
Abstract
Background:
The present study aimed to investigate the role of family process and content factors in predicting coronavirus anxiety and self-care behaviors during the COVID-19 outbreak in adolescents of Iran.
Methods:
The present study was a descriptive correlational study. Five hundred Iranian adolescents aged 14 to 18 were selected through the voluntary sampling method. Self-Report Family Process Scale, Self-Report Family Content Scale, Corona Disease Anxiety Scale, and Corona Disease Self-care Behavior Questionnaire were used.
Results:
Pearson correlation and multivariate regression (stepwise method) were used to analyze the data. The results of the stepwise regression analysis showed that decision-making/problem-solving (B = –0.17), and coping skills (B = 0.11), could significantly predict 0.16 of COVID-19 anxiety. In addition, coping skills (B = 0.19), communication skills (B = 0.14), and family cohesion/respect (B = 0.11) could predict 0.29 of self-care behaviors. Regression analysis also showed that job, education (B = –0.17), and time spent together (B = 0.12) could predict 0.20 of COVID-19 anxiety. Furthermore, facilities (B = –0.3/92) could predict 0.20 of self-care behaviors.
Conclusions:
We can conclude that changes in process and content factors of the family are associated with changes in anxiety and self-care behaviors during the COVID-19 outbreak.
Introduction
Infectious diseases have been a significant threat to human health throughout history, and the emergence of the COVID-19 virus is the most recent example. As of December 31, 2019, a case of severe respiratory infection was reported in Wuhan, China, which caused great concerns. The new coronavirus manifests itself in most patients as a respiratory disease. In some patients, it could lead to pulmonary complications, septic shock, and death in some cases. 1
Studies have shown that the COVID-19 outbreak has had a significant impact on the mental health of children and adolescents. They experienced increased stress, anxiety, depression, and fear of illness and death. The disruption of daily routines, reduced social interactions, and limited physical activities due to the quarantine measures have led to a sedentary lifestyle, poor diet, and disturbed sleep patterns, which put them at risk of obesity, cardiovascular, and respiratory diseases. Additionally, the closure of schools and loss of entertainment have further exacerbated the psychological and social consequences of the pandemic on children and adolescents. Therefore, it is essential to address the mental health needs of this population and provide them with the necessary support and resources to cope with the pandemic’s impact.2–3
Anxiety disorders have been prevalent among the psychological consequences of the pandemic, affecting both adults and children. The quarantine period, fear of infection, fatigue, frustration, and misinformation about the disease have contributed to the development of anxiety disorders. The lack of communication with peers and teachers, lack of personal space at home, and reduced family financial capacities have also intensified anxiety among children and adolescents.4–5 These disorders are characterized by the feeling of fear and apprehension of an unfortunate event, along with a variety of different physical symptoms mediated by the autonomic nervous system. 6 Many children and adolescents have experienced anxiety, especially during the outbreak. 7 The lack of information about the COVID-19 virus has exacerbated anxiety, leading to feelings of loneliness, decreased social support, reduced life expectancy, and fear of infection. 8 The anxiety can lead to feelings of loneliness, decreased social support, life expectancy, and fear of infection.9–10 Furthermore, the stress and anxiety of COVID-19 can impact the immune system and make people vulnerable to the disease. 2
COVID-19 was not the first pandemic and will not be the last one to occur. This fact indicates the importance of self-care. Self-care is a key concept in health promotion and refers to any action that is done to increase or enhance the health and self-fulfillment of a person or group. 11 Self-care improves the quality of life and reduces the number of hospitalizations that patients experience. By continuously following it, acute and chronic complications of the disease can be prevented or delayed. 12 Nowadays, more attention is paid to the psychological aspects, affecting the incidence and treatment of physical diseases. 13 Numerous studies have assessed the reasons for the lack of proper self-care in people and have identified environmental and individual barriers to the optimal care of the disease. Among these barriers are psychological barriers, the role of which in the occurrence of health behaviors is well-clarified today. 14
The family is a dynamic system consisting of 2 dimensions: family processes and family contents. Family processes are a set of actions that each family uses to adapt to new conditions. 15 It includes decision-making/problem-solving, coping skills, cohesion/respect, communication skills, and religious orientation. The family process refers to a family regulatory function that includes the ability to adapt to needs and new circumstances, enabling the family to cope effectively with new crises. The second dimension, the content of the family, includes all contents that form the objective and completely tangible reality of the family members’ lives. Family content refers to the family’s assets or capacity in the areas of job and education, time to spend together, financial resources, physical appearance/social status, physical and mental health, living space, and facilities. 16
Previous studies indicated that familial factors like family financial difficulties, domestic conflicts, and tension with parents can lead to adolescent anxiety during the COVID-19 outbreak and suggested that experts like psychologists, counselors, and social workers, help families use home confinement as a good opportunity to enhance the interaction between parents and children, involve children in family activities, and improve their self-sufficiency skills. With the appropriate parenting styles, family bonds can be strengthened, and children and adolescents’ psychological needs met during pandemics. 17
Family process and content factors can predict stress, anxiety, and depression among adolescents. 18 In families in which adolescents have more healthy contact with their parents, forming a secure attachment is better for them, and safe attachment is associated with less health-related anxiety and stress. 19
Social learning theory posits that family behaviors, such as parenting style, lifestyle practices, and communication, influence both the physical and psychosocial maturation of children and adolescents. Furthermore, mother and father education, warm and caring behavior of parents, providing emotional support, and parental monitoring can lead to self-care among adolescents by reminding them of self-care behaviors like social distancing, mask use, and washing-hand behaviors during the COVID-19 outbreak. On the other hand, parents’ self-caring behavior can be a healthy model. Moreover, open communication, and conflict resolution, can affect adolescents’ self-care behaviors by rationally managing the anxiety sources during the COVID-19 outbreak. In addition, studies indicated that the positive effects of nurturing family relationships on adherence to therapeutic regimes for adolescents can be significant.20–21
Based on the importance of managing anxiety and self-care behaviors in adolescents, especially during the outbreaks, and as no study was found to explore the role of content and family process factors on the self-care and COVID-19 anxiety of Iranian adolescents, this study’s hypotheses are:
Family process factors can predict COVID-19 anxiety in adolescents. Family process factors can predict the COVID-19 self-care behaviors of adolescents. Family content factors can predict COVID-19 anxiety in adolescents. Family content factors can predict COVID-19 self-care behaviors of adolescents.
Material and Methods
Participants
The present study was designed as an applied, descriptive-correlational study. Five hundred Iranian adolescents aged 14 to 18 were selected through the voluntary sampling method. Based on the Krejcie and Morgan table for a statistical population of above 100000, 348 samples are sufficient. We used 500 participants, and therefore adequacy of sampling has been considered. 22
Procedure
The study was approved by the IRB of the first-author university. After obtaining permission from the school authorities and providing instructions and assent forms to parents on social networks, all the volunteer adolescents completed the questionnaires. Social networks such as Telegram, WhatsApp, and Instagram were the main platforms for distributing the questionnaires among volunteer participants. Ethical considerations of the study including voluntary participation, assent form, anonymity, confidentiality, and the potential for harm were taken into account.
The selection criteria were as follows: (a) willingness to cooperate to fill out the questionnaires, and (b) meeting the age requirements to participate in the study. The exclusion criterion was the failure to complete the questionnaires, meaning that the samples were excluded from the study if they did not answer 20% of the questions.
Data Analysis
We used Pearson’s correlation and stepwise multivariate regression for data analysis in SPSS version 25 software.
Instruments
Family Process Self-Reporting Scale
Samani 15 has developed this scale based on the theoretical model of family process and content. The scale consists of 43 five-point graded questions (strongly agree = 5 to strongly disagree = 1) which have 5 areas; 1—decision-making/problem-solving (items 28–37), 2—coping skills (16–27), 3—cohesion/respect (items 2, 4, and 9–15), 4—communication skills (items 1, 3, 5–8), and 5—religious orientation (items 38–43). The total score of this scale indicates the ability of the family in life skills.
The reliability of this scale has been reported as 0.83 by the retest method (with an interval of 2 weeks to 1 month) and 0.86 by Cronbach’s alpha method. The results indicated the psychometric adequacy of this scale. Cronbach’s alpha coefficients of the subscales of this scale have been reported as sufficient: decision-making/problem-solving (α = 0.86), coping skills (α = 0.88), cohesion/respect (α = 0.76), communication skills (α = 0.79), and religious beliefs (α = 0.79). 16 In addition, the internal consistency of this scale has been calculated for adolescents as sufficient (α = 0.88). 17 In this study, Cronbach’s alpha was calculated to be 0.81.
Self-Report Family Content Scale
Samani 15 has developed this scale based on the contextual model of process and family content. This scale has 38 five-point graded questions (strongly agree = 5 to strongly disagree = 1) which have 7 areas. 1—job and education (items 20 to 24 and 28), 2—time to spend together (items 6 to 9, 11, and 12), 3—financial resources (items 1–5), 4—physical appearance/social status (items 13–16, 18 and 19), 5—physical and mental health (items 34–38), 6—living space (items 29–33), and 7—facilities (items 25–27). The total score is obtained by summing the scores of the items. The total score is ranged between 38 and 190. The items that should be scored reversely are 1, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 18, 20, 21, 22, 23, 25, 27, 28, 31, 32, 33, 37, 38.
Samani 15 used the factor analysis method to determine the validity of the family content scale, as well as the internal validity. The reliability of the family content subscales is reported as sufficient: job and education (α = 0.83 and α = 0.86 respectively), time to spend together (0.77 and 0.88), financial resources (α = 0.78), physical appearance/social status (α = 0.82 and α = 0.83 respectively), physical and mental health (α = 0.72 and α = 0.79), living space (α = 0.79), and facilities (α = 0.82). In addition, the internal consistency of this scale has been calculated for adolescents as sufficient (α = 0.88). 17
Corona Disease Anxiety Scale
This tool has been developed and validated to measure coronavirus anxiety caused by the COVID-19 outbreak. The last version of this tool has 18 items and 2 components of psychological and physical symptoms. Items 1 to 9, measure psychological symptoms and items 10 to 18 measure physical symptoms. The instrument is rated on a 4-point Likert scale (never = 0, sometimes = 1, most of the time = 2, and always = 3). Therefore, the highest and lowest scores that the respondents get on this scale are between 0 and 54. High scores in this questionnaire indicate a higher level of anxiety in individuals. The reliability of this tool was sufficient, using Cronbach’s alpha method for the first factor (α = 0.879), the second factor (α = 0.861), and the whole questionnaire (α = 0.919). The scale indicated a good internal consistency (α = 0.91) and good convergent validity, correlating with the General Health Questionnaire-28 (r = 0.49, P > .01). 23 In addition, the internal consistency of this scale has been calculated for adolescents as sufficient (α = 0.88). 24
Corona Disease Self-Care Behavior Questionnaire
This questionnaire consists of 15 items that assess self-care behaviors during the COVID-19 outbreak on a 5-point Likert scale from 1 (very high) to 5 (very low). For example, I observe hygienic points when going out, such as wearing a mask and gloves. Cronbach’s alpha of the questionnaire in the current study was 0.87. The validity of this questionnaire was evaluated and confirmed by experts. This questionnaire has items that assess factors such as social distance, mask use, and related-washing-hand behaviors. 25 In addition, the internal consistency of this scale has been calculated for adolescents as sufficient (α = 0.88). 26
Results
Descriptive Analysis
The present study included 500 adolescents, of which 62.8% were female and 32.2% were male. The majority of participants were 14 years old and in the sixth grade. Most participants reported living with their families, with family members numbering 4 or fewer. The education level of mothers varied, with 3% being illiterate, 28% having elementary education, 46% having a diploma, and 23% having more than a diploma. The education level of fathers varied as well, with 2.2% being illiterate, 31% having elementary education, 38.8% having a diploma, and 28% having more than a diploma. Among fathers, 24.2% were employees of government organizations, 20.6% were workers, 5.4% were professionals, 21% were teachers, 3% were university faculty, 1% were military, 5.8% were retired, and 19% were unemployed. Among mothers, 26.8% were employees of government organizations, 20.8% were workers, 35.8% were homemakers, 11.4% were teachers, 2.6% were university faculty, and 2.6% were retired.
The average scores of religious beliefs and COVID-19 anxiety were low in the study. The mean score of participants in the study in decision-making/problem-solving was 3.25 for females and 3.26 for males. The total score of family process factors was 3.19. The mean score of males in the decision-making and problem-solving subscales was 3.26 and the total score for process factors was 3.55. The mean score of female adolescents in content factors was 3.02 and in physical and mental health was 3.63%. The mean score for male adolescents in physical appearance and social status was 3.74 and in facilities was 4.53. The average score of anxiety in female adolescents was 4.54 and in self-care behaviors was 4.63. Male adolescents’ mean score for anxiety was 4.35 and for self-care behaviors was 4.19.
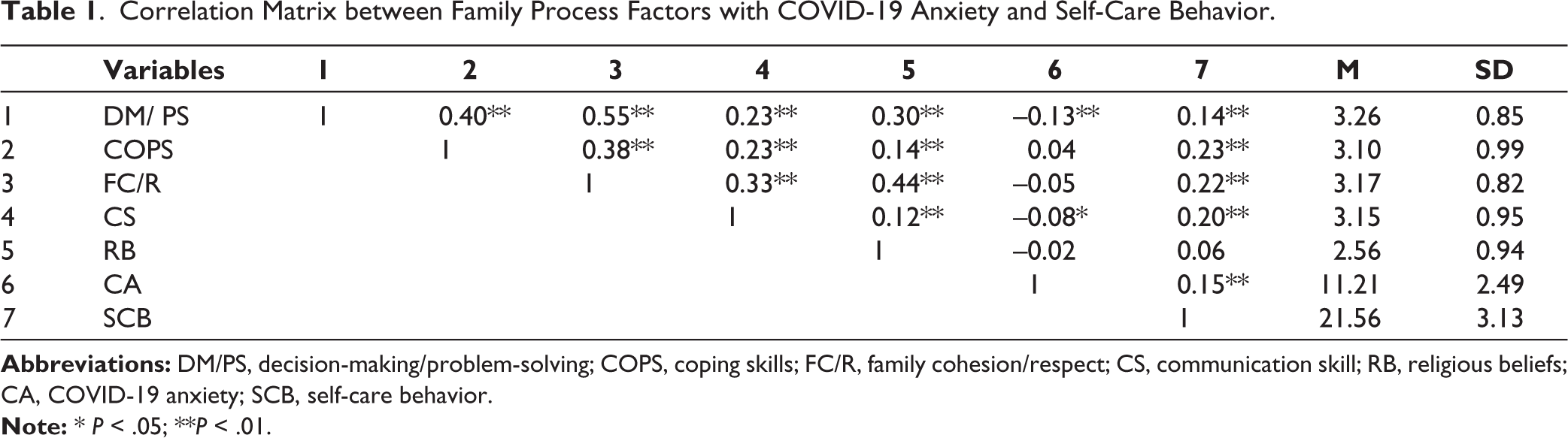
The correlation matrix between the process factors and COVID-19 anxiety in Table 1 indicated that the relationship between decision-making/problem-solving, and communication skills with COVID-19 anxiety was meaningful. The relationship between decision-making/problem-solving, coping skills, family cohesion/respect, communication skills, and religious belief with self-care behaviors was meaningful.
Correlation Matrix between Family Process Factors with COVID-19 Anxiety and Self-Care Behavior.
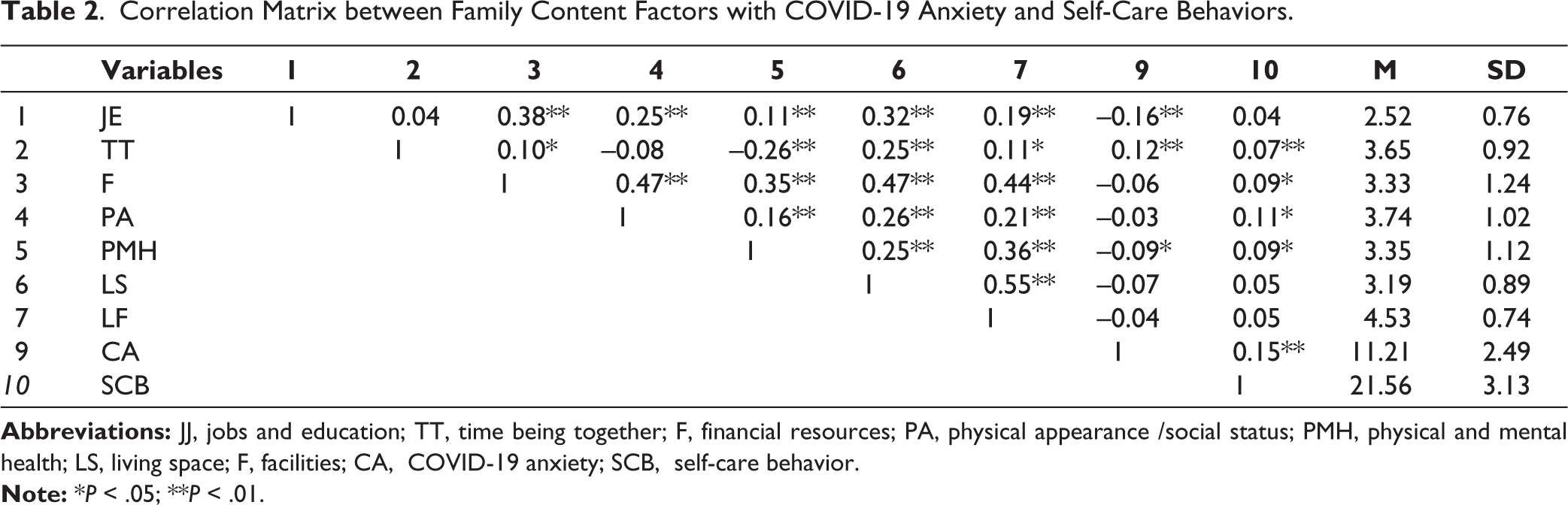
The correlation matrix between family content with COVID-19 anxiety and self-care behavior in Table 2 indicated that the relationship between job and education, and time to be together, with physical and mental health was significant. The relationship between physical appearance/social status, physical and mental health, living space, and facilities with self-care behaviors were significant.
Correlation Matrix between Family Content Factors with COVID-19 Anxiety and Self-Care Behaviors.
Assumptions were examined before regression analysis. The Kolmogorov-Smirnov test was used to evaluate the normality. The results confirmed normality for family process factors (z = 1.41 and P = .06), family content factors (z = 1.26 and P = .09), and COVID-19 anxiety (z = 1.33 and P = .06), and self-care behaviors (z = 1.06 and P = .21). The variance inflation factor obtained for family process factors was (1.44), and for the family, content factor was (1.44). The results showed that there was a linear relationship between the predictor variables. The results of the eigenvalue index also did not indicate a linear relationship between the predictor variables. Status index values also indicated the absence of a linear relationship between predictor variables.
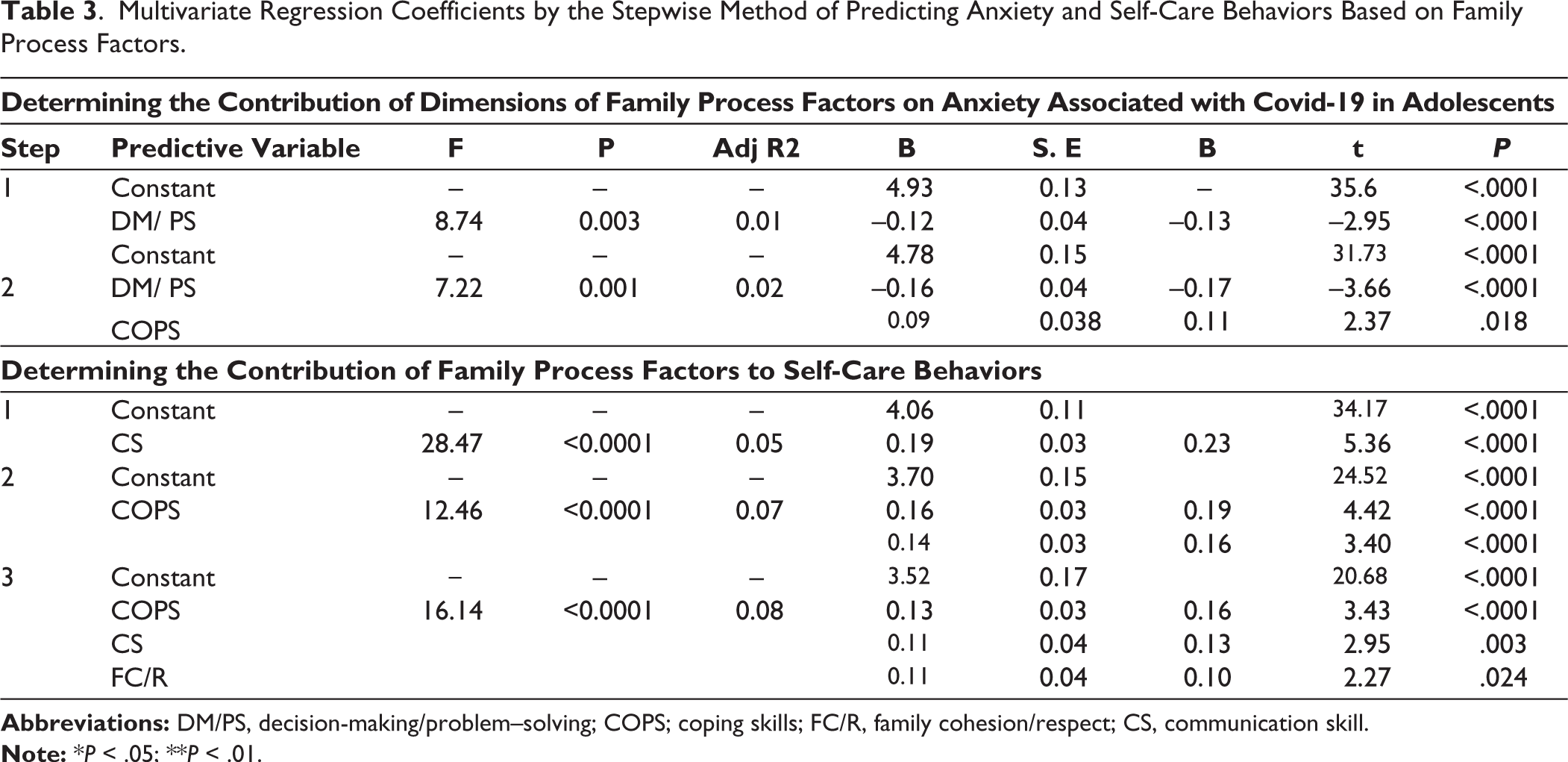
The results of Table 3 showed that decision-making/problem-solving and coping skills could predict 0.02 of changes related to COVID-19 anxiety. The regression coefficients showed that decision-making/problem-solving (β = –0.17, t = 3.66) and coping skills (β = 0.11, t = 2.37), could explain significantly the variance of family process factors. The results indicated that the share of decision-making/problem-solving is stronger than coping skills. The results showed that coping skills, communication skills, and family cohesion/respect were able to predict 0.08 changes in self-care behaviors related to COVID-19 in 3 steps. Regression coefficients showed that coping skills (β = 0.16, t = 3.34), communication skills (β = 0.13, t = 2.95), and family cohesion/respect (β = 0.10, t = 2.27) could significantly explain the variance of family process factors. The results showed that coping skill was a stronger predictor than communication skills and family cohesion/respect.
Multivariate Regression Coefficients by the Stepwise Method of Predicting Anxiety and Self-Care Behaviors Based on Family Process Factors.
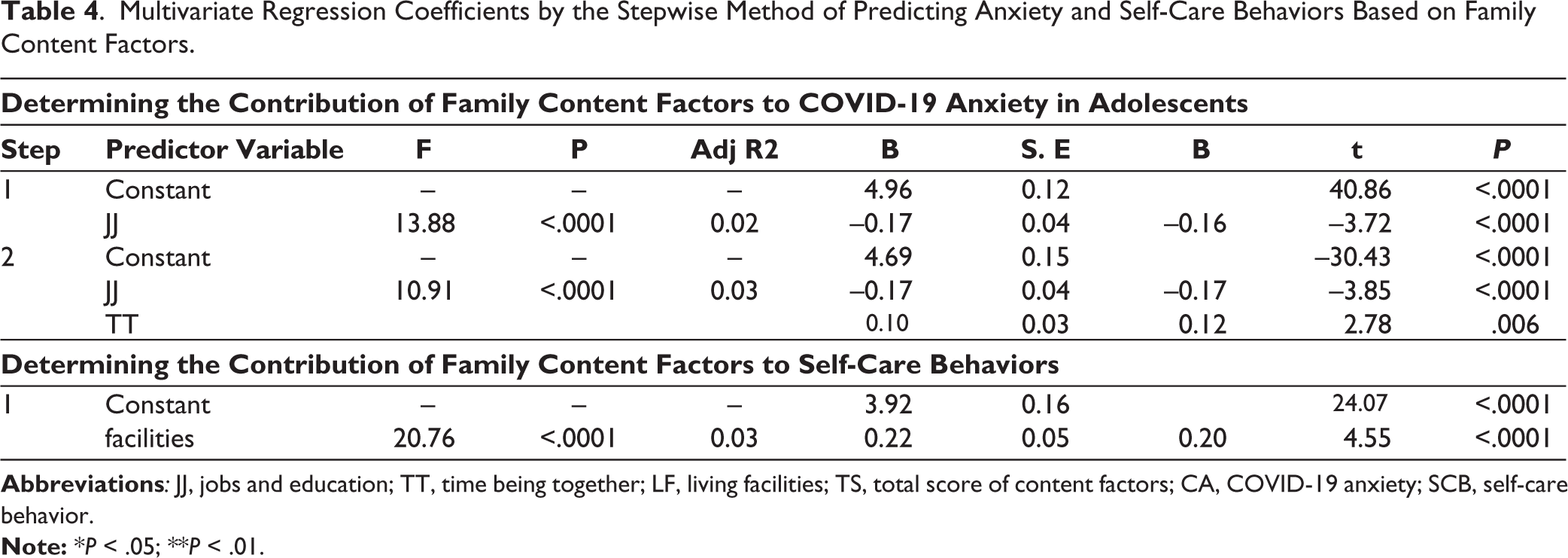
The results of Table 4 showed that job/education and time to be together were able to predict 0.03 of the changes related to COVID-19 anxiety. The regression coefficients showed that job and education (β = –0.17, t = 3.85), and time to be together (β = 0.12, t = 2.78), could significantly explain the variance of family content factors. The results showed that the share of job/education in predicting was better than the time to be together. Other results showed that among the components of family content factors, facilities were able to predict 0.03 of the changes related to self-care behavior. Regression coefficients showed that facilities (β = 0.20, t = 4.55) could significantly explain the variance of family content factors.
Multivariate Regression Coefficients by the Stepwise Method of Predicting Anxiety and Self-Care Behaviors Based on Family Content Factors.
Discussion
The results of regression analysis indicated that decision-making/problem-solving and coping skills predicted COVID-19 disease anxiety, respectively. These results are in line with other studies which indicated that problem-solving and decision-making skills can lead to less anxiety. 26 Furthermore, this finding is in line with other studies that emphasize the role of the family in reducing the anxiety of adolescents.17–18 According to the family process model, healthy families are stronger in problem-solving and decision-making skills compared to unhealthy families. 15 Families who have good decision-making skill share more information and are more aware of each other’s plans. Problem-solving and decision-making skills include a set of abilities that will increase compatibility and efficient behaviors; therefore, families with stronger skills in problem-solving/decision-making accept their social role responsibilities without hurting others or themselves and cope efficiently with COVID-19 anxiety. 27 The onset and persistence of symptoms of the disorder in family members are due to repeated use of dysfunctional solutions. Therefore, with increasing skills like problem-solving/decision-making and coping skills, the incidence of anxiety in family members, and consequently in children and adolescents, can be reduced. 28 These skills can make the environment of the family safe and lead to safe attachment styles and consequently less anxiety. 19
Another finding of this study indicated that some of the family process variables, including coping skills, communication skills, and cohesion/respect could predict self-care behaviors during the COVID-19 outbreak, respectively. This finding is in line with studies that indicate that family-related factors can impact the self-care of adolescents.20–21 Families equipped with effective communication skills, family cohesion and respect, and coping skills tend to be more united and supportive of each other. They are better equipped to face difficulties and use effective strategies to overcome challenges. In a safe and supportive family environment, adolescents can communicate their worries and concerns and use the best coping styles to deal with stressors such as the COVID-19 pandemic. Moreover, a healthy family environment can help adolescents feel valued and important, which can motivate them to take care of themselves. When families prioritize communication, respect, and coping skills, they create a positive and supportive atmosphere that helps adolescents feel more secure and confident in managing their anxiety and stress. This, in turn, can lead to better mental and physical health outcomes for adolescents, both during the pandemic and beyond.
The results also showed that among the components of family content factors, job and education, and time to be together could predict COVID-19 anxiety. Furthermore, higher literacy can decrease anxiety during the COVID-19 outbreak. 29 The family content model suggests that families with optimal job and education situations tend to create a more satisfying environment due to their increased literacy, awareness, and better financial situation. Members of such families may feel a sense of security and pride in their families and can rely on them for support, especially during the COVID-19 outbreak. This supportive atmosphere can help reduce anxiety levels and provide a feeling of safety for adolescents. When families spend more time together, it can increase the feeling of security in adolescents and help them express their feelings and thoughts more openly. This mutual understanding can help reduce anxiety levels among family members, particularly adolescents. Overall, our analysis suggests that families with better job and education situations, and who spend more time together, tend to experience less anxiety among adolescents. This finding is particularly important during the COVID-19 outbreak, where many people have lost their jobs and faced financial difficulties. By prioritizing job and education opportunities and spending quality time together, families can help create a supportive and secure environment, which can help reduce anxiety levels and promote better mental health outcomes for adolescents.
Our analysis showed that, among the family content factors, facilities were able to predict self-care behaviors related to COVID-19 among adolescents. Self-care is a voluntary act that is essential for maintaining personal and public health, and it is a responsibility that individuals have towards themselves, their families, and their communities. During the COVID-19 pandemic, the importance of self-care has been emphasized through widespread media campaigns, resulting in an increase in the number of people taking care of their health and that of their family members. Families equipped with factors such as job opportunities, education, financial stability, and physical resources are more likely to engage in self-care behaviors. Having access to facilities such as clean water, sanitizers, and personal protective equipment can make self-care easier and more effective. Therefore, families that are well-equipped with these resources are more likely to engage in self-care behaviors that can help protect themselves and their loved ones from COVID-19.
Limitations and Clinical Implications
One limitation of this study is that it only includes adolescents from Isfahan City in Iran, which may limit its generalizability to other communities, age groups, and clinical samples. Additionally, this study was conducted during the COVID-19 pandemic, and the findings may not apply to other periods.
Despite these limitations, the results of this study have important clinical implications for healthcare professionals. Clinicians can use the results of this study to develop preventive programs that help reduce anxiety among adolescents during COVID-19 and future outbreaks. Specifically, interventions that focus on improving decision-making/problem-solving and coping skills, as well as communication skills and family cohesion/respect, can promote self-care behaviors in adolescents and reduce anxiety levels.
The findings also suggest that families with better education and financial resources may experience less anxiety among adolescents, highlighting the need for prevention intervention programs for low-income, less educated, and families with low social status. For severe cases of anxiety, family therapy intervention programs may be necessary.
In summary, the results of this study have important clinical implications for healthcare professionals. By promoting self-care behaviors, improving coping skills, and addressing family-related barriers to self-care, clinicians can help reduce anxiety levels among adolescents during COVID-19 and future outbreaks.
Footnotes
Acknowledgements
We would like to thank all the participants of the study for their valuable time and help.
Authorship Statement
All authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, and revision of the manuscript, and approve the manuscript and its submission to this journal.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed assents were received and obtained respectively before initiating the study from all participants. The study was accorded Ethical Committee Approval vide Ethics Committee (Arak Islamic Azad University) No. 1212943229896911399162336634, dated February 9, 2021.
Written/Verbal informed consent was taken from all the participants.
The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.