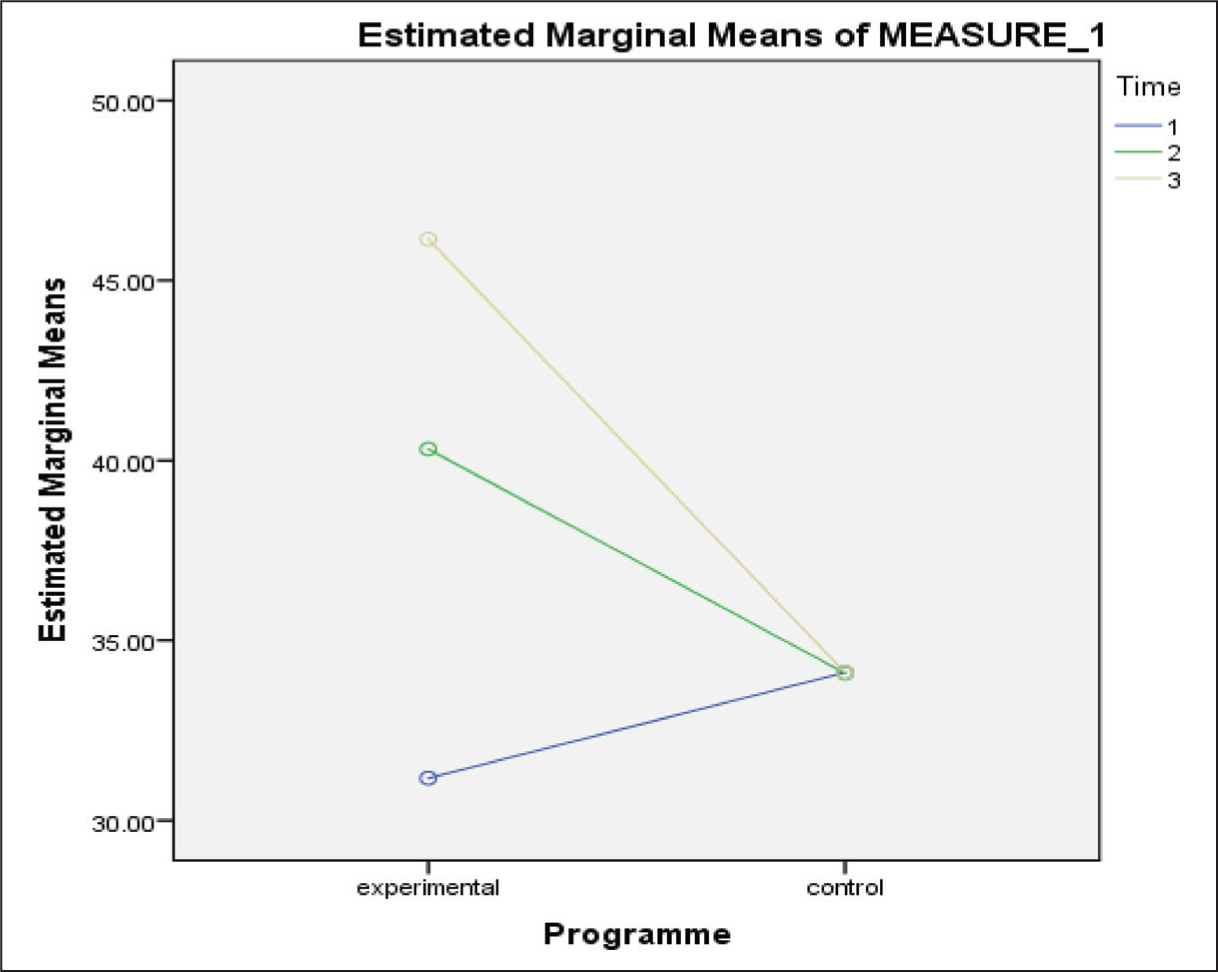
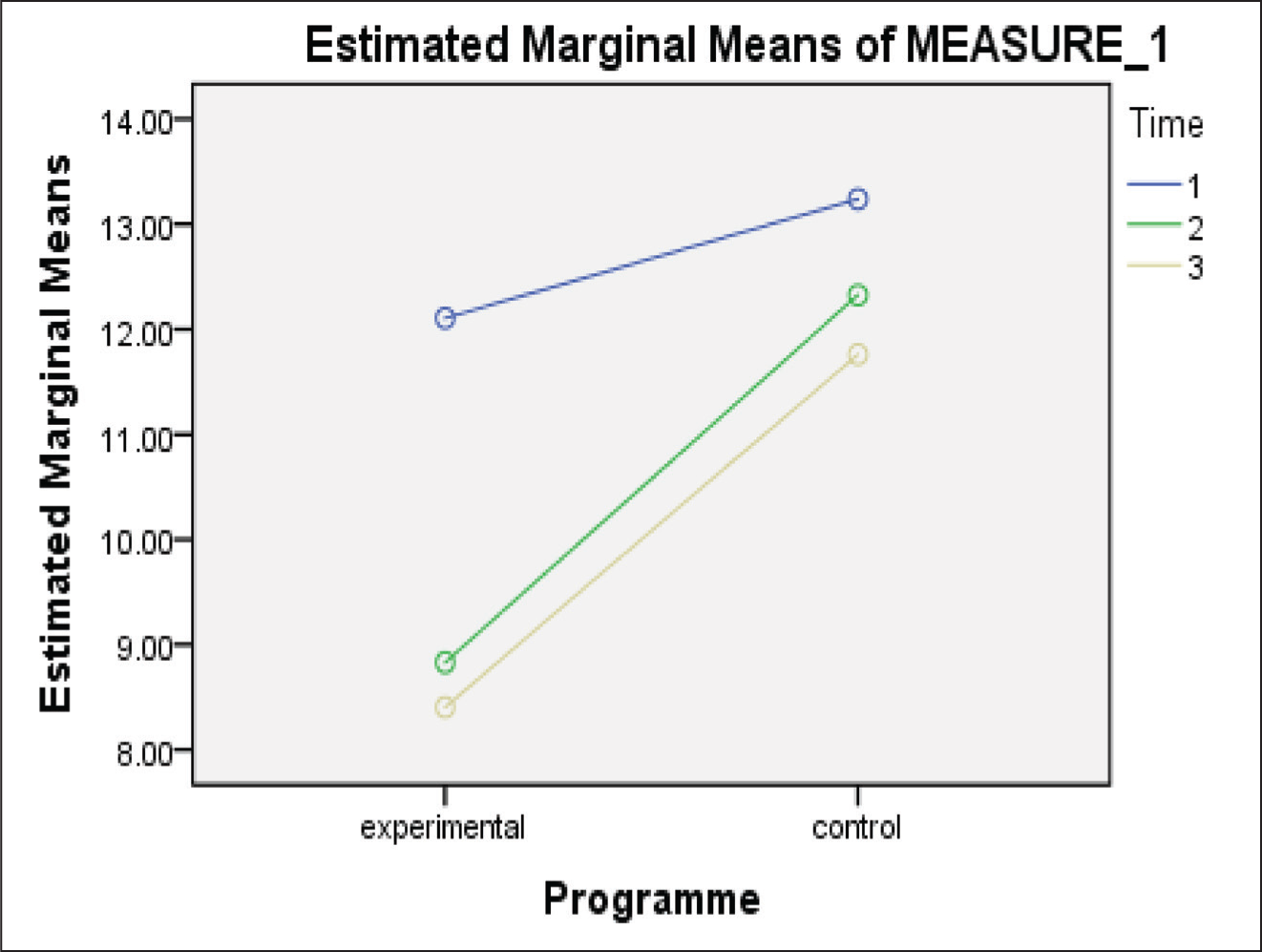
In the three graphs above, the result shows the comparison of experimental and control groups of all variables across three time points, where one indicates the pre-assessment, two is the post-assessment, and three stands for the follow-up assessment phase. Figures 2 and 4 show a stark increase in the overall level of subjective well-being and mindfulness capacity from the pre-to-post and follow-up assessment phases in the experimental group as compared to the control group.
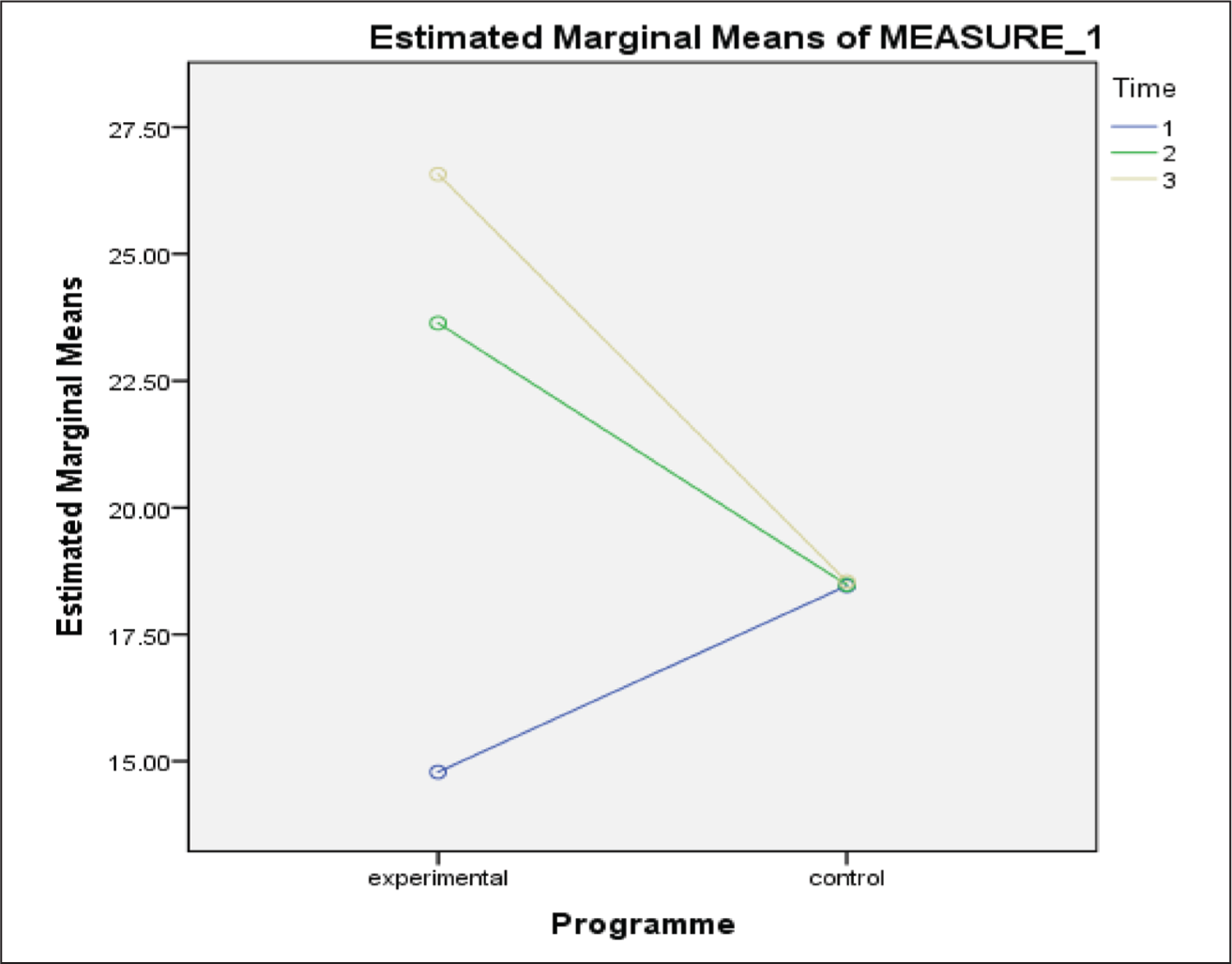
Figure 3 indicates a significant decline in academic anxiety from the pre-to-post assessment and a minor decline from the post-to-follow-up assessment phase in the intervention group as compared to the control group.
Table 2 presents the mean and standard deviation for each group at different stages, along with the results of mixed repeated measures ANOVA. A significant drop was observed in the levels of academic anxiety from pre-to-post-assessment and improvement was found in subjective well-being across all three phases. Mindfulness exhibited a significant interaction between group and assessment phases, indicating greater improvement in the intervention group from pre-to-post and follow-up assessments.
Mean, Standard Deviation, and Mixed Repeated Measure ANOVA.
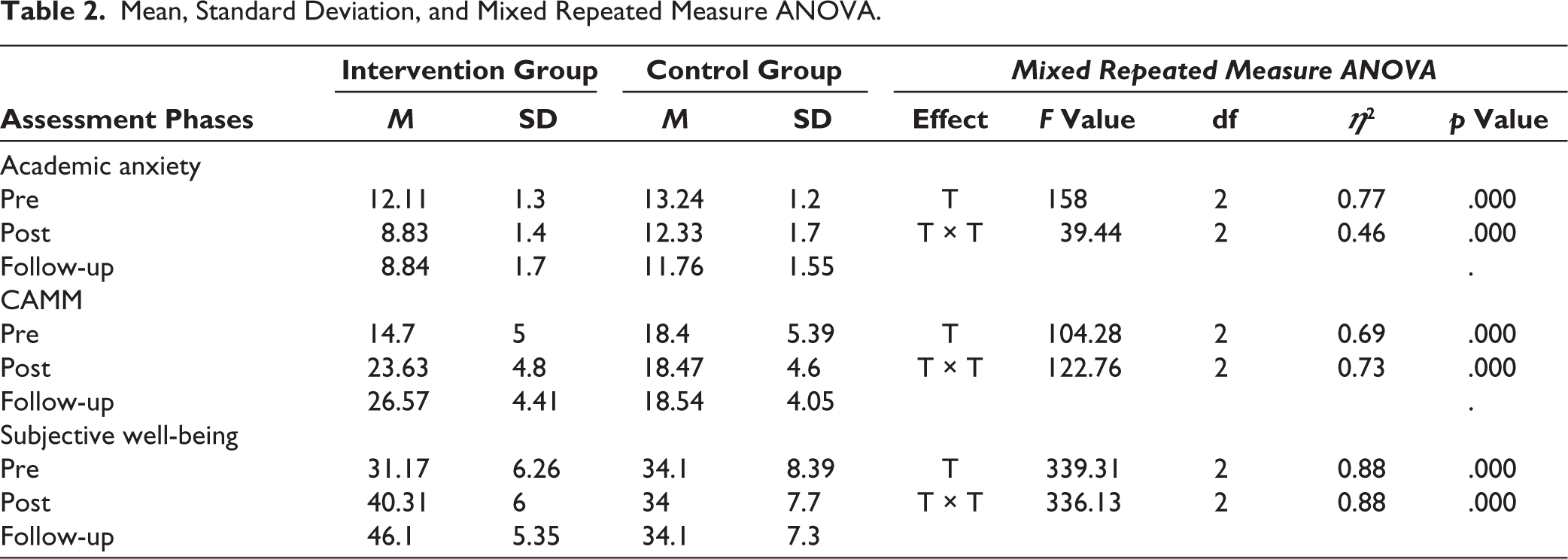
Further support is provided by mean differences between post-test and follow-up for subjective well-being, academic anxiety, and mindfulness. These results suggest a significant positive impact of the intervention on academic anxiety and the subjective well-being of the students.
Discussion
Numerous studies have consistently shown the beneficial effect of mindfulness on mental and physical ailments.25, 26 Along the same lines, this study aimed to understand the effect of MBI on the subjective well-being of rural adolescents with academic anxiety. The study included 93 participants who reported having high anxiety levels. The effectiveness of MBCT was evaluated through a control group intervention design, wherein the intervention (adapted from MBCT developed by Teasdale et al., 2002) was provided to the intervention group (47 participants) over eight sessions. The study reported a positive effect of mindfulness practice on the academic anxiety of rural adolescents.
The findings of the current study supported the disposition that mindfulness can be strengthened through practice. 27 The intervention schedule spanned across eight sessions and included homework assignments as well as a goal to integrate the practice in daily living, which allowed the participants to realize and practice its effects. The significant and consistent increase in mindfulness scores from pre to post and follow-up, showed that mindfulness disposition improved during the intervention and practice period.28, 29
The efficacy of the intervention schedule, with its various tasks and goals, contribute to the increased mindfulness capacity in the sample group. The various activities involved bringing the focus of the participants to the present moment while engaging in activities of daily living (eating, breathing, etc.). The intervention aimed at bringing to awareness the experience of automatic processes like thinking and responding while reflecting on the emotions involved. This encouraged the participants to delve into the practice of mindfulness and hence, incline their focus from their anxiety to the present moment. This enterprise can be supported by the premise that mindfulness is, in essence, the opposite of anxiety, which could have helped the participants get out of their one-track focus on their own thoughts and ruminations, allowing them to instead reflect on their thoughts as they come to their minds. Research suggests that the reduction in anxiety and other internalizing disorders was connected with the increase in mindfulness,30, 31 and it appears to be a result of this very action plan.
Another factor at play for the efficacy of the intervention plan has its foundation in the theory which suggests reperceiving as a consequence of mindfulness which in turn leads to positive changes in the participants. This construct of reperceiving includes components of intentionality, attention, and attitude, and it is the interplay of these constructs that makes MBI practical and effective. 27 Application of this theory in the current context implies the resolution of anxiety through attending to the present moment, with the intention of making conscious choices to respond to situations and ruminations in a modified way. These three constructs of mindfulness can be found to be at play in the intervention schedule of MBCT, where the goals and activities align to justify the same.
Consistent with the study’s findings, a recent systematic review found that 11 studies reported significant improvements in subjects’ well-being after the MBCT intervention.32, 33 This schedule of activities and planned goals helped participants become more attuned to the present moment and more accepting of their feelings and experiences, which in turn reduced stress and improved their subjective well-being.34, 35 Factoring these findings with respect to the current study, it seems appropriate to conclude the effectiveness of mindfulness practice on the academic anxiety of adolescents.
The findings of this study were supported by the findings of Weems et al. (2014) and Sohrabi et al. (2013). The only difference observed was that both studies demonstrated a significant reduction in academic anxiety in the follow-up duration (Shahidi et al., 2017; Weems et al., 2015), which was not observed in the present study. This could be due to the fact that the mean score of academic anxiety observed in the post-assessment suggests that the presence of academic anxiety was negligible as per the score interpretation given in the particular test. Therefore, in the follow-up assessment, there was little room for the decline of academic anxiety. The second could be due to the fact that the MBCT intervention plan used in the current study, though deemed fit for the Indian population by experts, could not guarantee complete cultural sensitivity.
A relatively small size with a particular sample location may limit the study findings from generalization. The dropout rate at the follow-up was relatively high which was not handled effectively. The sample size adjusted with the dropouts for the data analysis might have presented inflated statistical significance. Due to the fact that the MBCT intervention plan used in the current study, though deemed fit for the Indian population by experts, could not guarantee complete cultural sensitivity.
However, the findings are promising with those adhered to the entire intervention. Thus, this can be implemented as an intervention and adjunct strategy for the management and prevention of academic anxiety of rural school-going adolescents. This intervention introduced as a curriculum activity can be very beneficial, not only in helping to reduce anxiety but also in improving subjective well-being. However, future research with robust statistical methods like path analysis, mediation, and moderation analysis with large samples can bring out more promising results.
Conclusion
The current study implies that this MBI improves overall well-being and decreases academic anxiety in adolescents from rural areas in India. The findings of this study are promising, as it could help to manage academic anxiety in rural adolescents in a way that is easy to follow and relatively suitable for the Indian setting. The MBI intervention can be implemented cost-effectively in a school setting. The practice of daily academic activities in a mindful way makes the students more present-oriented and gives them the coping capacity to manage their worries, especially academic-related ones. The insight-building psychoeducation of this intervention enables them to incorporate the mindfulness practice in their daily lives and generalize it to other areas of concern.
Footnotes
Acknowledgements
We express our heartfelt gratitude to everyone who contributed toward the successful completion of this study. We would like to thank the principal of the school as well as the students who willingly participated in this study. Further, we express our appreciation and gratitude to the research advisory committee and the center for research for giving ethical clearance to this study. Lastly, we are thankful to our mentors, colleagues, and friends who provided support and encouragement for the completion of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee (Christ Deemed to be University) No. CU: RCEC/00297/06/22) dated June 7, 2022. Written informed consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.