
Abstract
This narrative review aims to identify key concepts associated with school refusal, including various risk factors, and to discuss current practical assessment and treatment methods available or under trial. For this study, we searched MEDLINE and Scopus databases for articles containing keywords like “school refusal” and associated keywords such as “childhood,” “adolescence,” “risk factors,” “interventions,” and “assessment.” Thirty-eight original articles in English containing these keywords, published in the last 10 years on the above platforms, were included. We excluded studies focusing on school refusal solely in a subset of the population, such as autistic children or immigrant children. This review found that in India, school refusal is often ignored, especially in lower socioeconomic families, due to non-affordability and poor access to appropriate resources, and is sometimes also equated with truancy and bad behavior. Various risk factors at the parental and school level promote this behavior, and therefore, appropriate interventions at these levels are necessary. As per current evidence, psychoeducation and multidisciplinary treatments are the most effective in managing such children. Early detection of such cases and coordinated efforts by all stakeholders are crucial for effective intervention.
Introduction
The term “school refusal” was first used to describe the behavior of children who did not attend school because of emotional distress.1, 2 Consistent evidence has demonstrated that school absenteeism is most prevalent among primary school students.1–5 It is often associated with the inability to form lasting peer relationships and severe academic underachievement. 2 It is crucial to pay attention to this because, if it persists, it could result in less prospects for postsecondary education, trouble finding work, greater social isolation, and a higher risk of psychiatric disease. Although school refusal is not technically recognized as a mental diagnosis by any classification system, children who exhibit such behavior frequently experience emotional discomfort or some type of psychiatric condition. Thus, in the child and adolescent psychiatry sphere, school refusal is frequently regarded as an emergency.
Often, the terms “truancy” and “school refusal” are erroneously used interchangeably. However, the literature suggests that unsanctioned absences may be classified as truancy when associated with antisocial behaviors and as school refusal due to underlying anxiety, depression, or other mental distress. 6 This implies that the provision of care may differ based on the classification of school absenteeism. Also, while school refusal is a common presentation associated with a gamut of psychiatric disorders such as anxiety disorders, there is a recognized heterogeneity present at the causal level, which makes it difficult to distinguish and, therefore, to manage school refusal effectively.
In recent times, more research has been conducted on school refusal in developed countries. However, most Indian research is focused on clinical correlates, comorbidities, and outcomes of school refusal. Moreover, large-scale studies focusing on interventions and assessment methods in school refusal cases in India are deficient. Therefore, this narrative review aims to identify the key concepts associated with school refusal, including the various risk factors, and to discuss the current practical assessment and treatment methods available or under trial.
Methodology
For this study, we searched MEDLINE and Scopus databases for articles containing keywords like “school refusal” and associated keywords such as “childhood,” “adolescence,” “risk factors,” “interventions,” and “assessment.” Original articles in the English language containing these keywords and published in the last 10 years on the above platforms were included. Studies focusing on school refusal solely in a subset of the population, such as autistic children or immigrant children, were excluded.
Figure 1 depicts the methodology of this study.
Selection Process of Articles.
School Refusal: Key Concepts
Epidemiology
The current prevalence rates of school refusal among children and adolescents have been reported to be between 2 and 16% worldwide.7, 8 In India, several studies have reported a prevalence rate of up to 7%.9, 10 Research indicates that school refusal peaks around the age of transition between school stages at the start of primary school or after the move to secondary school and is more common in secondary-age pupils.11–13 Some studies have found a significant association between school refusal and socio-demographic aspects like the gender of the children, family type, regular income of families, and parental education.8, 14 Most studies have reported school refusal behavior among male children more frequently. 12 These rates may vary based on detection rates in different countries, which again vary based on educational and socioeconomic factors, awareness about school refusal behaviors among families, and access to mental health resources. In India, school refusal is often ignored, especially in lower socioeconomic families, due to non-affordability and lack of access to appropriate resources. 15 Therefore, screening such cases at the school level is crucial for early intervention. Moreover, one of the first measures before employing any preventive measures is to know the risk factors associated with the behavior, which facilitates early identification and timely intervention.
Risk Factors for School Refusal Behavior
Psychiatric Disorders
In various studies, most pupils with school refusal behavior were invariably detected with a psychiatric disorder. In a recent study, the prominent psychiatric co‑morbidities in such cases were unspecified childhood emotional disorder, separation anxiety, conversion disorder, over‑anxiety disorder, and somatoform disorder. 16 Previous studies have shown that children with complaints of school refusal generally present with anxiety symptoms, and teenagers have symptoms related with anxiety and mood disorders. 17 Some studies have highlighted mental retardation and learning difficulties as precursors to school refusal behavior. 15 Similarly, children with school refusal behavior are often found to be at risk for developing subsequent psychiatric disorders. For instance, in some studies, almost 30% children with anxiety disorders have been described to present with school refusal initially.18, 19 Allen and colleagues have previously reported that mental health conditions impair the cognitive and emotional development of the child. 20 Often, this leads to difficulty coping with school and causes children to refuse to attend school. Consequently, school refusal can disrupt the formation of progressive self-perception and healthy social relationships among refusers, resulting in detachment from friends, peer rejection, and academic collapse, which can lead to psychiatric illnesses. 21 It implies thus that most school refusal behaviors and psychiatric disorders may have a bidirectional relationship regarding causation. This becomes important for management as the treatment of one can potentially cause a decrease in the other and the identification of psychiatric disorders should always be considered in any case of aberrant behavior like school refusal lest the disorder goes untreated.
Personal Factors
Several studies have reported a child’s temperament as an important predisposing factor to school refusal behaviors. For example, in one study, 57.6% (n = 19) children presenting with school refusal had temperamental issues: anxious traits, adamancy, sensitivity to criticism, and introversion. 10 Carpentieri et al. concluded that children with school refusal were characterized by inhibited, self-constricted, and emotionally dysregulated personality styles. These children reported more negative automatic thoughts concerning personal failure, fewer negative automatic thoughts concerning hostility, and fewer positive ones. 22 Maric and colleagues have previously reported that negative automatic thoughts relating to personal failure and hostility and the negative cognitive error of overgeneralizing all predict school refusal independently. 23 Thus, cognition and temperament significantly affect how a child copes with stressors around him or her, and an inability to do so may manifest as school refusal.
Other factors include chronic medical illnesses (like typhoid fever, history of febrile seizure, disorder, h/o surgery, obesity) preceding the onset of school refusal, which may lower the child’s self-esteem. 10 In addition, many students also have to contend with “bias bullying,” which results from the victim’s perceived membership of a particular, often marginalized, group (e.g., based upon gender, race/ethnicity, sexual orientation, faith/religion, and disability). 24 Identification of such personal factors becomes crucial and also pertinent to ensure holistic care.
Psychosocial Factors
Parental Factors
Family factors such as substance abuse, psychiatric illness, death or separation of parents, maltreatment, and family discord often are critical risk factors for school refusal behaviors.8, 10 Other factors, including an account of abuse, adoption, stepmother, and issues with peers, influence school refusal behavior. 10 However, contrary to other studies, Fukuya et al. found that child rearing, such as parent–child dealings and child maltreatment, may not be associated with school refusal among elementary school pupils. 7 Differences in study design and cultural differences in parenting and child-rearing practices may account for this discrepancy in findings. However, this also calls to attention the role of family dynamics, parenting styles, and socio-cultural factors in school refusal and how they can be targets for intervention such as family therapy as it has been shown through various studies that dysfunctional family dynamics tend to maintain and even perpetuate the target problem despite seemingly adequate intervention.
School Factors
Teacher-perceived psychological control, poor relationships with peers at school, academic difficulties, and adjustment problems have often been cited as essential triggers for school refusal, especially among school going children.9, 25, 26 In a previous study, Yadav and colleagues hypothesized that an apparent discord between parental expectations and an adolescent’s aptitude or attitude toward academic achievement might reinforce the behavior. 27 Other reasons included complications or fear associated with a teacher or other students due to bullying, teasing, etc. 9 Compared to children, adolescent refusers tend to have a greater sense of independence, which can help them refuse adult structures. However, they might need help engaging with more complex, demanding, specialized curricula. As a result, adolescents often tend to endure more severe symptoms.28, 29 Children with school refusal behavior often suffer the highest emotional, behavioral, and physiological pointers of stress. 30 Moreover, their school achievement is negatively foretold by school refusal and the number of absences. 25 Therefore, it becomes crucial for schools to actively liaise and be involved in a more collaborative manner for the proper management of children who demonstrate school refusal, and the earlier this is initiated, the better, to prevent the loss of precious time in the academic progress of children.
Protective Factors
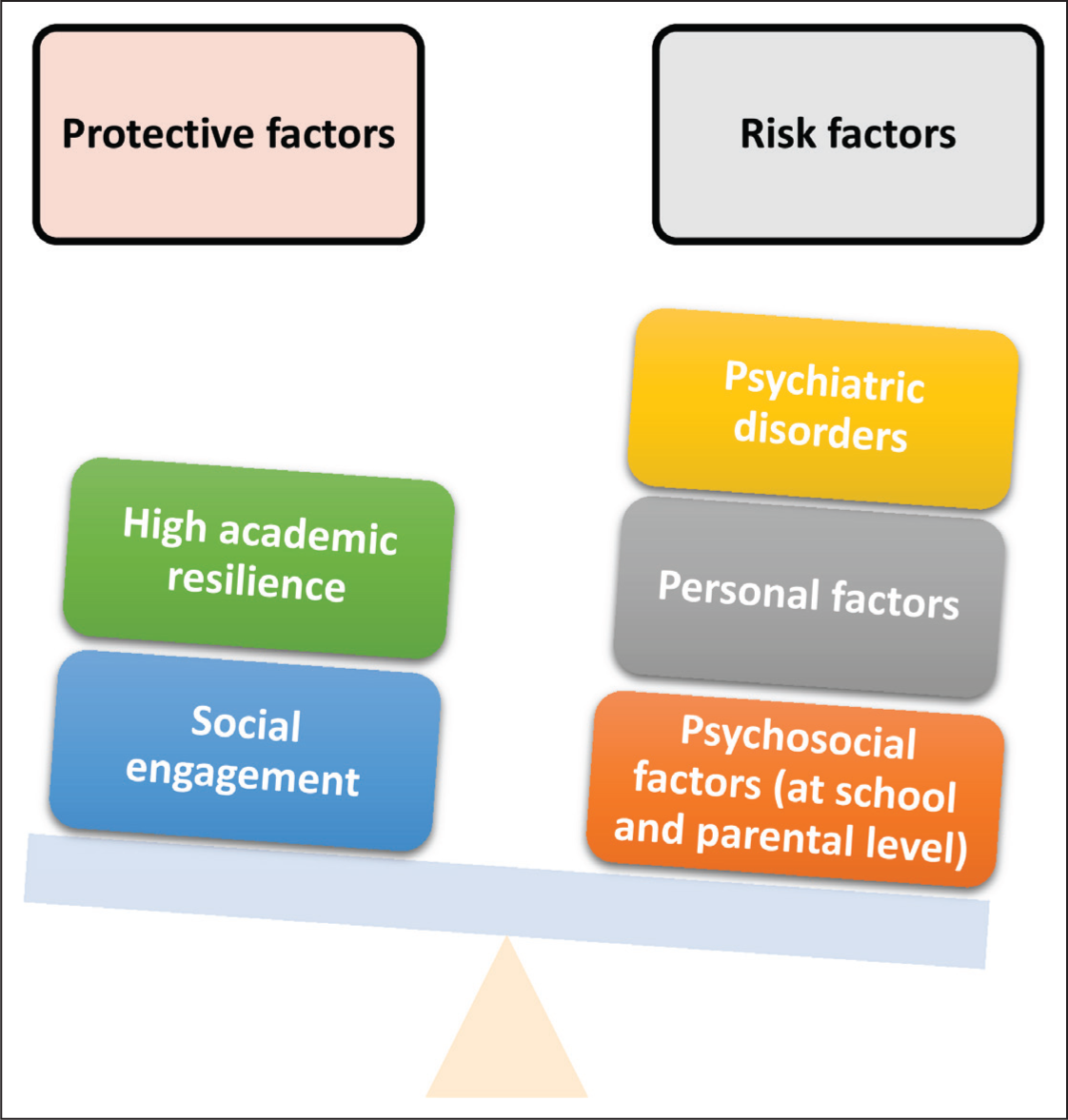
Studies report that elevated academic resilience has a robust protective role against problems of negative school attachment and problematic school absenteeism among young people. 31 In Ingul’s study, anxious school attendees tend to have fewer negative personality traits, social anxiety, and behavioral issues. This study’s findings suggested that simply managing the anxiety problems of nervous school refusers may not be enough. However, these findings imply that increasing resilience and participating in prosocial activities may be beneficial and may reduce the chance of absence. 32 The social engagement of children in question thus becomes a crucial part of the treatment program, serving as a robust protective factor and promoting improvement. Figure 2 summarizes protective and risk factors associated with school refusal.
Risk Factors and Protective Factors Associated with School Refusal.
Assessment
In commencing an initial assessment, it is essential to identify that school refusal could be a resultant symptom of additional pervasive problems. For example, somatic symptoms associated with anxiety, such as palpitations or abdominal pain, could have a physical basis. On the other hand, caregivers and school staff may mistakenly consider stress-related physical problems purely physical complaints, resulting in delays in suitable treatment, with harmful consequences. 26 Therefore, a thorough medical assessment involving a physical examination with proper follow-ups is valuable.
Educational and psychological calculations typically examine a child’s academic ability level because low functioning is a significant problem among school refusers. 33 Intellectual assessment and verbal ability can help to indicate what role cognitive therapy might play in intervention. A comprehensive mental health assessment to understand issues and identify comorbidities is crucial to ensure that intervention is most helpful for that individual. This typically involves interviews with the child, the parents, and the family, to offer a holistic view of problem areas; target concerns; and the scope of improvement and avenues for effective intervention.
Diagnosis
Until recently, Berg’s criteria for diagnosing school refusal had been the most comprehensive in describing school refusal behaviors.
34
However, in their study, Maric and colleagues offered a helpful operationalization of this definition as follows:
H/o < 80% attendance recorded over the past 2 weeks (excluding legitimate absences). The presence of an anxiety disorder as identified in DSM-IV [excluding obsessive-compulsive disorder (OCD) and post-traumatic stress disorder (PTSD)]. Parents could account for the child’s whereabouts on days marked by school absence. No concurrent DSM-IV conduct disorder is present. There is clear commitment on the part of parents to help the child achieve total school attendance except for legitimate reasons.
35
Various scales have been developed to evaluate school refusal behaviors. The School Refusal Assessment Scale has been widely reported in the literature and comprises a child, parent, and teacher form and examines school refusal in association with negative and positive reinforcers. 36 In the Indian population, Srivastava and colleagues employed this scale on 1640 students to assess the prevalence of school refusal in their sample. 14 In Germany, Knollmann and colleagues did a validation study for a new scale called the Inventory of School Attendance Problems (ISAP), which evaluates the quality and function of a broad spectrum of school attendance problems, including school refusal. 37 However, there is yet to be a consensus on a good psychometric tool that can be employed for diagnostic purposes in field research and setting parameters. Future research could perhaps focus on developing and validating culturally sensitive psychometric instruments that can be used to operationalize the diagnosis of school refusal further.
Numerous psychological evaluation tools (e.g., teacher and parent rating scales, self-report measures, and clinician rating scales) have been established to provide information about the child’s general functioning at home and school. Generalized scales (e.g., Child Behavior Checklist and Teacher’s Report Form) identify areas of difficulty. Specific rating scales assess symptoms and severity of psychiatric problems, including anxiety and depression.37, 38 In addition, they propose a functional and symptomatic evaluation of refusal behaviors and thus deliver more precise data, thus helping in designing the intervention protocols better.
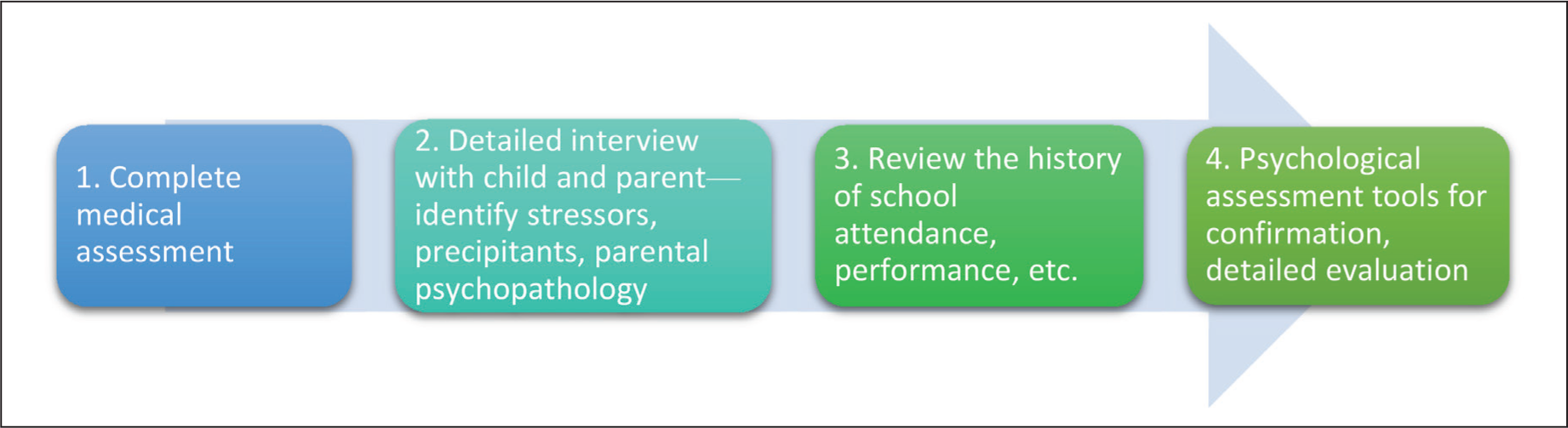
Figure 3 shows a summary of suggested steps in the evaluation of a child presenting with school refusal:
Suggested Steps in the Assessment of a Child Presenting with School Refusal.
Treatment
Heyne and colleagues supported the use of a developmentally sensitive style that tailors the treatment to a young person’s specific needs, developmental level, and family circumstances. 29 Regarding school refusal, research points toward a more prominent role of non-pharmacological and multidisciplinary interventions as the objective is a complex and multifaceted one and requires a collaborative approach rather than an individualistic one.
Non-pharmacological Approaches
Individual-based Approaches
Behavioral methodologies for school refusers are primarily based on exposure and utilization techniques such as systematic desensitization (incorporating relaxation training), flooding, emotive imagery, modeling, shaping, and contingency management. In addition, techniques such as social skills training and problem solving concentrate on a child’s behavior rather than on intrapsychic conflict and highlight treatment in the context of the family and school. As a first step, educating the child regarding the nature of feelings, negative thoughts, and negative behaviors that comprise anxiety is crucial. Then, depending on the underlying reason for refusal, the therapist should introduce the treatment plan (exposure/coping/distraction/alternate statements). 39 Several studies have tried to examine the effectiveness of these approaches and have found them to be the most effective of all modalities.
Nursalim and colleagues studied behavioral interventions of 40 senior secondary students who were divided into four groups of 10 students each. One cluster of students was given the ego state therapy (EST), another cluster was given systematic desensitization (SD), yet another group was given a combination of SD and EST (SDEST), and one group of students received no treatment. The experiment was conducted in six sessions, each for one hour. The authors concluded that SDEST is significantly more effective in managing school refusal because it can comprehensively construct memories positively and indorse counselees’ courage in adapting to latest and upcoming events. 40
Cognitive behavioral therapy (CBT) is another effective method for reducing school refusal, which tries to restructure a child’s thoughts and actions into a more robust and adaptive frame. It is the most studied technique in school refusal research. Here, children are motivated to challenge their fears and are taught how to alter negative thoughts. It involves identifying and recognizing thoughts and emotions, their restructuring, and creating a new functional answer to deal with symptoms. It includes engaging the child by recognizing the reality of feelings, working together to plan school return, and dealing with anxieties through problem-solving, relaxation training, breathing retraining, and social skills training. 41 Several studies have attempted to examine the efficacy of CBT in school refusal. For example, in their longitudinal study on manual CBT, Maric and colleagues found that the post-treatment increases in school attendance and a decrease in fear about being in the school the next day were mediated by self-efficacy worked on during the CBT sessions. 35 Similarly, in their study, Hannan and colleagues tried an intensive CBT school refusal program among 25 students, in which sessions lasting up to 2 hours were delivered daily. Based on their needs, individual care interventions were devised that included standard CBT procedures and interventions specific to the needs of a student/family. Treatment was delivered daily over 3 weeks. An improvement in school attendance was noticed, from only 12% of students attending pre-intervention to 60% post-intervention. The authors reported that intensive CBT allows clinicians the necessary time to address maintaining factors of school refusal within a short timeframe (daily). In addition, it will enable extended time in the session to build skills and address any daily issues that arise. 42 However, some studies suggest standard CBT manuals developed for treating anxiety or depressive disorders may not be appropriate for managing school refusal, given its highly heterogeneous nature. 43 As a result, authors from various countries have tried to modulate CBT according to their social and cultural structures. For example, in Sweden, Strömbeck et al. studied a multimodal CBT intervention for chronic school refusal among adolescents, called hemmasittarprogrammet (HSP). At the end of their study, participants went to school four times more at follow-up than before treatment. In addition, levels of anxiety and depression were lower both post-treatment and at follow-up for youths and their parents. 44
The efficacy of dialectical Behavior therapy for school refusal (DBT-SR) has also been studied. DBT-SR is a multimodal method to address severe emotional and behavioral dysregulation mechanisms maintaining school refusal behavior. It utilizes a web-based coaching program to provide active, real-time skills coaching to youth and parents at times and in the context of the most urgent need (at home, during the morning hours). A pilot trial and illustrative case examples provide “proof of concept” that DBT-SR is reasonably feasible and acceptable to clients and therapists. 45
Emerging research also supports mindfulness-based interventions (MBIs) for anxious school refusal. 46 Mindfulness encourages individuals to explore how they might have a “different relationship not only to thoughts, but also to feelings, body sensations, and impulses to act, that is, to the whole mind-body state.” 47 School-based programs such as Mindful Schools, MindUp, and Learning to BREATHE are some interventions studied abroad that are organized, purposeful, and evidence based. 48 These interventions have been studied extensively and seem to be efficacious, backed by sound statistical evidence.
Family-based Approaches
Family-oriented interventions are the second-most crucial aspect that help manage children’s school refusal. Years earlier, Siegel argued for a central focus on relationships in the prevention of and interventions to address school refusal. As noted above, anxiety disorders in children are affected by the family and community context of a child’s life. Thus, when developing strategies to address school refusal, it is crucial to always do so in a context that acknowledges relationships as central, including the child’s relationship with attachment figures, school staff, and other students. 49
Involving family members in various techniques is found to be effective in management. Usually, it concerns methods such as establishing fixed routines, contingency contracts, etc. In a French study, six school-refusing adolescents and their parents (n = 9) were administered multifamily therapy in an adolescent department. Initially, the six families expressed painful emotions, social isolation, and separation anxiety in interviews. At the end of sessions, multifamily therapy increased teenagers’ self-confidence. It allowed group experience; for parents, it supported them and relieved them from stigmatization and guilt. Parents became more aware of their adolescents’ suffering and their insight. They all considered that multifamily therapy improved intra-family communication and expression of emotion. Participants highlighted benefits of intergenerational interactions, activities, groups, and guidance from therapists. 50 The family-based approach also assuages concerns of family members apart from those of the child, provides hope by making them an active part of the treatment process, and allows them to witness the improvement as the treatment progresses.
School-based Approaches
School-oriented interventions require parents to liaise with the school and discuss the treatment plan, where the common goal should be to send the child to school as soon as possible. School counselors must determine how to strengthen the child’s connection to the school and work with parents/guardians to develop interventions. Various school interventions have been tried across the world.
In Japan, between 2009 and 2015, parents of 62 adolescents displaying school refusal were invited to implement a school-based rapid return approach based on the flooding and exposure and response prevention therapy. To the intervention group, after discussing the adverse effects of prolonged school refusal, the school counselor explained the intervention process as follows: (a) at some point after the meeting, parents would declare to their child that they would be forcing him/her to attend school; (b) the intervention would commence two days after the declaration, during which time parents would encourage their child to get ready to return to school (e.g., preparing textbooks and school uniform); (c) parents would use planned ignorance of the child’s behaviors associated with school refusal, such as crying, somatic complaints, or tantrums; (d) parents would conceal sharp implements at home to reduce the possibility of self-harming; (e) parents would wake their child up, get him/her changed into the school uniform, and escort him/her to the school gate; (f) school staff and the classroom teacher would escort him/her from the school gate to the classroom, perhaps with the support of close friends; (g) school staff would come to the family home if parents could not escort the adolescent to school on time due to resistive responses; (h) after arriving at school, the adolescent would be expected to stay at school all day (preferably in the classroom for the whole time), and school staff would not permit him/her to leave school early, even if the adolescent wished to do so; and (i) the intervention would be suspended if parents requested it. Of the 39 cases in which the approach was implemented, 28 adolescents (72%) resumed attendance at their original school, 2 (5%) transferred to another school, and 9 (23%) did not resume attendance. In contrast, all 23 non-intervention cases refused to attend school for 3 months or longer, and none of these adolescents resumed to regular school attendance within 9 months. This study suggests that the rapid return method may be the most practical for adolescents demonstrating school refusal and refusing to attend individual therapy. However, this approach is ethically complicated, and the authors suggest its use only under specific circumstances. The rapid return approach is especially contraindicated when parents encounter difficulties (e.g., anger management, depression, low self-efficacy) and no substitute support people can escort the young person to school. 51
In Australia, McKay-Brown and colleagues designed and implemented a multidisciplinary, school-based program called the In2School as a pilot. In2School includes well-known cognitive and behavioral interventions for school refusal, an outpatient classroom program, parent groups, attention to social skills, provision of psychoeducation for staff at partner schools, and exhaustive outreach support to facilitate a young person’s return to the partner school. Most importantly, it has at its center at a multidisciplinary education- and health-focused partnership between mental health clinicians and teachers. This program focuses on young persons missing more than 50% of school in the previous 6 weeks due to mental health disorders, including anxiety or depression. Over 14 weeks, therapeutic and educational interventions were molded into the learning environment via a transitional classroom to support youths’ return to school. Of the seven youths recruited initially, six returned to conventional schooling, with attendance levels maintained for 6 months after completing the intervention. In addition, progress was observed in mental health recovery, quality of life reports, increased social interactions with peers, and positive experiences at school. Initial findings based on this piloting of the In2School program suggest that a wraparound model for school refusal intervention may support the return to school while improving young people’s health outcomes and quality of life. 52 The school-based approach has the advantage of being at the center of the treatment strategy and also the target of behavior modification as the ultimate goal is to make sure that the child doesn’t continue with school refusal behavior.
Pharmacotherapy
Melvin and colleagues investigated that the augmentation of CBT with fluoxetine betters outcomes in anxious school-refusing adolescents (11–16.5 years). Sixty-two participants were randomly allocated to CBT alone, CBT + fluoxetine, or CBT + placebo. CBT was conducted twice weekly for the first four sessions (50–60 min duration) and then weekly for the remaining eight sessions. After acute treatment, monthly booster sessions were given for 3 months in the maintenance phase. Attendance of at least eight (67%) sessions is required to qualify as having completed the treatment. At the end of the study, all groups showed significant improvement on primary (school attendance) and secondary (anxiety, depression, self-efficacy, and clinician-rated global functioning) outcome measures, with gains primarily maintained at 6 months and 1 year. During the follow-up period, anxiety and depressive disorders continued to decline. In addition, all three treatments improved school attendance, with attendance rates increasing from 15% to 52% after acute treatment and maintained at 54% at 6-month and 12-month follow-ups. The only significant between-group difference was greater adolescent-reported treatment satisfaction in the CBT + fluoxetine group than in the CBT-only group. Thus, they concluded that using anti-depressants is an effective augmentation strategy in school-refusing adolescents. 53 In another RCT study of school refusers in China, Wu et al. found no additional efficacy for fluoxetine and CBT compared to CBT alone. However, improved school attendance was found for both groups. Therefore, our recommendation is to reserve pharmacotherapy for severe cases and for those children in whom anxiety and depression are the primary cause of school refusal. 54 Concerns like hampering the physical growth and cognitive development of a child are major concerns that cannot be overlooked, and hence, pharmacotherapy is utilized as a last resort and in a very controlled and judicious fashion.
Examples of Screening and Prevention of School Refusal Behaviors from Around the World
While several treatment modalities for school refusal do exist, research has consistently shown that early detection and prevention have better outcomes in the long run. As a result, several countries have tried to implement screening programs for school refusal, which have shown promising results and can be utilized with adaptations in the Indian context.
For example, in Japan, preschool developmental-behavioral screening and consecutive support programs were undertaken, wherein 1,165 children were recruited at age five and followed up over 8 years. The survey had a three-step method as follows. Step 1: Interviews and checklists overseen by public health nurses and nursery/kindergarten teachers for all children. Step 2: Medical screening for all children performed by a local/homeschool doctor. Step 3: Diagnosis in selected children carried out by child neurologists, special support education teachers, and clinical/school psychologists. Subsequently, for 1–2 years until entrance into elementary school, these children and their parents were given speech, behavioral, and mental support, as well as group play therapy in nursery/kindergarten. During the 8-year study period, 56 children (5.4%) were identified with developmental disorders, and six children were diagnosed with maltreatment by their parents. Of these subjects, 40 children received support consecutively after entrance into school, 38 of whom entered regular elementary school, and 32 attended regular classes for 1–6 years. A total of 39 of 40 children attended school without refusal. Moreover, the total number of students who refused to attend school in elementary school decreased for 3 years from 8 of 3246 children (0.25%) to only 1 of 2646 children (0.04%). 54
Sleep disorders and extreme difficulty in awakening are the leading triggers of school refusal. The accumulation of chronic sleep deprivation accompanied by a late-night lifestyle was considered the essential inciting factor. Several interventions focusing on sleep education have been studied. In Japan, a sleep education program (Min-Iku) for primary school students was initiated to improve student lifestyle and prevent future school refusal. The Min-Iku included the execution of a “daily life rhythm survey” by recording the sleep–wake rhythm in a table for 14 days, an assessment of the sleeping table according to classifications A–D, interviews of stage D children and their guardians, lectures on the status of daily life rhythms for parents and teachers, and 45 min classwork for all participating pupils. They found that 10% of students developed school refusal in the first year, which decreased each year after implementing the Min-Iku program and finally reached zero. At the end of 5 years, the Min-Iku program for primary school pupils successfully achieved a more regular night-time sleep pattern and a regular life rhythm, which prevented school refusal during the subsequent JHS years. 55
In the USA, a multi-tiered system of support (MTSS) is used to deliver school refusal interventions at the community level. This is based on two models: RTI (response to intervention) and PBIS (positive behavior interventions and support). RTI is a rigorous academic framework designed to assist instructors’ instructional needs based on student learning and behavior; its goal is to close the achievement gap.56, 57 PBIS, on the other hand, focuses on social and emotional elements that influence behavior. Each strategy employs a three-tiered intervention intensity model, resulting in the MTSS framework, which helps educators to continue to work with problematic kids. 58 Tier 1 supports are interventions that are provided to all students and are typically anticipated to offer adequate support to 80% of pupils in a school. Tier 1 school-related techniques include those aimed at creating a high-quality learning environment for all pupils. Tier 2 services are more targeted at meeting the needs of around 15% of “at-risk” adolescents who may be suffering anxiety at school or having missed many days of school. Tier 3 supports are intense interventions designed to fulfill the requirements of around 5% of at-risk adolescents, and they are sometimes less engaged in school. 59
Working with families to promote school attendance is one of the primary techniques for reflecting school refusal in this group of students, and school officials may work with families to highlight school attendance. A positive home/school contact can provide useful information to staff and build partnership between a student’s family and the school. Small groups led by school counselors or other school personnel (e.g., teachers, school psychologists, school nurses, speech/language pathologists) may offer kids more comprehensive education and assistance in the development of academic, social, and coping skills. These clusters may concentrate on academic deficiencies or social/emotional abilities, as well as cognitive-behavioral and mindful awareness events.60, 61 Structured recesses or meals, supported study halls, and academic support during recess are some more treatments that may help with the inclusion of mindfulness techniques. Schedule changes can be implemented to assist at-risk students. These changes may involve a late start, early out, strategically placing high-demand and low-demand classes, and matching students with positive teachers. Classroom teachers can help students by breaking large assignments into smaller ones, giving students more time to complete assignments and tests, avoiding timed projects and tests, shortening assignments, providing copies of class notes, and providing preferential seating, such as seating anxious students with positive peers. In Tier 3, emphasis is placed on determining whether the student qualifies for special education and an individualized education program (IEP), as well as conducting a functional behavior assessment (FBA) and PBIP to analyze a student’s behavior and develop a plan to address problem behaviors more closely. 49
The instances elucidated above provide a guiding path toward the structuring of similar programs in the Indian target population.
Conclusion
While school refusal is a pervasive problem, we still need to have more knowledge about the exact mechanisms mediating it. Also, working with school refusal children can be challenging due to its multifaceted nature. The ultimate success of the treatment depends on how all the pieces are pulled together. The school, the parents, the child, and the mental health professional all play a vital role in returning the child to school and functioning well there. Although various interventions and culture-specific innovations in treatment have been tried worldwide, there is still a dearth of research regarding effective interventions among Indian children. Future studies should focus on testing targeted interventions to develop efficient protocols for the community to deal with such cases and thereby bring about a decrease in the deleterious school refusal behavior, which evidently leads to loss of precious time with respect to the education of the children and hampers their cognitive development, thus assuming significant importance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.