
Abstract
Psychiatric disorders in children and adolescents have a varied and heterogeneous presentation. Many risk factors play a role in the emergence of the disorder. Newer molecules have been tried for comorbidities in ASD and ADHD. Many have shown efficacy but need more robust evidence for clinical use. Oxytocin in ASD has shown efficacy however is not yet in clinical use. Viloxazine in ADHD has been FDA-approved and has shown efficacy in ADHD. Neuromodulation is tried in almost all disorders; however, studies are limited. Computer-based cognitive training has proven to be helpful in psychotic disorders. More trials are warranted to consolidate the evidence. Digital interventions and virtual reality can be a new way forward. Studies are limited.
Introduction
There exists heterogeneity in presentation and multifactorial nature in the etiology of child and adolescent mental disorders. A constant search for the most appropriate interventions in childhood psychiatric disorders persists. Research has been conducted on various neurodevelopmental disorders, psychosis, and mood disorders. Solid evidence is yet to be established since the trials have been few. The scope of the review includes the different interventions across the different disorders and understanding the framework of prevention in this population.
Recent Updates in Management Of Autism Spectrum Disorders (ASD)
Core Symptoms of ASD
An imbalance between excitation and inhibition involving glutamate and GABA signaling is proposed to be a disease mechanism in ASD. This dysfunction is implicated in impaired synaptogenesis and plasticity during early development stages. 1
NMDA receptor antagonist, Memantine, has shown significant improvement in memory, irritability, lethargy, stereotypies, hyperactivity, and language. 2
N-acetylcysteine (NAC), a glutamatergic agent, causes a decrease in the synaptic vesicular release of glutamate, resulting in decreased irritability in ASD. The effectiveness of NAC in autism has also been linked to its antioxidant properties. 1 However, there have been mixed results, with few studies not showing any difference in response compared to placebo. 2
Acamprosate is an NMDA modulator and GABA B inhibitor. Acamprosate resulted in an improvement in social responsiveness and hyperactivity. It was well tolerated with mild side effects. 3 Valproate has GABA inhibitory effect in specific brain areas. One study reported improvement in compulsive symptoms and irritability, but none reported improvement in aggression. Arbaclofen, the active R-isomer of baclofen is a GABA B receptor agonist. 4 It blocks pre – synaptic release of glutamate. 4 A study done by Erickson et al, 2014 showed that it improved irritability, social behavior, and compulsive symptoms. 5 D-cycloserine, a partial agonist at the NMDA receptor has been shown to positively affect social behavior, increasing sustained benefit from short-term social skills intervention in clinical studies. In pre-clinical studies, Fenobam, a metabotropic GluR5 antagonist, has improved repetitive and social behavior. 6
Oxytocin has been extensively studied for its role in regulating social behavior. Many clinical trials are underway to assess the long-term effect of oxytocin. A placebo-controlled trial of intranasal oxytocin therapy in children and adolescents with ASD showed no significant between-group differences in social or cognitive functioning over 24 weeks. 7 A meta-analysis with intranasal oxytocin found improvement in social impairments of ASD 8 and another found no effect on anxiety and repetitive behavior. 9 Social interaction and communication are also partly modulated by vasopressin in children with ASD. The polymorphisms in the vasopressin 1a (V1a) gene have been associated with ASD in humans, and V1a receptor antagonists have been found to modulate anxiety and regions of the brain related to face emotion processing. Balovaptan is an orally administered, selective V1a receptor antagonist. VANILLA, a phase two trial conducted in adult men with ASD demonstrated no effect of Balovaptan on the primary end point, Social Responsiveness Scale-2, however, showed clinically meaningful improvement on the secondary end point, Vineland-2 ABC score versus placebo. aVIation, a phase 2 study in children and adolescents did not show any benefit. 10
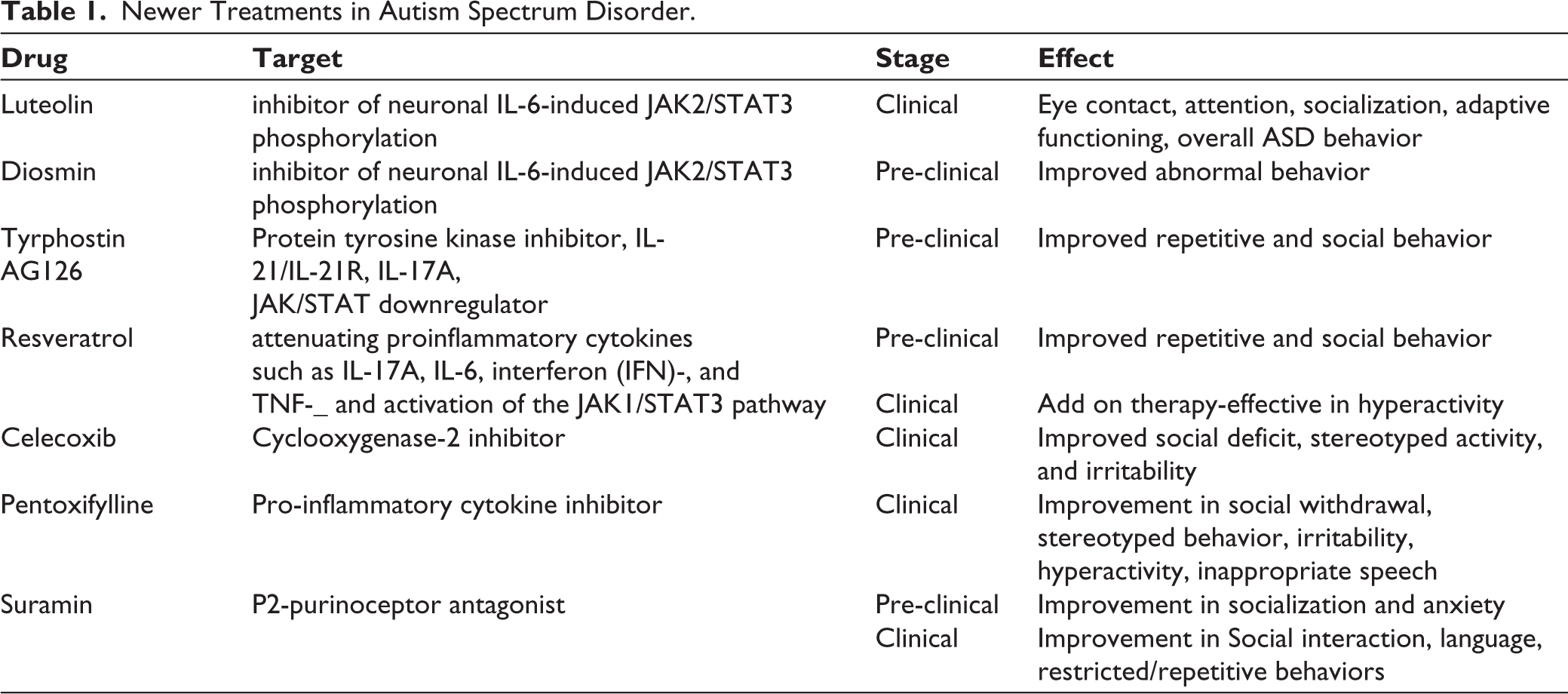
Children with ASD may present with maladaptive behaviors, including aggression, irritability, and self-injury along with the core features of ASD. Risperidone and Aripiprazole are two FDA approved drugs for children above 5 and 6 years of age. 11 Several case reports have also demonstrated efficacy and safety of clozapine which can be used to treat disruptive behaviors not responding to first-line antipsychotic drugs for patients with ASD. 12 Few case reports suggest significant aggression, irritability, tantrums, and hyperactivity improvement with long-acting injectable paliperidone palmitate. Similarly, other LAI antipsychotics are also thought to be helpful, especially for children who struggle with swallowing and compliance. 13 Some studies have shown altered levels of beta-endorphins in ASD patients. Naloxone and Naltrexone (opioid antagonists) demonstrated a reduction in self-aggressive behavior, hyperactivity, restlessness, and withdrawal, whereas some studies claim that it is effective in reducing only hyperactivity and restlessness and not the core symptoms. 14 Recently, several studies have confirmed the elevated level of cytokines in ASD patients. Hence, new treatments by immunomodulation have been assessed in several studies (Table 1). 6
Newer Treatments in Autism Spectrum Disorder.
Mood and ASD
The co-occurrence of ASD and mood disorders have a reported prevalence ranging from 1.4 % to 70 %.
The various interventions studied in mood disorders in ASD:
Repetitive transcranial magnetic stimulation (rTMS), noninvasive brain stimulation technique, is approved for depression in adults. Gwynette M et al, 2020 reported efficacy with high-frequency rTMS in reducing depressive symptoms (Hamilton rating scale for depression improved 13.5 points and 40% of participants achieved remission) with possible effects on core symptoms as well and was well tolerated. 15 Data on the pharmacological intervention in individuals with ASD consists only of case reports and open-label trials however, randomized controlled trials are lacking. Lithium and divalproex sodium have been widely used as mood stabilizers in autistic individuals, with research supporting their efficacy. The data on TCA and SSRI for treating depression in patients with ASD is limited and conflicting. 16
Anxiety and ASD
The prevalence of anxiety in ASD has varied widely, ranging from 13.6 to 84.1 %. Novel treatments include biofeedback and neurofeedback. However, they haven’t shown any specific effect on anxiety. 16
OCD in ASD
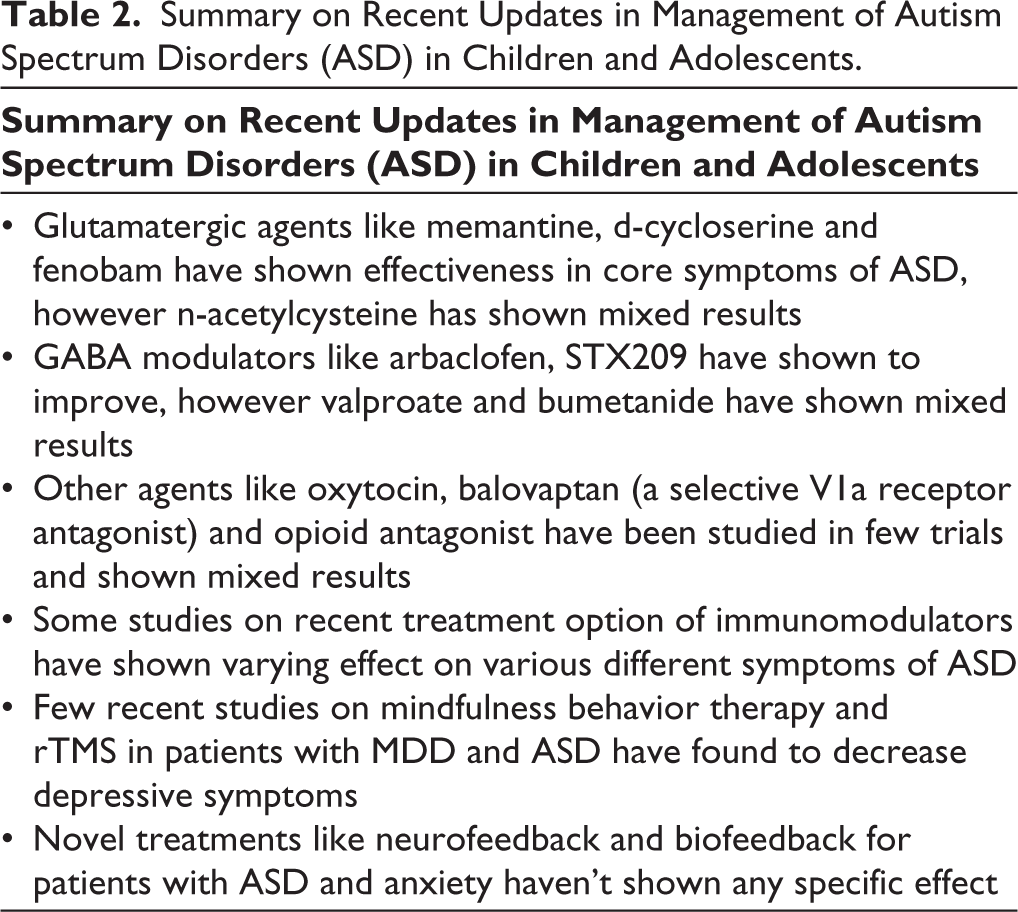
The prevalence of OCD in children with ASD is around 17%. 17 Both psychotherapy and psychopharmacology have some evidence to support their efficacy. There is limited yet mixed evidence for efficacy of psychopharmacologic treatment for comorbid ASD and OCD. Trials with risperidone and aripiprazole has shown mixed results. SSRIs, which are used as first line treatment in OCD-only population have shown mixed results in comorbid OCD and ASD population. A case study reported use of deep brain stimulation of the nucleus accumbens in an adult patient with ASD, refractory OCD, and aggression suggests that it may decrease OCD symptoms with effects lasting for up to 1 year. 18 A recent study suggested use of modified intensive CBT protocol that incorporated exposure with response prevention (ERP) for patients with ASD with OCD and resulted in significant improvement in obsessive compulsive symptoms, functionality, quality of life, anxiety and depression. The protocol included some modifications to individualize care to youth with ASD which included- increased attention to affective education, emphasis on therapeutic exercises while reducing focus on cognitive techniques, treatment planning incorporated participants’ restricted/stereotyped interests, increased participation of parent/caregiver, use of developmentally appropriate language, manipulatives to reduce abstraction in treatment. 19 A summary of recent updates in management in autism spectrum disorder in children and adolescents has been mentioned in Table 2.
Summary on Recent Updates in Management of Autism Spectrum Disorders (ASD) in Children and Adolescents.
Attention Deficit Hyperactivity Disorder (ADHD)
Many molecules have been tried in ADHD in the recent years.
Vilaxozine
Recently FDA approved SNMA (Serotonin norepinephrine modulating agent), in 2021. The underlying mechanism in ADHD is norepinephrine and dopamine dysregulation. A selective 5- HT 2B receptor antagonist and 5HT C receptor agonist blocks norepinephrine transport and reuptake of norepinephrine. It is available as an extended-release capsule with approved use between 6 and 17 years of age. Side effects are somnolence, headache, decreased appetite and irritability. It shows a greater reduction in ADHD symptoms. 20
Mazindol
It was originally used for obesity. It is repurposed for use in attention deficit hyperactivity disorder. It inhibits the reuptake of norepinephrine, dopamine and serotonin. It is a CNS stimulant. Mazindol (1 mg) showed improvement in a phase II study and was well tolerated. 21
Serdexmethylphenidate
A prodrug of d methylphenidate. The combination of Serdexmethylphenidate and dexmethylphenidate was FDA approved in 2021 for treating ADHD. It was observed to have an earlier onset of action, longer duration of therapy, few adverse events, and lower abuse potential. In an RCT on 149 children (ages- 6 to 12 years), a significant treatment effect with Serdexmethylphenidate over placebo with a significant treatment effect observed over 1 to 10 hours post dose. 22
Tipepidine
The mechanism is by inhibition of G protein coupled inwardly rectifying potassium channel currents (GIRK). It results in increase in monamine levels in brain. Tested in animals has shown improvement in hyperactivity. A randomized double blinded placebo-controlled trial was conducted in 53 children with ADHD, using 8 weeks of tipepidine as a supplementary medication to methylphenidate resulted in satisfactory efficacy and safety of adjuvant therapy in management of patients with ADHD. 23
Dasotraline
It is a triple reuptake inhibitor with preference for dopamine and norepinephrine reuptake. In animal studies, it resulted in reduced impulsivity and immediate reward choices. It has a long half - life and slow absorption. A significant improvement in attention and hyperactivity symptoms was seen in 112 children (6–12 years) with ADHD in a randomized, double blinded study using dasotraline 4 mg compared to placebo. Dasotraline was well tolerated with some adverse effects such as insomnia, headache and decreased appetite. 24 Dasotraline 4 mg/d, in a placebo controlled trial in 342 children aged 6–12 years, showed significant improvement in symptoms of ADHD and behaviors, including attention and hyperactivity and was tolerated well. 25
Centanafidine
A trial with centanafidine, a triple reuptake inhibitor, with preferential reuptake of norepinephrine and dopamine, is currently underway to evaluate safety and efficacy in children and adolescents. 26
Lisdexamphetamine Dimesylate (LDX)
Long-acting d amphetamine prodrug is FDA approved. In most cases, the mechanical release of the drugs and its conversion to active drug may be affected by gastro intestinal factors such as transit time and pH. The LDX prodrug uses enzymatic hydrolysis to convert the therapeutically inactive molecule to active drug, d amphetamine. It is long acting (13–14 hrs) with OD dosing. It is indicated from 6 to 12 years of age at doses of 30 -70 mg/d. 27
MTS (Methylphenidate Transdermal System)
Those with swallowing difficulties, overcomes enteric first pass metabolism. The duration of it lasts for more than 9 hours. It is FDA approved. 28
Technological Advances
FDA recently approved EndeavorRx for children of ages 8 to 12 years old, with inattentive or combined type ADHD. EndeavorRx improved attention as measured by computer-based testing. There is a lack of meaningful evidence for effective evidence and further studies are needed to consolidate its evidence. 29
Cognitive training has also been tried in ADHD. Now, computer-based applications are also used with cognitive training, resulting in changes in activation in task relevant, parietal and striato – limbic regions of sustained attention and working memory. 30
Neuromodulation techniques: Repetitive Transcranial Magnetic stimulation has also been tried in children and adolescents in open label trials with some improvement in symptoms of ADHD. 31
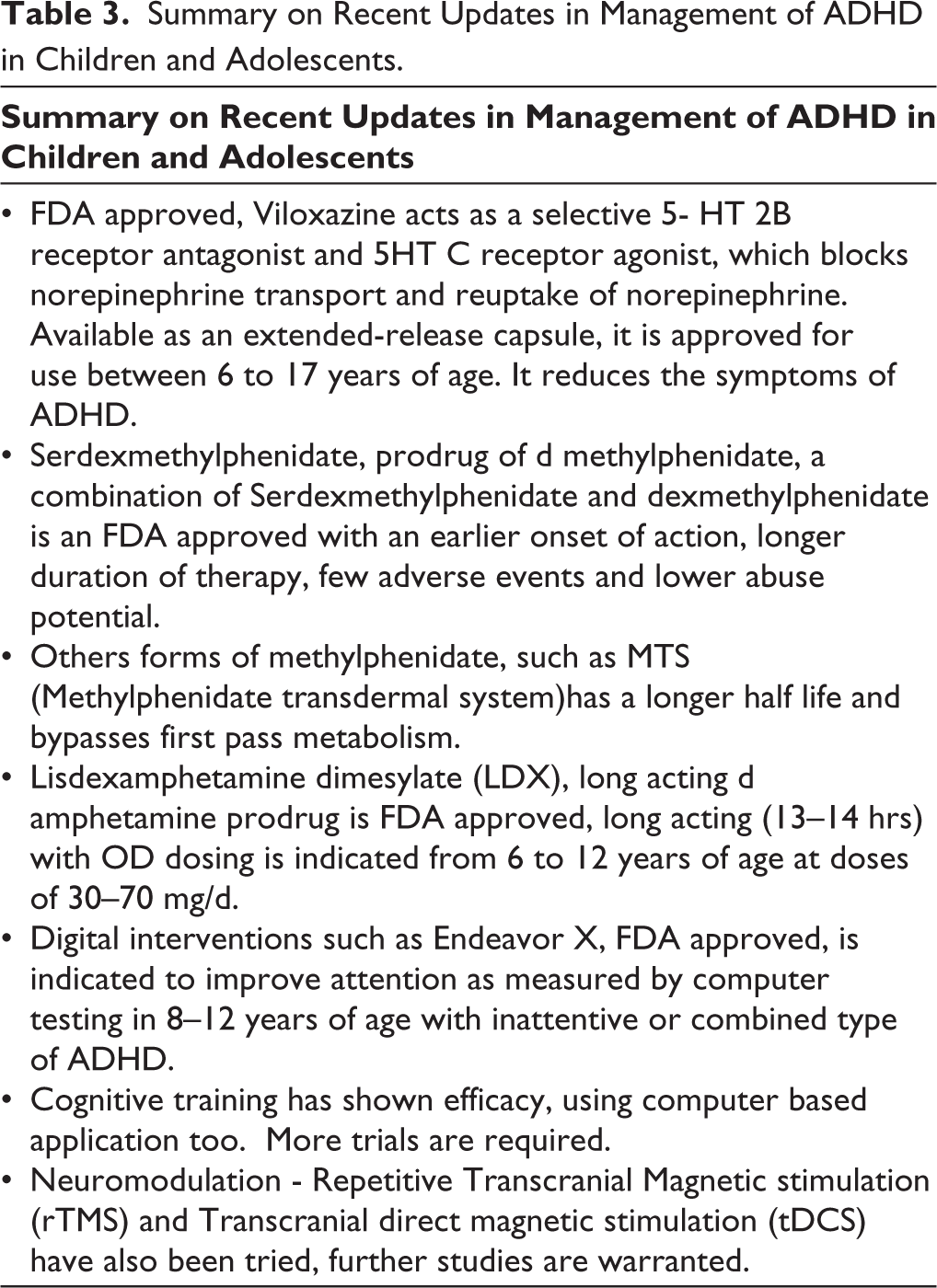
tDCS (Transcranial direct magnetic stimulation) – It alters cortical excitability and has been tried in disorders such as ADHD. It has been associated with improvement in cognitive deficits such as response inhibition, working memory, attention and cognitive flexibility and clinical symptoms such as impulsivity and inattention with no significant adverse effect. 32 A summary of recent updates in management in ADHD in children and adolescents has been mentioned in Table 3.
Summary on Recent Updates in Management of ADHD in Children and Adolescents.
Recent Updates in Management of Mood Disorders in Children
Depression
The psychotherapeutic techniques with the most extensive evidence for treating depressive episodes in children and adolescents are cognitive behavior therapy (CBT) and interpersonal therapy (IPT). 33 Many recent studies have shown the effectiveness of CBT in children with depression and anxiety. 34 A recent network meta-analysis of psychological therapies for child and adolescent depression found IPT and CBT to be significantly more effective than treatment as usual, placebo and waiting list. A modular approach to CBT, with flexible application of manualized focused treatment for problems in a young person, has shown to be more effective than treatment as usual. There is a recent growth in the development of mobile applications and computerized technologies; however, there is limited evidence on the use of applications for mental health disorders in children and adolescents. 35 A study done to assess the efficacy of an internet-delivered CBT protocol blended with weekly real-time therapist sessions via chat showed significant improvement in adolescent depression. 36 A recent Indian study on computer-assisted CBT (Smartteen) found that it was more effective in reducing symptoms of depression, improving functionality and adherence than usual treatment. 37 Results of a meta-analysis study has also shown evidence for the efficacy of internet and computer-based CBT in the treatment of anxiety and depressive symptoms in youth. 38 Family-focused interventions have recently emerged as a promising strategy in young children. 33 A recent and first study of agomelatine in children and adolescents with depression showed that 25mg/day of agomelatine along with psychosocial counselling was more effective in treating adolescent patients compared to placebo and had similar effect as fluoxetine. 39 A systemic review on rTMS (repetitive transcranial magnetic stimulation) in youth with depression found that rTMS can help reduce depressive symptoms in adolescents. However, controlled randomized trials are needed. 40
Bipolar Disorder
The mainstay for managing Bipolar Disorder (BD) in young children is using medication and enhancing social skills and family support. Currently, the FDA-approved drugs for children and adolescents with Bipolar disorder are risperidone, aripiprazole, quetiapine for more than 10 years, lithium for more than 12 years and olanzapine for more than 13 years old. One of the most important clinical trials in pediatric BD is the Treatment of Early Age Mania (TEAM) study which found risperidone to have higher response rates than lithium and divalproex sodium. Another systemic review on pharmacotherapy of pediatric mania concluded better response with aripiprazole, olanzapine, quetiapine and risperidone than mood stabilizers. The open-label trials on ziprasidone, carbamazepine, lithium, lamotrigine, and clozapine have shown positive effects. However, randomized placebo-controlled trials are needed to produce more definitive conclusions. 33 A prospective study with lithium monotherapy in individuals carrying the response-associated alleles was associated with a significantly lower rate of relapse. Anti-inflammatory strategies such as aspirin have shown potential to reduce risk of depression in epidemiological studies. Research on family focused therapy (combines psychoeducation and training in communication and problem-solving skills) is controversial, although it is related to longer affective stability and milder symptoms at follow-up. Interpersonal and social rhythm therapy have shown promising results in youth with BD. 41
Recent Advances in Psychosis in Children
A magnitude of structural, neurochemical and functional changes take place in the brain during the period of adolescence. This is also the time when there is reorganisation of the brain with regards to higher cognitive, social and emotional maturity. Significant amount of synaptic alignment and functional efficiency occurs during this early adulthood period. 42
Adolescence is usually the time when most of the cases of mental illness usually have their onset with nearly half of the cases seen during adulthood having started before the age of 14 years. 43 Imbalance between the inhibitory and excitatory systems along with disruption in the cortical and limbic pathways are proposed mechanisms for development of psychosis.
Cognitive Training
Cognitive training is a well-studied therapeutic process which aims at increasing or improving an individual’s capacity to process stimuli. This ability is generally affected in early psychosis. 44
Researchers working in the field of cognitive training have come up with a newer concept of cognitive remediation. This is a form of behavioral training which attempts to improve different cognitive processes, keeping in mind two basic goals of durability and generalization. 45
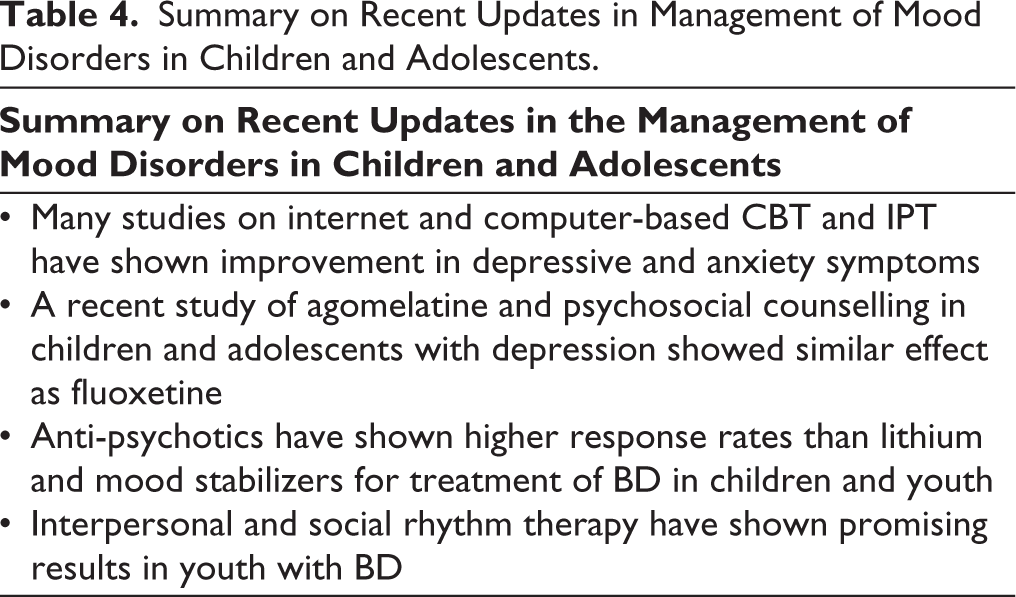
Cognitive training is of two types namely compensatory and restorative. Compensatory refers to operating changes in the environment to facilitate cognitive functions. 46 Restorative is goaled towards trying to correct specific deficit to repair the particular underlying compromised function. 47 It harnesses the inherent neuroplastic capacities of the brain. It is an intervention that uses specifically designed and behaviorally constrained cognitive or socio-affective learning events, delivered in a scalable and reproducible manner, to potentially improve neural system operations. 48 A computer assisted cognitive remediation program used in 32 adolescents with psychosis or at risk for psychosis, showed improvement in visuospatial abilities, reasoning and inhibition abilities at 6 month follow – up. 49 CRT( cognitive remediation therapy) resulted in improvement in verbal memory and executive functions, daily living in EOS in adolescents. 50 A summary of recent updates in management in mood disorders in children and adolescents has been mentioned in Table 4.
Summary on Recent Updates in Management of Mood Disorders in Children and Adolescents.
Neuromodulation
Transcranial direct current stimulation (TDCS) in 13 adolescents with childhood onset schizophrenia when used along with clozapine was well tolerated in these individuals. In 8 adolescents, when bilateral anode dorsolateral prefrontal placement, was used for cognitive difficulties and bilateral cathodal superior temporal gyrus for halluciantions, the modality was well tolerated. 51
RTMS (Repetitive transcranial magnetic stimulation) – the studies are limited to case reports and open label trials in psychosis. It has been tried in auditory hallucinations in early onset schizophrenia. It targets left temporoparietal cortex. There is less data and no published guidelines. 31
Digital technologies offer new opportunities for improving psychological interventions in an engaging and tailored way, as well as providing novel therapeutic contexts within which core psychological processes can be targeted in real time with immediate feedback. Smartphone based apps enable monitoring of distressing experiences and real time management strategies. A CBT informed smart app when used along with treatment as usual for early psychosis resulted in reducing negative symptoms, mood and general psychotic symptoms in a controlled trial. 52
Virtual reality users a computer technology by creating an illusion of being physically present in an artificial world. It is an acceptable intervention for adolescents with psychosis. The basis of CBT for psychosis lies in exposure to a trigger which evokes fear or paranoid ideations, allowing the user to test beliefs or form adaptive beliefs. It represents social environment which triggers physiological and psychological responses equivalent to the real-world context. However, the test outcomes have not been tested. 53
Preventive Approaches in Child and Adolescent Mental Health Disorders
Prevention programs helps reduce the risk of children developing a mental problem and disorder. These programs just as in medical disorders, can eliminate the emergence or even alter the trajectory by means of the preventive strategies.
Within the framework of prevention, there is: Primary, secondary and tertiary prevention.
Primary prevention- Universal, selective and indicated preventive interventions
Universal prevention – targets the general public or a whole population, that has not been identified on the basis of increased risk.
Selective prevention – targets individuals or subgroups of population whose risk of developing the disorder is significantly higher than average as evidenced by biological, psychological and social factors. Indicated prevention targets high-risk people who are identified as minimal but detectable signs or symptoms.
Secondary prevention includes early detection and treatment of diagnosable diseases. It revolves around reducing the established cases of the disorder.
Tertiary prevention encompasses interventions which reduce disability, enhance rehabilitation and prevent relapses and recurrences.
Most of the treatment approaches in child and adolescent mental health disorders revolve around tertiary prevention, which reduce symptoms, distress, disability and facilitate functionality and integration of the individual in society by offering rehabilitative approaches. This would include pharmacological interventions, psychotherapeutic approaches and parenting programs.
In most developmental disorders, the primary preventive approaches revolve around perinatal interventions, screening in prenatal stages, and nutritional supplements in the pre-natal/infantile stage.
Secondary approaches include the identification of biomarkers in at-risk individuals, genetic studies, interventions in at risk of disorder stage. 54
Following are the Preventive Approaches
Attention Deficit Hyperactivity Disorder
Using our understanding of glutamatergic signilang, fasoracetam in adolescents with ADHD has been tried with the improvement since in scores on the Vanderbilt parent version scale. 55 Interventions such as Perry Preschool and the Abecedarian Project have shifted the trajectories associated with residence in high poverty communities. These alter educational, occupational and criminal outcomes in children. Parenting programs during pre-school years such as TEAMS(Training Executive, Attention and Motor skills (TEAMS) which is a program developed for 4 to 5 years old children with ADHD uses games to target neurocognitive skills. Many other programs have been designed along similar lines. 56 A summary of recent updates in management in psychosis in children and adolescents has been mentioned in Table 5.
Summary on Recent Updates in Management of Psychosis in Children and Adolescents.
Autism Spectrum Disorder
The Deficiency of Insulin growth factor - 1 lead to insufficiency of neuron myelination and defective synapse function resulting dysconnectivity in the neural circuitry observed in 1st post partum infants. This may result in social malfunction in childhood years and beyond. Hence prenatal or post natal Vitamin D. Prenatal or post natal Vitamin D supplementation also increases the circulating IGF -1. This offers protection only in high risk siblings of ASD. Also IGF administration of exogenous IGF 1, only in high risk siblings of ASD. 57
Another intervention in primary prevention, is the initiation of gene therapy largely for research purpose, antisense nucleotides are used to silence RNA or gene products that are deleterious. However, the studies are limited to animal models. 58
A study assessing atypical visual orienting with white matter changes in 7 month olds with a risk for autism spectrum disorder revealed longer visual orienting latencies who expressed ASD symptoms at 25 months compared with both high-risk negative infants and low- risk infants. 59
Psychosis
A deficient cerebral inhibition is a pathophysiological brain deficit related to poor sensory gating and attention in schizophrenia and other disorders. Cerebral inhibition develops perinatally influenced by genetic and in utero factors. Amniotic choline activates fetal alpha 7 nicotinic acetylcholine receptors and facilitates the development of cerebral inhibition. Supplementation of choline to pregnant mothers and newborn post-natal 3 months resulted in inhibition characterized by suppression of amplitude of second P50. Children had fewer attention deficits and lesser social isolation. 60
Prenatal anxiety in mothers was observed to have a lower vagal activity across the first 2 years, with lower immunity and more illness with reduced gray matter in childhood. Emotional and mental development include greater negative emotionality and lower mental development scores in infants and internalizing problems.
Anxiety disorders occur during childhood and elevated cortisol and internalising behaviors occur during adolescence. Interventions for parental anxiety are virtually non existent although stroking (massaging) the infant has been observed to reduce pregnancy – specific anxiety effects on internalising behaviors in the offspring. 61 Another study to support the evidence of maternal stroking of infants reported associations between pre-natal depression and anxiety and child outcomes at 29 weeks and 2.5 years. Long term effects of early maternal stroking, modifying associations between pre natal anxiety and child emotional and behavioural symptoms. 62
The understanding of biomarkers can be considered an example of secondary prevention. For instance, an increased expression of CA4, associated with greater risk of schizophrenia, is associated with disrupted synaptic refinement in adolescence which plays a key role in disease etiology. 63 A summary of recent updates in preventive approaches in children and adolescents has been mentioned in Table 6.
Summary on Preventive Approaches in Children and Adolescents.
Challenges in Prevention Programs
Execution of programs is challenging in clinical practice. The availability and cost effectiveness of the programs also must be kept in mind. What is “at risk” does not transition into disorder. There are critical ethical issues pertaining to preventive interventions in at-risk individuals. Potential benefits need to be balanced against risks of pre onset interventions. Key considerations include an individual’s knowledge, autonomy, and right to choose, ideally in an environment of stigma-free treatment.
Limitations
Despite safety of interventions, most interventions are not FDA approved. Some of these interventions may have unforeseen side effects or interactions. There exists limited research and experience. Most disorders are heterogenous in presentation. Many of these interventions fail to transition from preclinical to clinical stage of targeted treatments. The lack of validated, objective biomarkers for diagnosis, treatment prediction, and relevant neural circuit modulation poses the challenge in identifying the most appropriate intervention. There is also a need for improved clinical endpoints and more robust trial designs.
It is important to navigate regulatory requirements for all new therapeutic indications.
Conclusions
Most childhood psychiatric disorders are heterogenous in presentation. A multitude of interventions has been tried across the different childhood psychiatric disorders however, a handful of them are in clinical use. Neuromodulation techniques have been tried across disorders however, we are yet to gather more evidence. Computer-based therapies and digital health interventions across all disorders have been tried but need more studies. Virtual reality has been tried, still in the nascent phase warranting further studies to gather evidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.