
Abstract
Introduction:
Despite having innumerable literatures, there has been dearth of comprehensive model of the manifestation of non-suicidal self-injury (NSSI).
Aim and Objectives:
The current study aims to construct a statistically validated model to explore the theoretical connections and the pathway to NSSI among female adolescents.
Material and Method:
A model was proposed based on the constructs empirically associated with NSSI. The research aims to explore the direct effects of external shame, hated self, and self-compassion on NSSI, and whether this relationship is mediated by borderline personality traits and menstrual phase. A total of 168 female adolescents completed the survey, including informed assent from the adolescents. The Other as Shamer Scale-2, the Forms of Self-Criticism/Self-Reassuring Scale, Self-Compassion Scale, the Risk-Taking and Self-Harm Inventory for Adolescents, and Borderline Personality Features Scale for Children were administered to the participants. Analysis of data involved descriptive statistics and path analysis.
Result:
The pathway shows hated self, disturbed intrapersonal relationship, and the inability to direct compassion for self may increase NSSI. Borderline personality traits and premenstrual dysphoria form indirect but contributory factors to strengthen the association between internal traits and NSSI.
Conclusion:
Thus it may be concluded from the present finding that external shame has significant negative effect on self-compassion and external shame has a significant positive effect on hated self. Also, self-compassion has a significant negative effect, and hated self as well external shame have significant positive effects on borderline traits. Thus, exploring this path would help to plan a suitable preventive action.
Introduction
With the incessant multifaceted complexities thrown by various life circumstances, including growing demands from environment as well as own selves, adolescents often find it too cumbersome to cope. Continuous pressure of establishing their “unique” identity, by dint of looks and other endeavors, a sense of rejection, a sense of not being good enough and lagging behind, often lead to insurmountable negativity, thereby developing frustration. That is, self-esteem, control, and mastery over situation get thwarted, marshalling depression, and get manifested through self-injurious behavior, 1 or non-suicidal self-injurious (NSSI) behavior.
NSSI is defined as the direct and intentional destruction of one’s own body tissue, in absence of suicidal intents and for purposes not culturally sanctioned, 2 such as cutting and burning. And it is a matter of grave concern that the average age of onset of NSSI ranges consistently between 12 and 16 years old. 3 The most alarming fact is: It is gradually getting augmented globally, and India is not an exception. In a recent study, 33.8% self-reported NSSI was revealed among adolescents and young adults. 4 However, it is yet to explore whether the risk factors associated with NSSI is extrinsic or intrinsic in nature or a combination of both as it would help to design a suitable intervention program. Though extensive literatures on the contributing factors of NSSI are available, there is dearth of research evidence in regard to their interaction, as previous studies barely focused on the interaction among the variables like shame, borderline traits, premenstrual dysphoria, and most importantly self-compassion as the protective factor in NSSI. The current study therefore delves to ponder upon resolving this dilemma regarding how these variables are related so that appropriate intervention program for NSSI can be designed.
While exploring the factors associated with NSSI, the experience of shame seems to have an important contribution which stems as a way of submission as well as withdrawal mechanism in order to deal with the early experiences of being criticized, judged, or viewed negatively by significant others which eventually led to negative self-evaluation. 5 And such combating procedure gives rise to both external and internal shame dimensions because when one encounters oneself as existing in a negative manner in the “psyches” of others, one may participate in an internal disgracing and degrading process that includes a “cruel” self-accusing and self-persecutory demeanor towards oneself, thereby resorting to defensive submissive strategies. 6 In other words, external shame originates outside the self, involves a distressing awareness that others view the self negatively, and internal shame originates inside the self, involving self-criticism and negative self-evaluation. 7 Thus, self-criticism may be another determining factor of NSSI. Furthermore, self-criticism is found to be a mediator between emotional abuse and NSSI. 8
Moreover, the harmful impact of such self-depreciating attitude tends to exacerbate the psychological vulnerability, thereby reducing the self-soothing as well as self-caring abilities, 9 which may be regarded as fear of compassion. Additionally, fears of compassion for the self and of receiving compassion from others are linked to a range of psychopathological indicators, such as self-criticism, insecure attachment, alexithymia, fears of happiness, lower levels of empathy and mindfulness, increased symptom of depression, anxiety, and stress. 10
Now the question still remains whether the nexus of hated self, which includes external shame and fear of compassion, are only operative in the manifestation of NSSI or there are other contributory factors allied with hated self, leading to NSSI. An important consideration here is the presence of borderline personality, which is essentially characterized by immense self-invalidation. Evidence shows that 95% of adolescents having borderline personality disorder (BPD) reported to have NSSI. 11 So, the presence of borderline traits may be a precursor to NSSI. Similar research revealed that among the individual with BPD symptoms, past suicidality, impulsivity, chronic emptiness, and identity disturbance were each significantly and positively associated with lifetime history of NSSI. 12
Among other factors which affect NSSI in female adolescents, one major factor contributing to mood swings, emotional dysregulation, and consequently NSSI in females may include the menstrual phase. Research suggested that onset of menarche, irregular periods, and period pain appear were associated with increased risk of NSSI. 13 Menstrual problems have significant influence on quality of life of adolescents. 14
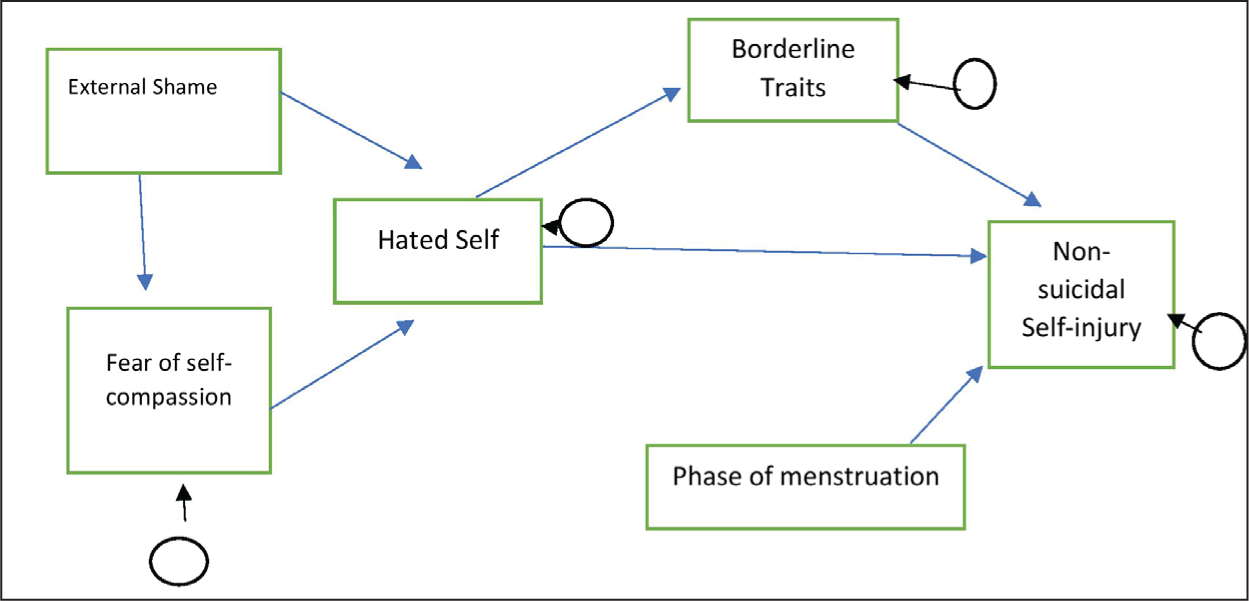
The role of external shame, self-criticism (hated self), self-compassion, borderline personality trait, premenstrual dysphoria on NSSI among female adolescents was empirically and theoretically explored, but as a whole there is no statistically validated model considering the above-mentioned factors. Therefore, the present study aims to explore the theoretical connection of such a statistically validated model (Figure 1).
Represents the Proposed Model of NSSI to be Validated by Path Analysis.
Methods
The current study aims to explore whether the 3 internal traits, ie, external shame, hated self, and self-compassion, have a direct effect on the frequency of NSSI, and whether these relationships are mediated by borderline personality traits and menstrual phase.
Firstly, the study aimed to investigate whether there exists any direct effects of external shame and self-compassion on self-criticism (hated self) among participants with NSSI and to explore whether external shame has an indirect effect on self-criticism (hated self) mediated by self-compassion (as a protective component).
The second objective of this study was to investigate whether self-criticism (hated self) has direct effects on frequency of NSSI among adolescents and to explore if external shame and self-compassion have an indirect effect on the frequency of NSSI mediated through self-criticism (hated self).
Finally, the study also aimed to determine whether borderline personality traits and any specific phase of menstrual cycle have any direct effect on frequency of NSSI and if self-criticism (hated self) has any indirect effect on the frequency of NSSI mediated through and borderline personality feature and any specific phase of menstrual cycle among female adolescents.
Sample
The participants comprised 168 female school students, with minimum education till 10th standard, who committed NSSI at least once in past life, residing in Kolkata, aged 16 to 18 years, did not have any present or past history of diagnosed psychiatric disorder.
Stratified Purposive Sampling was followed in this study, where population was divided into sub-groups (or strata) and purposive sampling was used in each of the sub-group. However, for zonal representation of different areas of Kolkata (North, South, East, West [Howrah]), the list of postal areas spread over Kolkata was prepared, and a zone-wise mapping was done. From each zone, participants were chosen purposively. They were given the informed assent form for the study and those who agreed and met the inclusion criteria defined for the study were included as prospective subjects. This group was again randomly shortlisted to include approximately equal number of subjects spread over the 5 zones. From each zone, initially 162 to 167 participants were approached, of which, a total of 720 participants were included in the study. They were provided with the information schedule including socio-demographical detailing along with information regarding presence/absence of NSSI. From the171 participants reported having committed NSSI act, 3 were excluded from the present study since self-injury in these respondents was reported with a suicidal intent. The final sample therefore consisted of 168 female adolescents, who were contacted for further research work.
Measures
Personal Information Schedule
It included name, age, sex, date of birth, religion, address, education, family income, type of family, area of residence, personal or family history of any chronic, or psychiatric/hormonal illness or any form of disabilities, any significant life event in past one year and past life (if any), any significant event before committing NSSI, age of the participants when first NSSI was committed, phases of menstrual cycle in which NSSI was mostly committed (premenstrual/menstrual/postmenstrual phase), any family history of NSSI, any family history of suicide or diagnosed psychiatric disorder, any significant perceived parental dysregulation, any family history of trauma or mishap.
The Risk-Taking and Self-Harm Inventory for Adolescents (RTSHIA)
It consists of 38 items that assess risk-taking behavior and self-harm. In the present study, items 32 and 33, which assess suicidal ideation and intent respectively, were not included in the overall sum of NSSI and the self-harm subscale was used. In the original study the authors found a very good internal consistency for self-harm dimension (a = 0.93). 15 In this study the self-harm dimension (9 items) presented good internal reliability (a = 0.88).
The Other as Shamer Scale-2 (OAS2)
It is an 8-item shortened version of the Other as Shame Scale and an economic, valid, and reliable measure of external shame. In the original version, OAS2 showed a very good internal consistency (a = 0.85) as well as in the adolescents’ version (a = 0.93). 16 In this study we also obtained a very good internal consistency (a = 0.94).
The Forms of Self-Criticism/Self-Reassuring Scale (FSCRS)
The 22-item self-report questionnaire has internal reliability with Cronbach’s alpha of 0.90 for inadequate self and 0.86 for both hated and reassured self. 17 In this study we only used hated self-subscale which assesses the desire to hurt or persecute the self, and it presented good internal reliability (a = 0.80).
Self-Compassion Scale (SCS)
This short form of the self-compassion scale comprises 12 items and composed of 3 subscales that assess compassion for self, compassion from others, and compassion for others. In the original version the FCself scale had good internal consistency (a = 0.85). 18 In the present study the Cronbach’s alpha was 0.90.
Borderline Personality Features Scale for Children (BPFSC)
The BPFSC an 11-item questionnaire, which is developed from the BPD scale and consists of 24 items measuring borderline personality features in childhood (for ages 9 and older, including adolescents). It is rated on a 5-point scale ranging from not true at all (= 0) to always true (= 4). Internal consistency was satisfactory (Cronbach’s α = 0.78). 19
Procedure
Assent forms were given and nature of the study was explained to the participants. At the beginning of the study, all participants were informed about the purposes of this research. Also, the authors of this study took into account the participants’ anonymity and confidentiality. Ethical clearance was taken from the Institutional Ethical Committee in accordance with the Declaration of Helsinki 1975, revised in 2000. Then, the information schedule and the RTSHIA were administered among 720 adolescents belonging to the age group of 16 to 18 years, staying in Kolkata. Of the 720 participants, 168 adolescent females were included in the final sample for the study based on the inclusion criteria, and they were contacted for further proceedings. Rest of the scales were then administered. The participants were given the required instructions and were asked to answer the questionnaire accordingly. Cronbach alpha was found out for all the above mentioned scales, to find out the internal consistency of the scales. After collecting the data, they were suggested to meet any psychiatrist or clinical psychologist, or if they face any urge to commit self-injury, to at least inform the researcher or any friend, rather than committing NSSI.
Statistical Analysis
Data were tabulated in SPSS 22. Then descriptive statistics (mean, SD, percentage of occurrences) were used. Then, path analysis of structure equation modelling using STATA (Software for Statistics and Data Science)] software 20 for formulating the proposed model with significant/non-significant path coefficient. Here, all the variables are manifested variables in the path analysis model. The process starts by specifying a model based on pre-defined model which was mentioned in introduction, and then 2 or more alternative models were formulated and compared in terms of model fit. Chi-square for goodness of fit was used to evaluate the best fitting model with the saturated model. The chi-square value close to 0 indicates little difference between the expected and observed covariate matrices, with the probability level more than 0.5 meaning the absence of meaningful variance.
Results
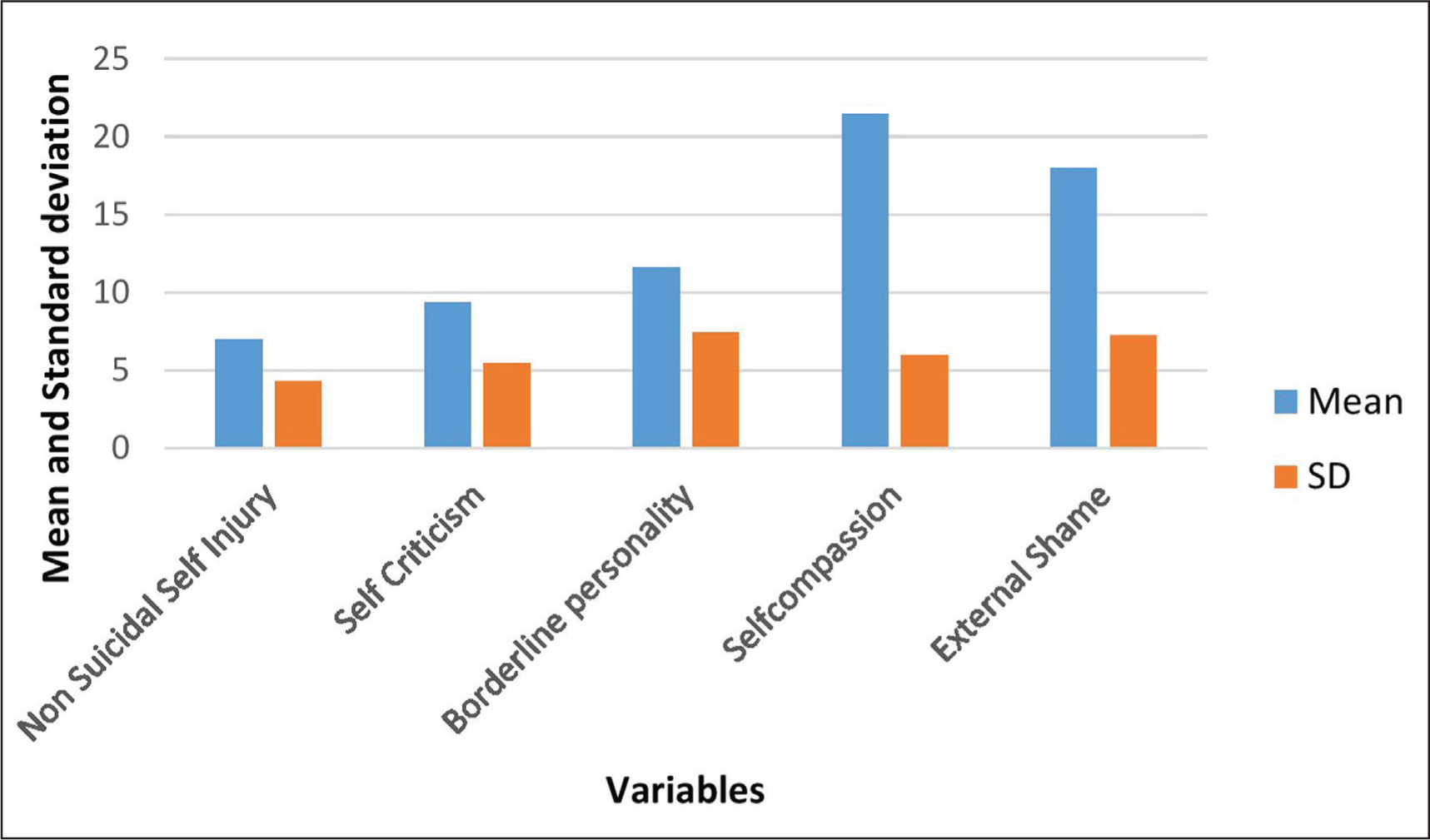
The results of the descriptive analysis of the study variables, including self-compassion, external shame, hated self, borderline personality traits, menstrual phase, and NSSI are summarized in Table 1 and graphically represented in Figure 2.
Descriptive Statistics of Variables Associated with Non-suicidal Self-injury.
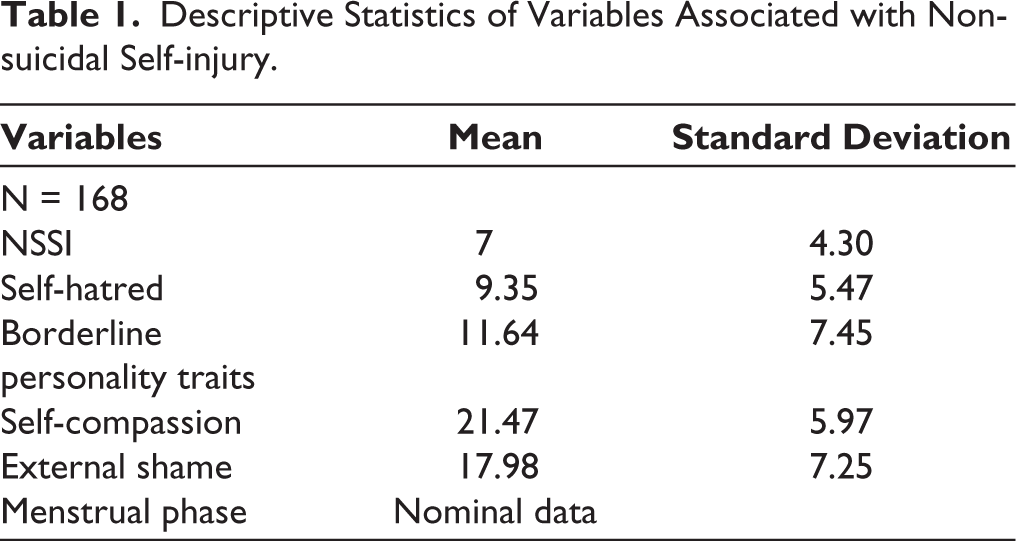
Showing the Variables and Their Corresponding Means and Standard Deviation Values.
The final path model had a good fit, as reflected by the widely reported fit indices. It is shown in Figure 3. The fits statistics for both hypothesized and final model are given in Table 2.
Final Model (Least Discrepancy Model from Saturated Model) of NSSI.
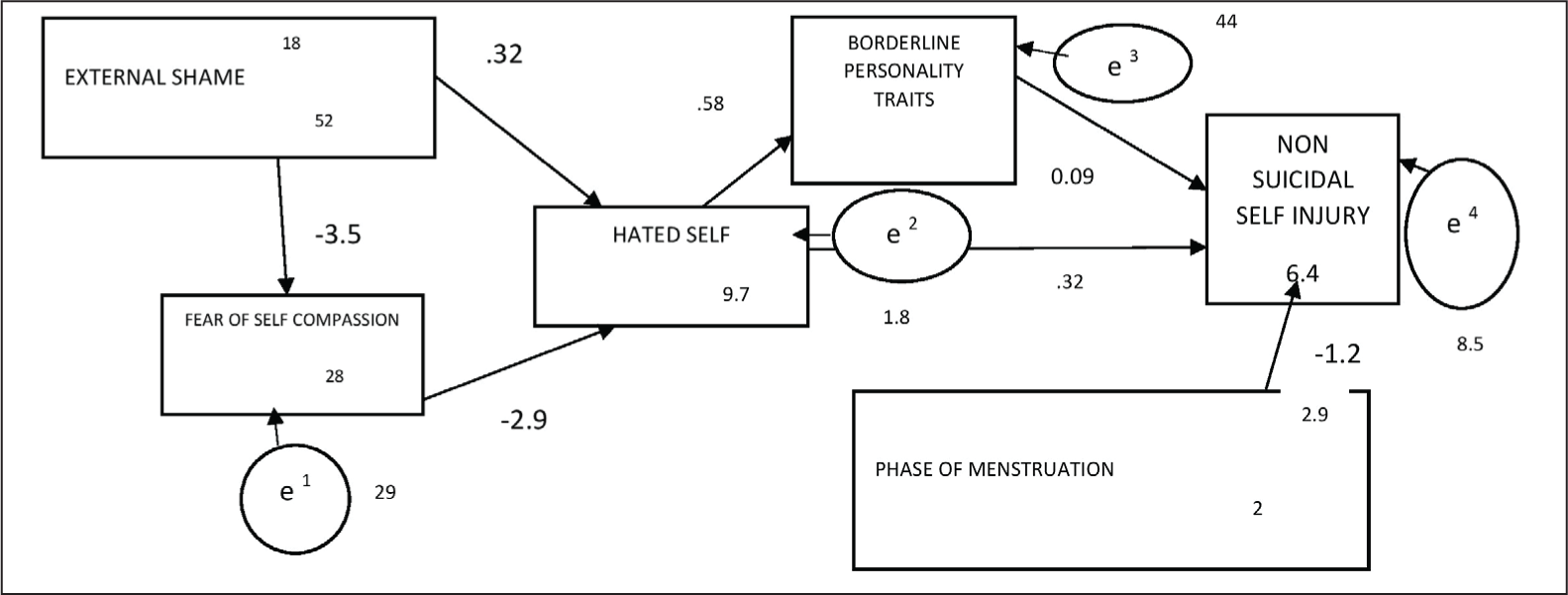
Table Showing the Fits Statistics for both Hypothesized and Final Model.

It can be observed from the table that the modified and final model had better fit than the hypothesized model. It can be seen that the final model had an excellent CFI as well as TLI, which reflects that the model has excellent fit compared to a possible model with poor fit. Research showed that RMSEA should not be higher than 0.08 to indicate good fit. 21 The final model had RMSEA in the acceptable range, with P-close value indicating close fit. Further, the path coefficients based on the final model is given in Table 3.
The final path model showed direct negative path from external shame on self-compassion (β = –0.35, P < .01). Also, direct positive and negative paths were revealed respectively from external shame (β = 0.32, P < .01) and self-compassion (β = –0.28, P < .01), on hated self, which, in turn, had direct positive effect (β = 0.58, P < .01) on borderline traits. Finally, both hated self and borderline traits had direct positive effects (β = 0.32, P < .01; β = 0.09, P < 0.05, respectively), while menstrual phase had direct negative effects (β = –1.18, P < .01), on NSSI.
As for the indirect effects, external shame had positive indirect effect (β = 0.10, P < .05) on hated self, whereas self-compassion and external shame had indirect effects, negative and positive respectively (β = –0.17, P < .01; β = 0.25, P < .01, respectively), on borderline traits. Self-compassion had indirect negative effect (β = –0.11, P < .01), whereas external shame and hated self had indirect positive effects (β = 0.16, P < .01; β = 0.09, P < .05, respectively), on NSSI.
Overall, it can be said that external shame has a significant negative effect on self-compassion (β = –0.35, P < .01). Self-compassion has a significant negative effect, and external shame has a significant positive effect on hated self (β = –0.28, P < .01; β = 0.42, P < .01, respectively). Also, self-compassion has a significant negative effect, and hated self as well external shame has significant positive effect on borderline traits (β = –0.17, P < .01; β = 0.58, P < .01; β = 0.25, P < .01, respectively). Finally, hated self, external shame, and borderline traits showed significant positive paths to NSSI, while self-compassion and menstrual phases showed significant negative paths to NSSI (β = 0.41, P < .01; β = 0.16, P < .01; β = 0.09, P < .05; β = –0.11, P < .01; and β = –1.18, P < .01, respectively). Thus, the mediation analysis showed the presence of both direct as well as indirect effect of different variables on NSSI. Additional information regarding the direct and indirect effects of self-compassion, hated self, external shame, borderline traits, and menstrual phase on NSSI are shown in Table 3.
Table Showing the Path Coefficients Based on the Final Model.
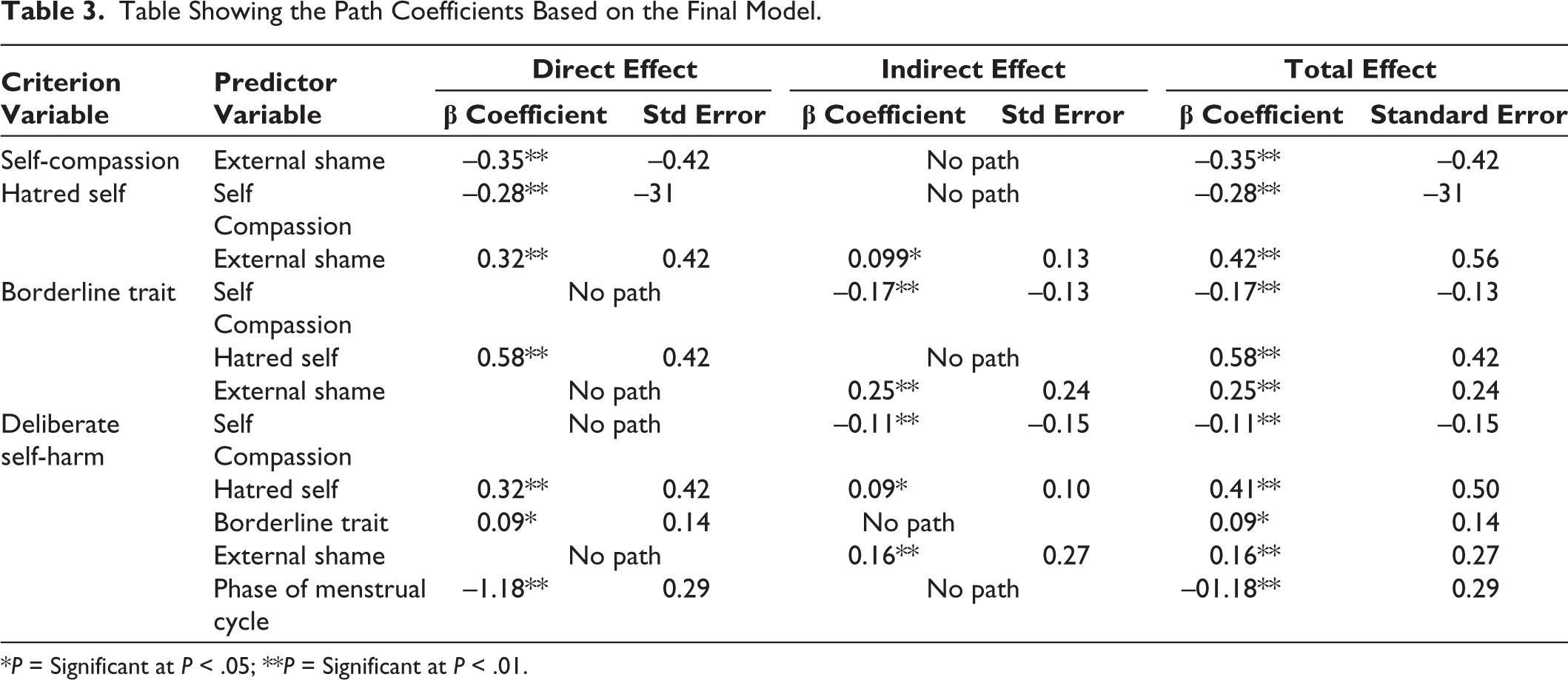
*P = Significant at P < .05; **P = Significant at P < .01.
Discussion
NSSI has become a relatively prevalent problem, especially among the adolescents as evidenced by the high prevalence rates. 22 There is a plethora of studies which have identified the factors involved in the engagement of NSSI; however little is known about the process involved through which the factors have an impact on the individual. Therefore, the main aim of the present study is to generate a model to predict the pathway for the NSSI behavior among adolescents. The study especially explores the pathway of external shame and self-compassion through self-criticism (hated self) leading to NSSI.
With respect to the current findings, it was observed that external shame was directly associated with the hated self and indirectly associated while being mediated through lack of self-compassion. Fear of self-compassion indicated direct association with NSSI. Hated self was found to have direct association with NSSI and indirect association as mediated through borderline personality traits and menstrual phase, which act as moderators in bringing about engagement in NSSI. In other words, adolescent females with high external shame, self-criticism (hated self), and lack of self-compassion may have a high tendency to inflict injury upon themselves which gets aggravated if they also possess high borderline features and if they experience premenstrual dysphasia, then propensity towards impulsive actions also gets evident.
Shame is known to have a debilitating effect on human psyche, especially during adolescence as it is the pivotal period for self-presentation and self-esteem. Thus, individuals who are pummeled by external shame may have low self-esteem and develop negative cognitive schemas based on other’s evaluation of him/her. Additionally, these maladaptive self-schemata, indwelled by detrimental interpersonal interaction, often get activated by later negative life conditions. 23 The current study also explored a direct pathway of external shame leading to self-criticism (hated self) which acts as a mediator to NSSI. Individuals high on external shame engage into self-harm when compelled by other factors such as hated self. It is observed that self-harm was significantly associated with forms and functions of self-criticism, shame, and feelings of inferiority (low social rank). 24 The self-persecuting function of self-criticism was especially linked to self-harm, depression, and anxiety. The variable like fear of self-compassion, however, complicates the alley, i.e., the indirect pathway from external shame to hated self via fear of self-compassion. This supports the view that when individual high on external shame also show a lack of self-compassion, it consequently leads to an aggravation of hated self. This finding is supported by a previous study, where it was found that a lack of self-compassion indirectly predicted NSSI while self-criticism (hated self) was strongly associated with NSSI. 25 In Compassionate Mind Training for people with high shame and self-criticism, it is observed that self-warmth and self-acceptance, which are essential facets of self-compassion, significantly reduced depression, anxiety, self-shame, inferiority, and submissive behaviour. 26
The situation gets irked up if there is presence of borderline personality traits. In the present finding as well, it has been revealed that hated self has a direct association with NSSI, and indirect one as mediated through borderline personality traits. Behavioural dysregulation and self-criticism, 2 significant characteristics of borderline personality, often lead to self-harming behaviour. 27 Furthermore, another study had reported that emotional dysregulation, along with affective liability and intense aggression in people with borderline personality traits, increases the likelihood of NSSI. 28 Likewise other studies also show that individuals with the borderline features show more severe depressive symptoms and suicidal tendencies than individual control. 29
Besides borderline personality traits, another factor which plays a significant role in promoting NSSI is the menstrual phase of female adolescents. Changes in hormones, like adrenocorticotropic hormone, which is one of the controlling factors of mood, may contribute to the cyclic occurrences of anxiety, aggressiveness, and irritability reported by patients with premenstrual symptoms. 30 Suicidal ideation and suicide attempts are associated with specific signs or symptoms of premenstrual syndrome, like low back pain, aggressiveness, desire to eat certain food or eat a lot, and guilty feeling. 31 It is also found that suicidal attempts were more common among females of 14 to 21 years, with the presence of situational reactions during menstrual phase. 32 Thus, the query which had started the quest for the present research, that how shame, borderline traits, premenstrual dysphasia interact, and most importantly the role played by self-compassion as the protective factor in NSSI, has been addressed, by exploring a previously less known pathway.
However, it is to be noted that the present study could not take into consideration the rate and severity of NSSI. Besides, the present study did not explore the role of other potential factors, such as impulsivity, pain tolerance level, and the role of family dynamics.
Despite being a pertinent issue, sociodemographic variables were not treated as covariate, which can be incorporated in future work. Future researches are required to investigate these variables, along with taking into account the social desirability aspect of the adolescents. The model may also be tested cross-culturally to validate the current findings.
Conclusion
Adolescence is a critical stage of life which summons on innumerable psychological turmoil. And the circumstances deteriorate when there is presence of self-hatred and criticism from others, thereby leading to self-injurious behavior. In this context, the present study contributes to the existing literature on NSSI by empirically revealing the pathways through which the belief that one is perceived negatively by others, disturbed intrapersonal relationship, and the inability to direct compassion for self may increase NSSI. Borderline personality traits and premenstrual dysphoria form indirect but contributory factors to strengthen the association between internal traits and NSSI. These findings provide useful insight into providing proper prevention as well as intervention measures to be undertaken for reducing NSSI in adolescents. As suggested by the current findings, these actions should address not only interpersonal difficulties but also intrapersonal relationship, along with development of positive and adaptive schemas since childhood.
The study was accorded with Ethical Committee Approval via Institutional Bio Ethics Committee for Human, University of Calcutta, on June 12, 2019 (No EC/2019/21).
Assent forms were given and nature of the study was explained to the participants. At the beginning of the study, all participants were informed about the purposes of this research. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki 1975, as revised in 2000.
Footnotes
Acknowledgements
The authors would like to appreciate all the participants and the research staff who kindly helped during this research. The authors received no specific funding for this work.
Author Contributions
All the authors are affiliated with prestigious institute. The manuscript has been read and approved by all the authors, the requirements for authorship as stated earlier in this document have been met, and each author believes that the manuscript represents honest work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study, from all participants.