
Abstract
Objective:
To study complementary effect of sleep training program in children with attention deficit hyperactivity disorder (ADHD) receiving tablet methylphenidate with respect to sleep, quality of life (social, behavioral, emotional, and executive functioning of children), and their parent’s emotional state.
Methods and Materials:
It was a comparative and prospective study, and it was conducted in child mental health services of a tertiary care municipal hospital. The children (age 8−12 years) were diagnosed with ADHD using DSM 5 criteria. The children’s sleep habit questionnaire (CSHQ) and Kiddie-SADS-PL questionnaire (K-SADS-PL) were used to select 100 consecutive participants (parent–child dyad). They were randomly equally divided into two groups: A and B. Semi-structured proforma was filled and different scales were applied for children; these scales include Strengths and Difficulties Questionnaire (SDQ), Pediatric Quality of Life Inventory (PQLI), Stroop test (ST) and Verbal fluency test (VFT), and to parent-Depression Anxiety Stress Scale-21 (DASS-21). The participants in group A received a validated sleep intervention and the scales were reapplied after 12 weeks. We used Chi-square test, paired t-test, unpaired t-test, Wilcoxon signed-rank test, Mann-Whitney U test, Spearman’s correlation test, and logistic regression analysis for data analysis. p-Value <.05 was taken as significant. SPSS version 20 software was used for data analysis.
Results:
We found significant post-intervention improvement in sleep, quality of life, social, emotional, behavioral, and executive functioning in children and emotional factors in parents.
Conclusion:
The combination of sleep intervention and tablet methylphenidate were more effective in improving these factors.
Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most common neuropsychiatric disorders with a male preponderance, which affects children, adolescents, and adults. Sleep problems are common in children with ADHD, and the cause is probably being shared neurobiological pathways. 1 It has been found that medications such as methylphenidate, amphetamine, dextroamphetamine, and others have an effect on sleep. These drugs are sympathomimetic stimulants and studies with them and methylphenidate alone have shown mixed results where they either reduce total sleep time, increase sleep-onset latency, and reduce sleep efficiency or they improve sleep quality by decreasing nocturnal activity or have no effect on sleep quality and decrease night awakenings.1–3
Adequate sleep is required for important cognitive and psychological functions such as learning, memory, attention, mathematical skills, and impulse control.4,5 In addition to the core ADHD symptoms, sleep problems lead to worsening behavior, decreased quality of life, and poor daily functioning. 6 Studies on effects of sleep problems on executive functions of children showed difficulties with priority and time management, planning and organization, and their improvement with ADHD medications.7,8 Others have reported that adequate sleep in children with ADHD helps in cognitive function, 9 emotional and behavioral performance, 10 and impulse control. 11 This highlights the need to address sleep problems in children with ADHD.
Prior research have studied the effect of sleep intervention resulting in improvement in sleep, behavior, emotional and social functioning, quality of life, and daily functioning.6,12 None of the studies have been comprehensive and they have failed to study the improvement in cognitive functions of the children and the impact of sleep disturbances on parents. With this gap, we planned a study on the effect of a study on the effect of a sleep intervention on sleep, ADHD symptoms, executive functions, emotional, behavioral, and social func- tioning of children and parent’s emotional state.
Methodology
Study Design and Participant Characteristics
It was a comparative and prospective study, and it was conducted in child mental health services of a tertiary care municipal hospital in a metropolitan city of Mumbai, India. We included children who were 8−12 years of age, diagnosed as ADHD as per DSM-5 criteria, were receiving methylphenidate and maintained on a responsive dose (10−30 mg) for at least three months. Children whose score on Children’s sleep habit questionnaire (CSHQ) was >41, who assented, and their parents agreed to a written informed consent were involved in the study. We excluded children having neurological diseases, co-morbid psychiatric disorders, which could impact sleep, such as autism spectrum disorder, intellectual disability, depressive and anxiety disorders, various medical or surgical conditions known to adversely affect sleep, such as asthma and obstructive sleep apnea, and those who are already on treatment for sleep complaints.
Procedure
Institutional ethics committee (Ethics committee for academic research projects, PG academic committee, TNMC and BYL Nair Ch. hospital) approval (ECARP/2015/03) was received on 27/02/2015, written informed consent of parents and assent of children were obtained, and principles related to Declaration of Helsinki were followed. Diagnosis of ADHD was made by a senior consultant based on reports from parents, school, observation of child, and using DSM-5 criteria. Comorbidity was excluded clinically and with Kiddie SADS present and lifetime version screening interview (K-SADS-PL). The sleep pattern of all the selected children was assessed by CSHQ and those with score >41 were included in the study. All the participants were randomly divided into two groups using red and blue ribbons; group A having 50 participants who were to receive sleep intervention and group B having 50 participants who would receive treatment as usual. The other scales and tests applied to children were: Strengths and Difficulties Questionnaire (SDQ), Pediatric Quality of Life Inventory (PQLI) parent and child, Stroop test (ST), and Verbal fluency test (VFT). Parents answered the Depression Anxiety Stress scale-21 (DASS-21). Group A participants received the sleep intervention over a period of 12 weeks. Both the groups were reassessed with the above-mentioned tools 12 weeks after the baseline assessment. The behavioral sleep intervention was also taught to the parents of group B after the study was completed. During the period of study, there was no change in medication dose and addition of other medication.
Measures
Demographic Data Sheet
It consisted of questions related to socio-demographic details and illness variables.
Scales
Children’s Sleep Habit Questionnaire: It is a retrospective 45-item parent questionnaire. There are eight subscales: (1) Bedtime Resistance, (2) Sleep Onset Delay, (3) Sleep Duration, (4) Sleep Anxiety, (5) Night Waking, (6) Parasomnias, (7) Sleep-Disordered Breathing, and (8) Daytime Sleepiness. The score range is 45−135 and cut-off score is 41. It showed adequate internal consistency (p = .78). Test–retest reliability was 0.62-0.79.
13
Stroop Test: This is a test for executive function and consists of two subtasks. The test–retest reliability of scores is robust.
14
We utilized the version from NIMHANS neuropsychological battery, which has been standardized for Indian population.
15
Verbal Fluency Test: In phonological verbal fluency (PVF) test, a single letter is provided and the person has to generate as many words starting with the specified letter (F,A,S) in a specified period of time. It is a reliable test for executive functions with a high co-efficient alpha and test–retest correlations.16,17 We utilized the version from NIMHANS neuropsychological battery for children. In this version, the letters used were “F”, “A”, and “S” for students studying in English or “Ka”, “Pa”, and “Ma” for students studying in Hindi or Marathi. The test–retest reliability of all the tests in the battery falls in the range of 0.53–0.83 and their construct validity is well established.
18
Pediatric Quality of Life Inventory: PQLI is a tool for measuring health-related quality of life in children and adolescents of 2–18 years of age. It has a child self-report and parent proxy-report questionnaire. It consists of 23 items covering four dimensions: physical, emotional, social, and school functioning. Internal consistency reliability for various scores and its validity were found to be acceptable.
19
Strengths and Difficulties Questionnaires: SDQ is an emotional and behavioral screening questionnaire for 4–16 years old. It includes 25 items divided in five scales namely emotional symptoms, conduct problems, hyperactivity/inattentive, peer relationship problems, and prosocial behavior. The reliability and validity of this questionnaire have been found to be adequate with internal consistency of 0.76.
20
Depression, Anxiety, Stress Scale 21: This is a 21-item self-report questionnaire to measure the severity of a range of symptoms common to both depression and anxiety. Each item is scored over a Likert scale of 0 to 3. The total score ranges from 0 to 126. Internal consistency is high with Cronbach’s alphas of 0.94, 0.88, and 0.93 for depression, anxiety, and stress, respectively.
21
Kiddie-SADS-present and Lifetime Version (K-SADS-PL) Screen Interview: It is a semi-structured diagnostic interview to obtain severity ratings of symptoms of psychiatric disorders. The Screen Interview surveys the primary symptoms of the different diagnoses assessed in the K-SAD-PL. The majority of the items in the K-SADS-PL are scored using a 0–3-point rating scale. Its reliability and validity were found to be acceptable.
22
Behavioral Sleep Intervention Module
This behavioral sleep intervention module was designed using previous literature reporting the use of interventions such as sleep hygiene, graduated extinction, scheduled awakenings, faded bedtime with response cost, stimulus fading, and chronotherapy.23,24 Based on common sleep disturbances in ADHD as reported in literature, such as bedtime resistance, delayed onset of sleep, night waking, and daytime sedation,25,26 and based on our experiences, we chose three techniques; they are sleep hygiene, faded bedtime with response cost, and graduated extinction.
Techniques used in behavioral intervention23,24
Sleep Hygiene23,24
Sleep hygiene refers to the arrangement of environmental and behavioral factors preceding sleep. Parents were taught and advised to follow the following practices: (1) Environmental factors: to keep surroundings quiet, dark, and cool, to ensure no access to stimulating activities in the room such as television and computer at least 1 h before bedtime, and to eliminate a visible bedroom clock so as to prevent focusing on time when trying to fall asleep. (2) Behavioral factors: to set a bed and wake time to be followed regularly and strictly, to establish and follow some bedtime habits serving as cues to fall asleep such as brushing teeth and changing clothes, to avoid harsh or bitter conversations with children before sleep time, to avoid excess water or caffeine and heavy meals for 2–4 h before going to bed, to try restrict the use of bed only for sleep and avoid using it for playing, eating, and studying, and to avoid daytime naps.
Faded Bedtime with Response Cost23,24
This technique has been found useful in increasing sleep duration, decreasing frequency and length of nighttime awakening, and in settling.
Parents are advised to determine a bedtime routine with sleep onset and wake-up time. The bedtime should be such that child will fall asleep within 15 min of going to bed. Once the child falls asleep at this time, the bedtime should be set earlier each night until desired bedtime is achieved. At the same time, wake-up time should be kept consistent, and the child should not be allowed to sleep beyond the prescribed sleep timings. If the child does not sleep within 15 min of going to bed, parents are advised to remove the child and keep him out of the bed for a predetermined time (1 h) to motivate him to fall asleep. He should be then again put to bed and this procedure is to be repeated through the night till the child sleeps within 15 min. On the next day, bedtime is to be made 30 min earlier.
This technique has shown to reduce settling problems, night awakenings, and co-sleeping.
This technique can be used by parents in addition to the above two if their child shows temper tantrums and unwanted behavior at night. In this technique, parents need to ignore the undesired behavior of child for 20 min and at the end of this period parent should go and settle the child. The duration for comforting should last from 30 seconds to 1 min.
Plan of Intervention
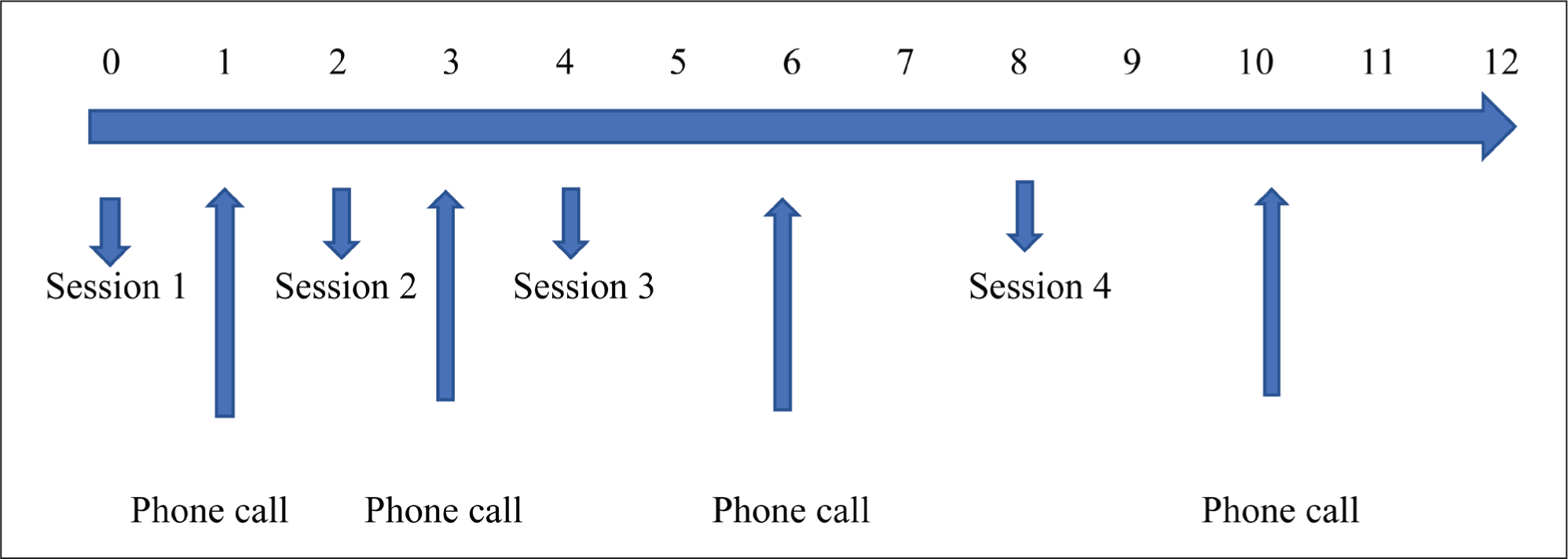
This module included four face-to-face group sessions on day 1 and then on weeks 2,4, and 8 and four telephone calls on weeks 1, 3, 6, and 10. The duration for the first session was two and half hours and the remaining were for 45 min.
First face-to-face session included educating the parents about ADHD and teaching them behavioral sleep intervention techniques. The education was a standardized and pre- recorded DVD played for all the parents in the sessions and followed by answering queries. Parents were given handouts to take home to help them follow the instructed practices. They were also given reminder cards with dates of their next sessions and telephone calls.
The further face-to-face and telephone sessions were conducted to ensure the parents were following the practice, to clarify difficulties faced by parents in practicing the techniques, and to encourage and motivate them to continue practicing the interventions.
Statistical Analysis
The formula used for the calculation of sample size (n) was n = (Z α/2 + Z β)2 * (p 1 (1 – p 1) + p 2 (1 – p 2))/(p 1 – p 2)2, where Z α/2 is the critical value of the normal distribution at α/2, Z β is the critical value of the normal distribution at β, and p 1 and p 2 are the expected sample proportions of the two groups. Based on this, our calculated total sample size was 90, but we recruited 100 participants. Data analysis was conducted with the help of SPSS version 20. Quantitative data was presented with the help of mean, standard deviation, and median. Comparisons were done with Chi-square test, paired t-test, unpaired t-test, Wilcoxon signed-rank test, and Mann-Whitney U test. Spearman’s correlation test was used to correlate between pre–post difference in scores of CSHQ with other scales and regression analysis between various socio-demographic variables and CSHQ improvement was done with Logistic regression test. p-Value <.05 was taken as significant.
Results
Our sample size was 50 children in each group. At follow-up, group A did not have any attrition and group B (comparator group) had attrition with 35 completing the study.
Demography: Both the groups were comparable for age with a mean of 10.66 years and range of 8−12 years (p = .15) with boys being more predominant (p = .85).
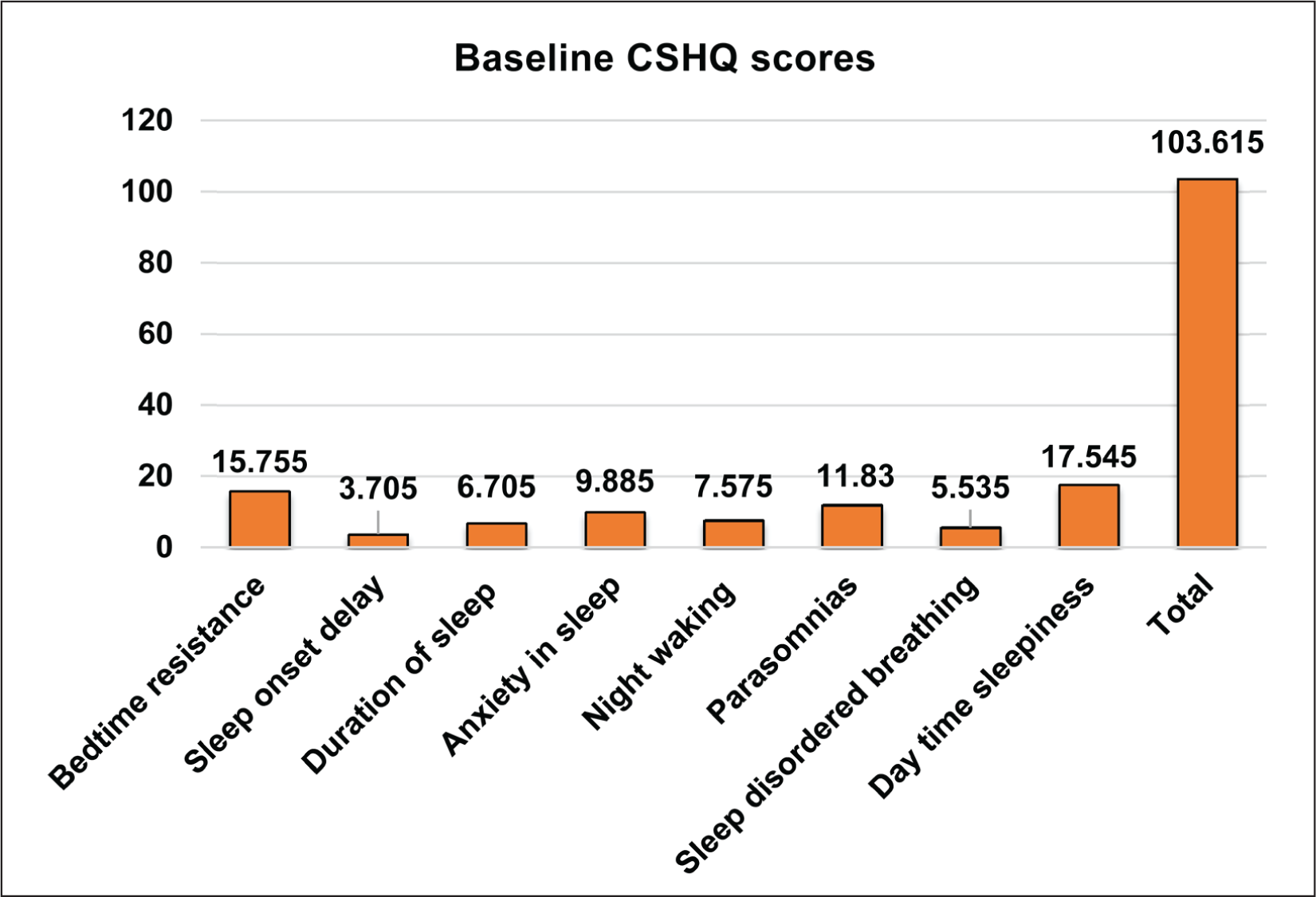
On the baseline assessment of sleep of all participants, the highest scores were found for “bed-time resistance” and “day-time sedation”. The baseline assessment in all the participants showed poor executive functioning and quality of life scores, high scores of difficult behaviors in children, and higher depression, anxiety, and stress scores in parents of these children (Figure 1).
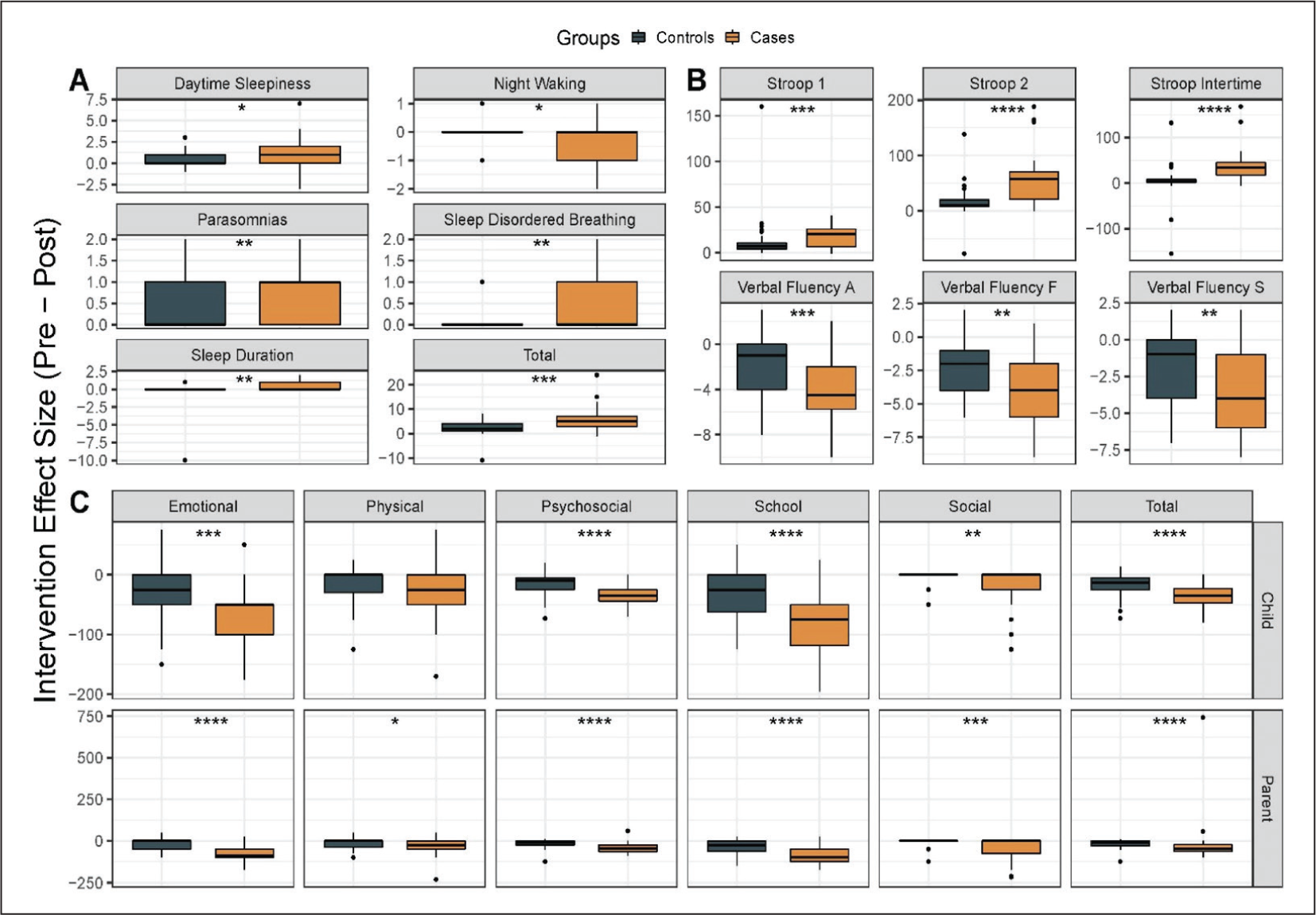
After calculating the post-intervention scores of all parameters in all participants, we calculated the difference between baseline and post-intervention scores and then calculated the mean in both the groups and then compared this mean between the two groups using Mann-Whitney U test.
On comparing the CSHQ mean between the two groups, significant improvement was found in interventional group in parameters of “duration of sleep (p = .006), daytime sleepiness (p = .012), total score (p = .000), parasomnias (p = .005), and sleep disordered breathing (p = .010).” However, worsening scores were seen on “night awakenings (p = .027).” In the executive function tests of Stroop (Stroop-1 p value = .007, Stroop-2 p value = .000004, Stroop inter-time p value = .000001) and Verbal Fluency (‘F’ p value = .08, ‘A’ p value = .001, ‘S’ p value = .003), significant difference with improved scores were seen in the interventional group. In the quality of life scale, both child and parent rated, parameters of emotional (p = .000, .00), social (p = .002, .00), school (p = .000, .00), psychosocial (p = .000, .00), and total (p = .000, .00) showed significant improvement in interventional group (Figure 2).
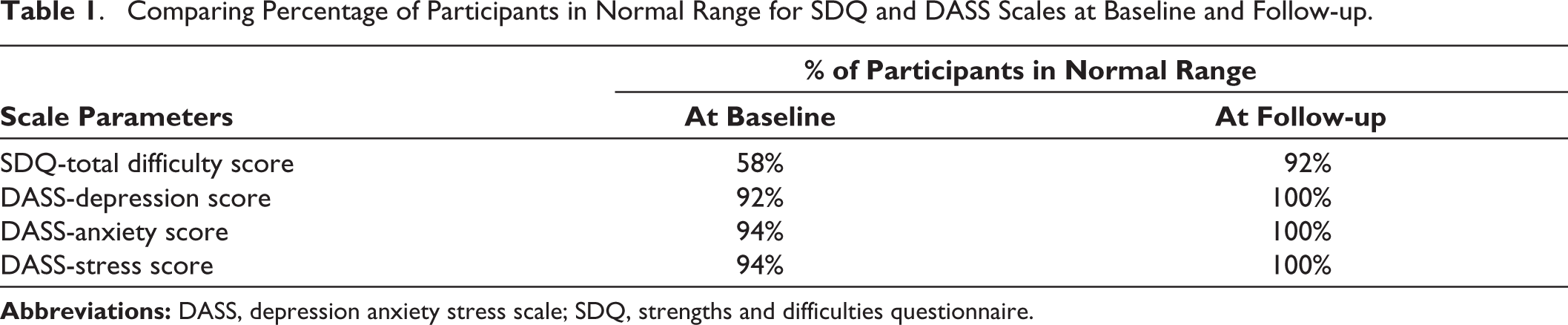
For SDQ and DASS-21 scales, the scores were measured in severity grade. On assessing the frequency of children who were in the unimpaired or average range, it was seen at the end of 12 weeks that SDQ total score had reached average range in 92% when compared to 58% at baseline (Table 1). Similarly, as seen in Table 1, the frequency of parents who improved in parameters of depression, anxiety, and stress is 100%.
Comparing Percentage of Participants in Normal Range for SDQ and DASS Scales at Baseline and Follow-up.
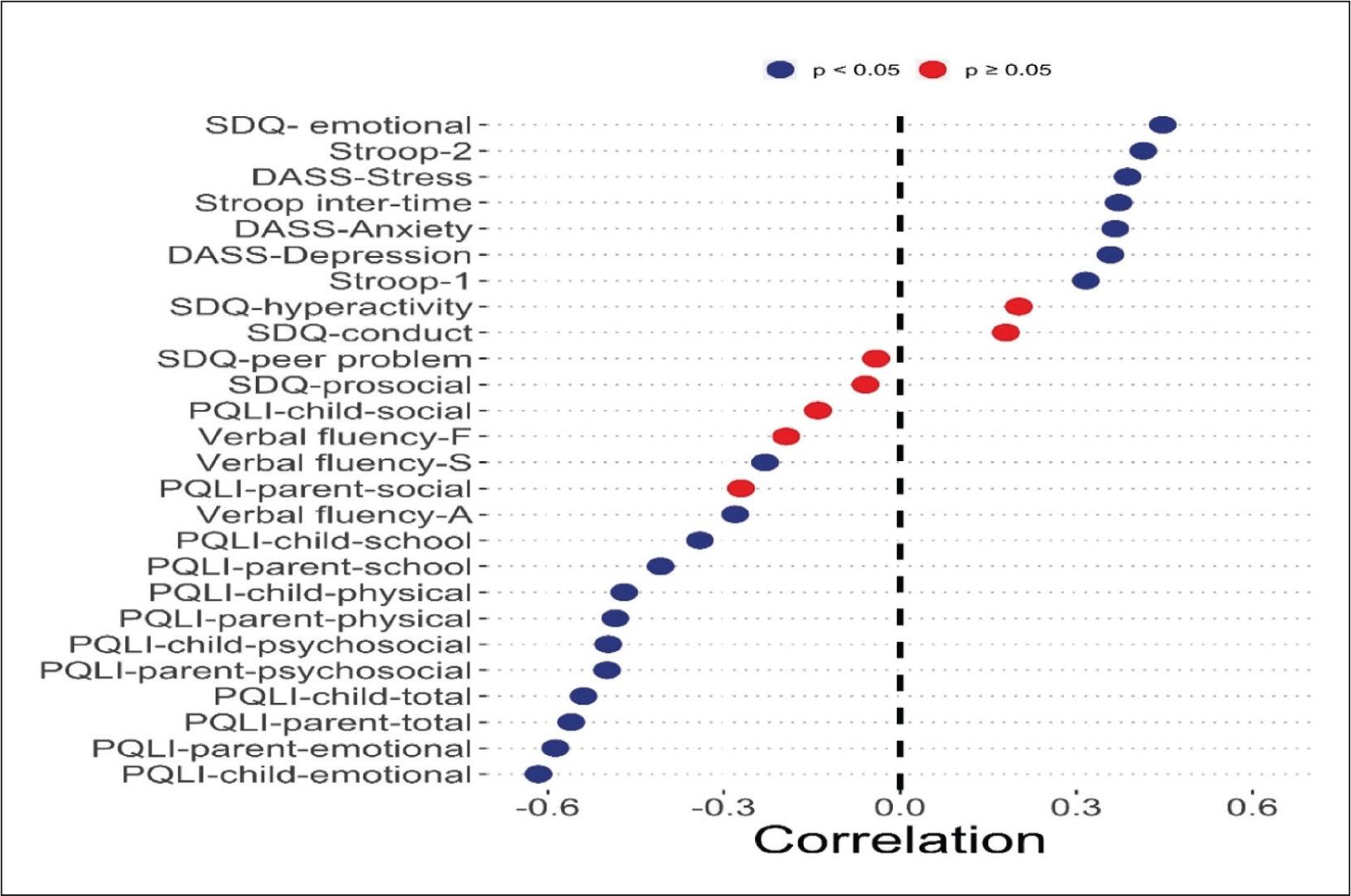
The correlation between change in sleep parameters (pre–-post difference of CSHQ) and change in all the other variables (pre–post-difference of other scales) only in the interventional group showed significant correlation with all except SDQ (Figure 3).
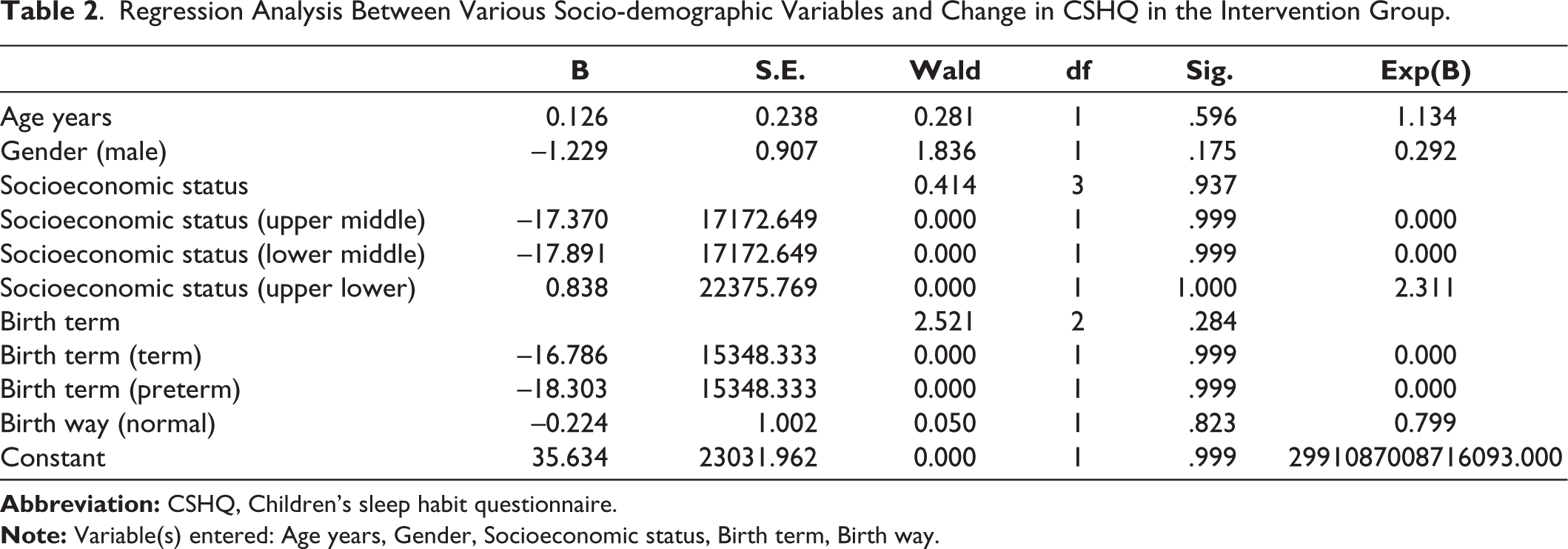
We also did a regression analysis between various socio-demographic variables and change in CSHQ in the intervention group and as seen in Table 2, we found that the change in CSHQ was independent of all other socio-demographic factors.
Regression Analysis Between Various Socio-demographic Variables and Change in CSHQ in the Intervention Group.
Discussion
Our research aimed at studying the complementary effect of sleep training program on various factors in child and parent. In children, we assessed the impact on sleep, executive functioning, emotional, behavioral, and social functioning, and in parents, we assessed the effect of sleep training program on their mental health. Adequate sleep is required for important cognitive and psychological functions and its disturbance in children with ADHD leads to worsening behavior, decreased quality of life, poor daily functioning, and decreased school attendance. Our study, which is similar to previous study, found difficulties with sleep, especially with bedtime resistance and daytime sleepiness.
Our intervention revealed significant improvement in the duration of sleep, parasomnias, sleep-disordered breathing, and daytime sleep and improvement in other parameters. The exception was worsening of night waking, which may be due to the effect of medication or increased awareness in parents. Probably, a longer duration of intervention or different sleep intervention techniques might be required for improving this parameter.
Our study matched previous studies on many aspects. It went beyond the previous studies to demonstrate improvement in parasomnias, symptoms of hyperactivity, and conduct. The improvement in parasomnias may be related to our study finding a higher frequency of these disorders, and therefore, unlike the previous study, this could not be studied due to the basal effect. Sleep and hyperactivity are interrelated and facilitating sleep probably led to our results. 6
The important findings of our study were that complementary sleep intervention improves the duration of sleep and quality of sleep and this is correlated with improvement in executive functions of the child and self-perceived quality of life. These improvements were independent of socio- demographic factors.
Parents reported improvement in the child’s emotional and conduct symptoms, peer relation, and prosocial behavior, besides the hyperactivity and attention symptoms. Parents too perceived improvement in all facets of the child’s quality of life. Parental stress and anxiety also improved. Our study suggests that educating and training parents about sleep, its significance, sleep hygiene, and a few behavioral techniques to improve sleep led to the improvement in child’s sleep, emotional and behavioral symptoms, quality of life, and improvement in parental stress.
Unlike other studies, we investigated the effect on cognitive functions and showed improvement of executive functions of the child with restitution in sleep. Studies on executive functions in ADHD have denoted difficulties with priority and time management, planning and organization, initiating and completing tasks in a timely manner, difficulty shifting cognitive set, a high level of procrastination, forgetfulness, and poor working memory. 8 Adequate sleep is required for important cognitive and psychological functions such as learning, memory, attention, mathematical skills, and impulse control.4,5 There have also been some studies on the effects of sleep problems on executive functions of children. Studies have shown that poor sleep adversely affects the neurological system involved in developing executive function in the form of loss of neuroplasticity, neuronal functional loss, and decreased neuronal reaction to learning. Sleep deprivation studies have also found that sleep deprivation leads to difficulty in planning and organization. 7 Studies conducted by Dewald Kauffman et al. and Beebe et al.27,28 have indicated that experimentally manipulated sleep time can have a direct effect on cognitive, emotional, and behavioral performance.
Attention deficit hyperactivity disorder is a neurodevelopment disorder causing significant impact in the life of the child. When this is compounded with sleep difficulties, emotional and conduct problems co-occur and there is poor quality of life. 29 Our study revealed similar findings, where children with adhd and sleep difficulties reported poor overall functioning, including social, emotional amd school. Our results correlated with research conducted earlier 12 stating significant improvement in the QOL in the interventional group.
We need to acknowledge the limitations of this study such as lack of objective measure of sleep and the restricted three-month follow-up. Future research could consider this as well as study the effect of intervention on different subtypes of ADHD. Despite this, our inclusive study strongly supports that the sleep intervention is effective in improving not only sleep but also quality of life, daily functioning, and cognition of ADHD children with sleep disturbances and also in improving anxiety, depression, and stress levels of their parents. We may also add that sleep intervention is easy to implement and gives good response, and hence, it can be used as an augmented treatment in all children, irrespective of their socio-demographic profile. Clinicians in their practice should consider behavioral sleep improvement techniques such as our simple module in addition to pharmacotherapy that may help these children in improving not only sleep but also various other aspects of life.
Footnotes
Acknowledgements
Dr. Ryan Anderson (Psychologist at Children’s Hospital of Pittsburgh) and Dr. Sangeeta Chakravorty (Associate Professor, Pediatrics, University of Pittsburgh School of Medicine) for their inputs in design of the module.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Dr Henal Shah and Dr Allauki Dani. The first draft of the manuscript was written by Dr Allauki Dani and Dr Henal Shah commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Transparency
All authors assure data transparency.
Declarations of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.