
Abstract
Background:
As a signatory of the United Nations Commission on Child Rights, India has enacted laws and policies to protect the child’s interests. The Juvenile Justice Act of 2015 addresses the needs and well-being of the most vulnerable children, including those who do not have anyone to care for or have experienced a traumatic upbringing and those who are allegedly in conflict with the law. No research from India addresses these vulnerable children’s mental health and well-being. The current paper describes a pilot project to create mental health awareness and improve children’s care access in India’s Juvenile Justice System (JJS).
Methods:
Permission was obtained from appropriate governmental agencies in Odisha and Tamil Nadu and Child Care Institutions (CCIs) that consented to participate. A co-creation model was utilized to create youth-friendly spaces and methods to deliver mental health literacy for all stakeholders and access to care.
Results:
Seven CCIs and 278 children across two states participated in the implementation of the project. 37.8% of the children had resided for less than six months and 34.5% for more than two years in the current CCI. Of the various adverse childhood experiences, neglect was the highest at 76.3% followed by parental issues at 32%.
Conclusions:
Children in the JJS have many risk factors predisposing them to develop mental health issues. This unique pilot project describes implementing a codesigned and co-created model of delivery of mental health literacy and access to care to this vulnerable group of children.
Abbreviations
Child Care Institutions
Children in Conflict with the Law
Children in Need of Care and Protection
Juvenile Justice Act of 2015
Juvenile Justice System
Mental Health Literacy
Youth Friendly Spaces
Introduction
Providing an appropriate and safe environment for children to grow is essential for their long term wellbeing. As a signatory of the UN Convention on the Rights of the Child, India has been making great strides in changing the legal structures to protect the needs and safety of the children in the country. The amended Juvenile Justice (Care and Protection) Act (JJ Act) was passed in 2015 to ensure appropriate care, protection, and treatment of all children. 1 It incorporated international standards to deal with Children in Need of Care and Protection (CNCP) and Children allegedly in Conflict with the Law (CCL) to ensure the disposition of matters in the child’s best interest.
As per the JJ Act, CCL refers to a child who is alleged or found to have committed an offense and has not completed 18 years of age on the commission of the said crime. The CNCP refers to a child who has faced unfavorable conditions such as homelessness, being abandoned, missing or runaway, vulnerable to drug abuse and trafficking and child labor, or victim of neglect, abuse or exploitation, or having a mental illness or intellectual disability or suffering from an incurable or terminal illness and has no one to support look after them. 1 The JJ Act recognizes facilities for providing care and protection for children who need such services called child care institutions (CCIs). As per a recent survey by the Ministry of Health and Family Welfare, 2 there are nearly 9600 CCIs that house and care for close to 370,000 children across the country. The CCIs are unevenly distributed across the country, with Tamil Nadu having nearly 1700 CCIs and housing about 60,000 children, while Arunachal Pradesh has only eight homes housing about 200 children and the state of Odisha has 427 CCIs, as per the survey.
Research on mental health issues among the youth in the juvenile justice system (JJS) globally is predominantly from developed countries and focused on children who are in conflict with the law. 3 A recent review concluded that the lifetime prevalence of mental health problems in detained adolescents far exceeds the prevalence of mental health problems among adolescents in the general population. 4 Mental health morbidity, including substance use has ranged from about 60% to 75% in different studies even after adjusting for a diagnosis of conduct disorder. Prevalence rates of mood and anxiety disorders and disruptive behavior disorders varied from 10% to 25%. 5,6 In a study of juvenile detainees in the USA, 7 47% of the youth (12-18 years) endorsed mental health symptoms within the first two weeks of being detained. Substance use was noted in about 70% of the detainees, with cannabis and alcohol being the most common at 70% and 31%, respectively. The review by Scheffler et al 8 summarized that these vulnerabilities in childhood might lead to the development of maladaptive coping strategies, including avoidance, substance use, and negative eating behaviors. Also, it increases the risk of developing mood and anxiety disorders, substance use disorders, and psychotic illnesses.
The rates of mental health issues drop as adolescents move out of detention centers. Still, they are higher than the general population, with nearly 45% of males and 30% of females having one or more psychiatric disorders.9,10 While the rates of mania, substance use disorder and depressive disorders dropped, the rates of anxiety and related disorders (including PTSD) increased. Even after 12 years, it was noted that only about 1 in 5 males and half of the females were able to achieve less than half the positive outcomes in the domains of educational attainment, residential independence, gainful activity, desistance from criminal activity, mental health, substance use, interpersonal functioning, and parenting responsibility. 11
The data from Lower and Middle Income Countries also mirror the results of High Income Countries regarding the increased psychiatric comorbidity and self-injurious behaviors among juveniles in conflict with the law.12,13 In India, more than 86% of the juveniles under inquiry had a history of substance use. 14 In a study done among about 180 CCL youth in the National Capital Region of Delhi, 15 were noted to have low literacy levels and mainly were from a lower socio-economic status. The study documented that the degree of Adverse Childhood Events (ACEs) in youth in one of the detention centers in India faced had a significant bearing on their risk of developing mental health issues.
As per the UNICEF report, 16 there were nearly 2 million children in institutional care due to various reasons, with a recent study 17 concluding that the numbers currently range between 3.18 to 9.42 million children. A review 18 summarized the significant negative effects of institutionalization on children’s developmental and mental health. There are also neurobiological changes 19 seen among children in foster care that suggest that these children are more sensitive to exclusion during activities among their peers. The children are also prone to mental health problems as evidenced in a recent study of adolescents in Nepal’s childcare homes, 20 where nearly 33% had clinically relevant depressive symptoms. Being female, being bullied, having low social support, having medical issues, and consuming alcohol increased the risk of developing depressive symptoms in these adolescents.
The JJS in India also provides care for vulnerable children (CNCP). The various issues that bring children under the care of the JJS including a history of abuse, trafficking, loss of parental support/ inability to care for the child also increase the risk of developing mental health issues. The mental health of children in orphanages have been studied using various rating scales and have reported the rates of depression ranging from 14.7% to 74.5%.21–23 There are many structural problems in working with children in CCIs 24 as evidenced by a qualitative study 25 with the staff working in various CCIs who identified a lack of professional and trained staff, obsolete vocational and life skill training, and unhealthy parent-child relationships as barriers to appropriate rehabilitation and social integration of the children.
As evidenced by the literature review, there is limited information about the mental health and wellbeing of children in the JJS in India even though they may be exposed to the multiple risk factors associated with the future development of mental health problems. The Juveniles Accessing Mental health Services (JAMS) project was initiated to address this gap. This is a pilot project funded by the Grand Challenges Canada, NIHR aimed at enhancing mental wellbeing, mental health literacy and access to mental health care for children in the JJS in India. This paper reports on the demographics of children in the participating CCIs in the two states of Odisha and Tamil Nadu and the components of interventions developed.
Methods
Study Setting and Design
The JAMS project was initiated in Odisha and Tamil Nadu from April 2021 after obtaining ethical clearance from the primary organization’s Institutional Ethics Committee (IEC). Following this, the district collector of Ganjam district in Odisha and the Department of Social Defense in Tamil Nadu, which oversee the implementation of the JJ Act in the respective states, were approached for permission to conduct the project. This was followed by listing and approaching the district’s various CCIs, including governmental and nongovernmental organizations that cared for children under the JJ Act (i.e. CNCP and CCL), with information about the project and goals. A total of 7 CCIs - 4 in Odisha (167 children) and 3 in Tamil Nadu (111 children) consented to participate in the program. Three catered to CCL (105 children) and four to CNCP (173 children). Following this, the staff, administration, and assent from the children between the ages of 12-17 in the selected CCIs that gave written informed consent were inducted into the project.
Tools
Socio-demographic information, including life experiences before coming to the CCI was collected using a standardized proforma. The mental wellbeing of children was measured using the Warwick-Edinburgh Mental Wellbeing Scale, a 14 item questionnaire measuring positive affect, interpersonal relationships and functioning as components of emotional wellbeing. 26 The Perceived Stress Scale is a 10-item questionnaire that quantifies the stress experienced by an individual in the month before evaluation. 27 The Strengths and Difficulties Questionnaire (SDQ) – adolescent self-report version was utilized to screen the children for emotional, conduct, hyperactivity/ inattention and peer relationship problems and prosocial behaviors. 28 All the tools were administered in the children’s native language. These scales have been validated to be used among adolescents.
Ethical Concerns
All the research staff underwent comprehensive child protection policy training at the primary research institution. It was ensured that no identifying data of the children was recorded from the individual CCI and each child was assigned an identifier and the key that linked the identifier to each child was maintained within the confines of the same CCI from where the data was taken. When a child scored high on the Strengths and Difficulties Questionnaire (SDQ), the staff was informed to facilitate ongoing mental health care and if there was any concern about the child’s immediate safety within the CCI. The research assistants conducted all the sessions in the presence of one of the staff members from the CCI.
Results
Socio-Demographic Profile
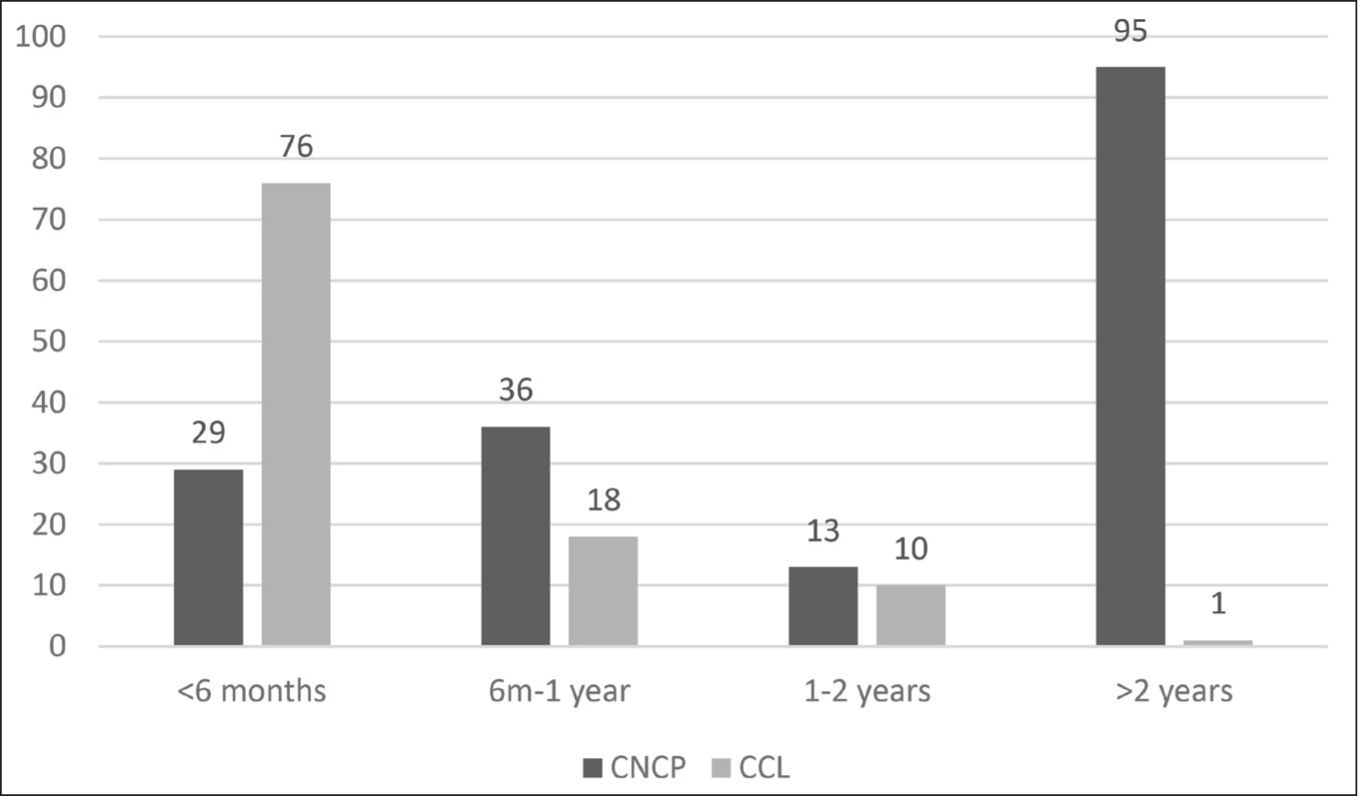
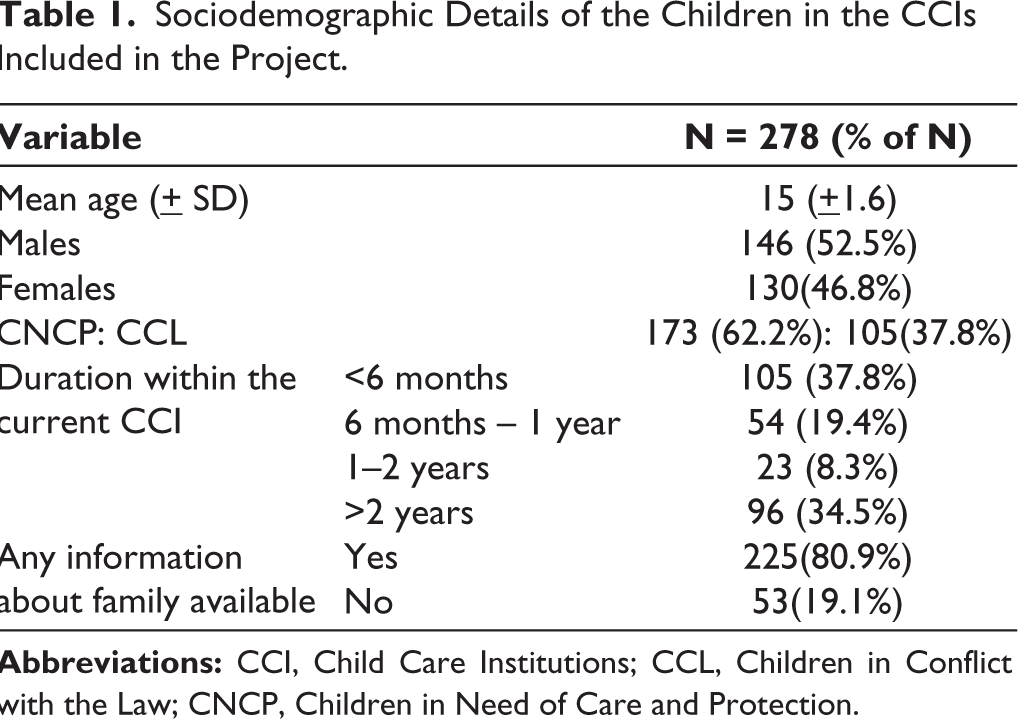
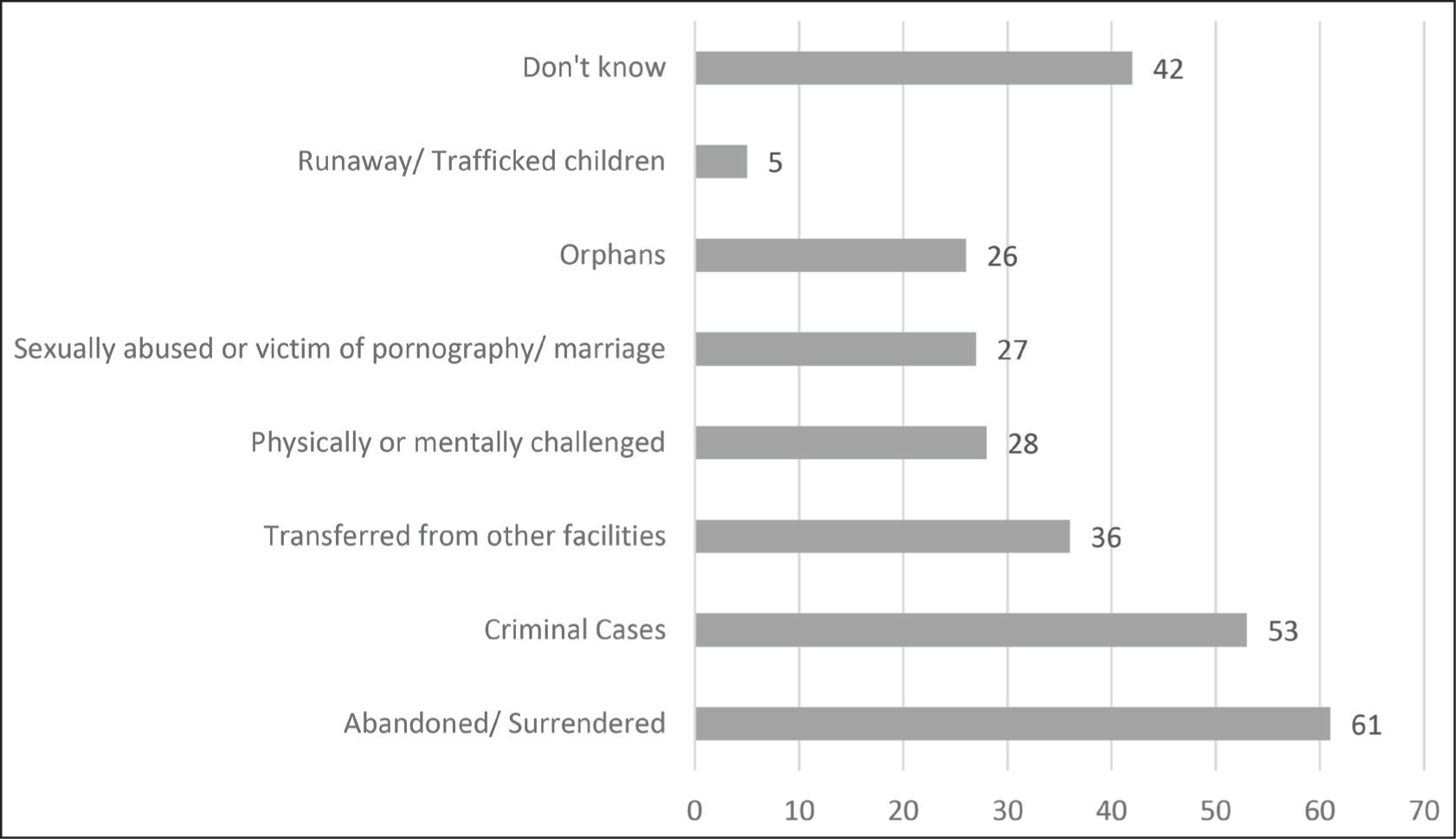
The mean age of children in the population was 15 + 1.6 years, with no male-female differences noted. The socio-demographic details of the children is shown in Table 1 and 80.9% of the children, were aware of their family of origin. The children had either spent less than 6 months (37.8%) or more than two years (34.5%) in the CCI where they were seen. The CNCP were more likely to be residents of the CCI for more than two years compared to CCL who were more likely to be residents for less than six months in the facilities (see Figure 1). The children had reported varied reasons for entry into the CCIs (see Figure 2), with most reporting either criminal cases or having been abandoned or surrendered.
Sociodemographic Details of the Children in the CCIs Included in the Project.
Where did the Children Come From?
Life Experiences of the Children in CCIs
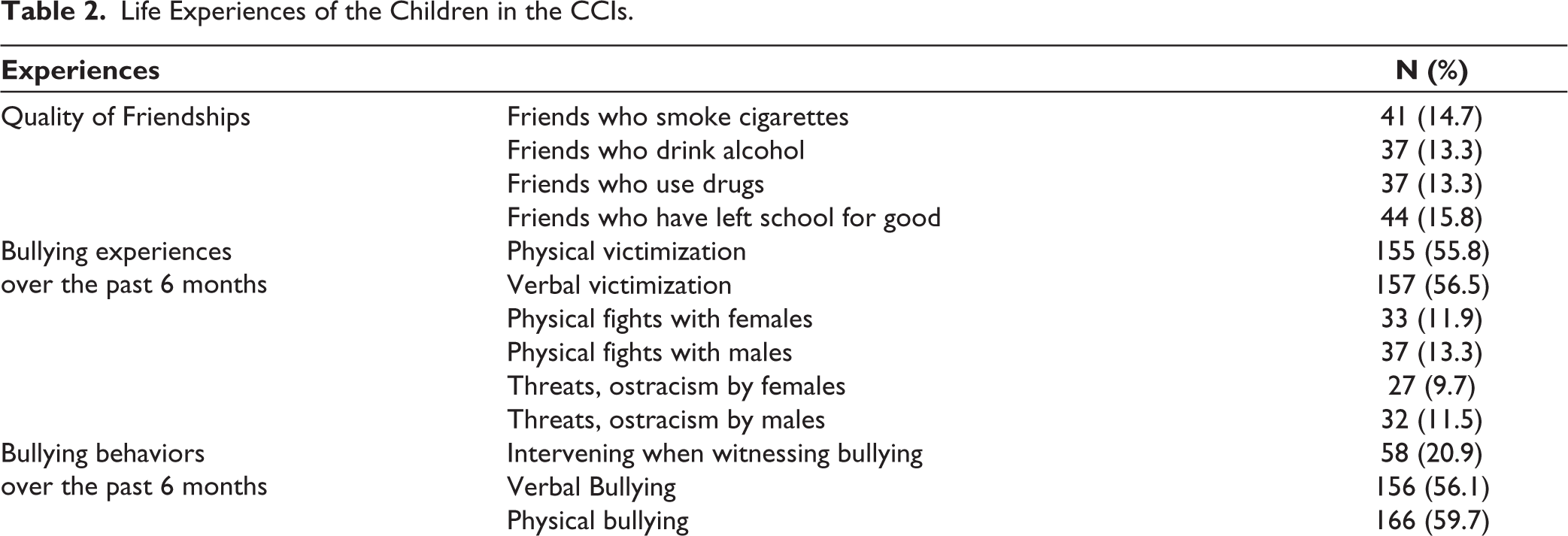
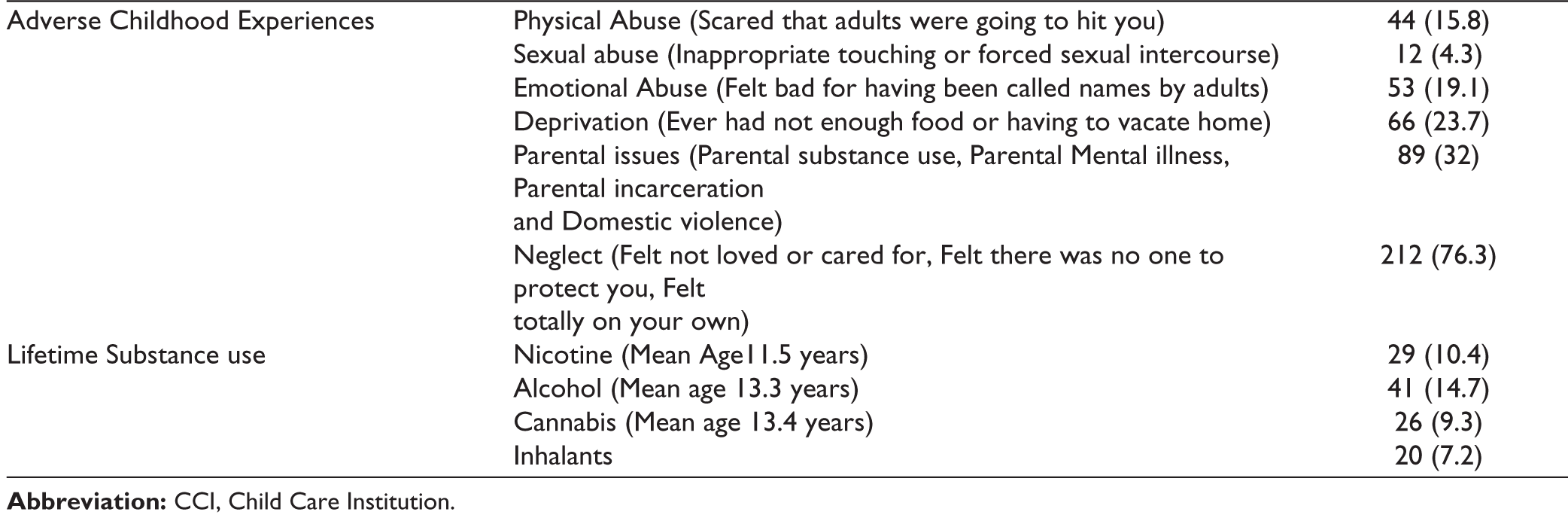
Table 2 highlights the various life experiences of children in CCIs. Alcohol use was endorsed by 14.7% of the children, nicotine by 10.4%, cannabis by 9.3%, and inhalants by 7.2%. More than half of the children had experienced verbal (56.5%) or physical (55.8%) bullying or victimization and also had perpetrated the same (56.1% and 59.7%, respectively) in the six months before the assessment. Neglect (including physical and emotional) was the most commonly reported adverse childhood experience (ACE) (76.3%). A history of sexual abuse was reported by 4.3% of the children.
Life Experiences of the Children in the CCIs.
The JAMS intervention
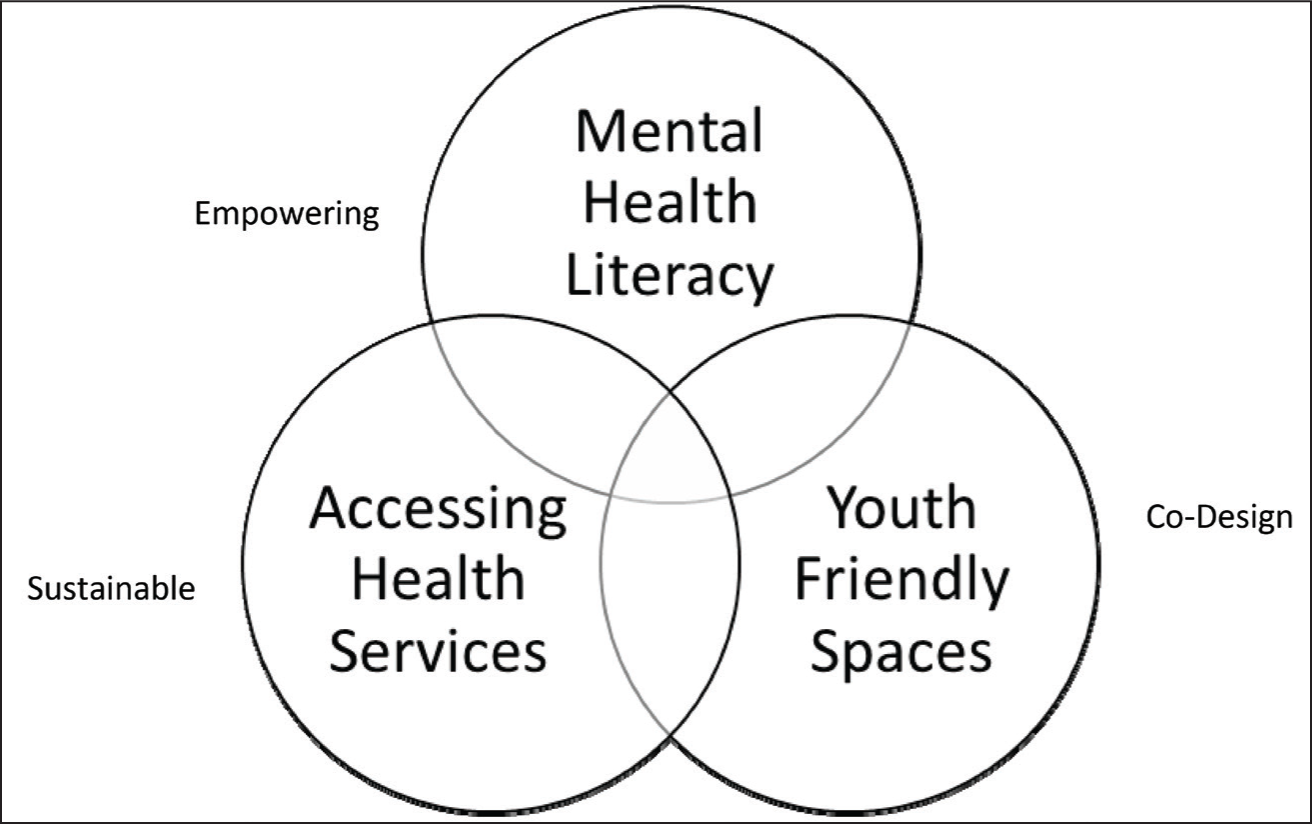
Given the nature of the multiple vulnerabilities faced by these youth, the JAMS project focused on empowering them to not only know about aspects of mental health but also create systems to ensure that they could access appropriate mental health care when needed. Furthermore, given the limitations CCIs work in, a focus on the program’s sustainability was also considered. Thus, the program was developed in a co-creation model with the children, the staff, and administrators weighing in on how the program could be implemented. Using the definition as mentioned in a review, 29 co-creation was considered an essential component, with the stakeholders assisting in identifying the issues and generating solutions. Under this overarching goal of co-creation, a co-design process was used to address issues such as creating safe spaces and mental health literacy materials. The intervention was centered on three key components: youth-friendly spaces (YFS), enhancing mental health literacy (MHL), and creating appropriate links for ongoing mental health care (see Figure 3).
The JAMS Intervention.
The YFS
This is a non-clinical physical space (invariably a room or a hall within the CCI earmarked for this purpose at the said time) that was co-designed within the confines of each CCI in consultation with the staff, administration, and the children. This space was to be utilized by the children to unwind and engage in
During the rest of the week, the YFS functioned under the supervision of volunteer senior children and a staff member who would maintain the space and support any children there. The senior children in the facility were invited to volunteer to lead the YFS and were trained by the research staff to support their peers. The co-creation process involved the children at all steps from the time that they would like to access the space to the contents, including materials that they would use within the space including board games, and arts and crafts materials.
Enhancing Mental Health Literacy (MHL)
An important aspect of the intervention was to enhance the MHL of all the stakeholders in the care of the children in the CCI. These included the children, staff members, administrators, and members of the JJS. The MHL was contextualized to the needs of the groups. The administrators and members of the JJS were sensitized to the bio-psycho-social model of mental health problems and the various social vulnerabilities and their effects on children’s mental health. The staff who were involved in the day to day care of the children had case-based discussions lasting about 12 hours, over a period of 6 weeks on various aspects of mental health, including enhancing communication with children, the bio-psycho-social model, the various mental health problems and their methods of evaluation and management, including triaging and referral pathways. These referral pathways were created keeping in mind the available local services. At the end of the training period, the material was compiled into a book and given to the staff as a ready reckoner.
As a part of the co-design process, other children between the ages 12-18 in communities similar to where the CCIs were located were engaged in a discussion about how they wished to learn about mental health. Some replies included using multimedia (like movies/ cartoons) through play and activities. A script for animation videos was created and shared with the children who had provided the initial feedback, and following a few iterations, and the videos were created. These videos included topics ranging from an introduction to mental health and various illnesses, including depression, anxiety, psychosis, substance use, and help-seeking. These videos were then piloted with children from the community and the CCIs where the intervention was going to be implemented before they were finalized. To ensure that the staff members could use the videos and engage the children in the future in discussion about mental health, a discussion module for each of the videos including frequently asked questions and information on the content was created and shared with the staff.
Access to MH Services
Following an increase in mental health literacy, the program hypothesized an increased need for referrals for mental health services. A stepped model of care provision was considered with the peers being the first level of support and then the staff who had more training in communicating with the children and finally the referral for mental health services. To support the various CCIs and their staff, linkages were created with local government hospital psychiatry departments to make the program sustainable. A specific staff member and an identified mental health professional in the psychiatric departments were connected after obtaining consent from both. A common referral and follow-up form was created after discussion with the CCIs and psychiatry departments to enable continuity of care for the children.
Discussion
Nearly 1/3rd of India’s population is below 18, according to the 2011 census. 30 The period of youth is not only a period of growth and development but also a period of vulnerability to mental health issues, as most mental health issues tend to emerge below the age of 18. 31 In addition to the biological changes that are seen in this age group, the influence of the social environment, including the peer group, family, and community and life experiences like exposure to violence, abuse, neglect, and bullying on the long term mental health and wellbeing of individuals cannot be overemphasized. 32
The study by Desmond et al 17 reported that there were no standard definitions of institutional care for children and that there was higher variability of reporting and estimate of number of children in institutional care in South Asia compared to other regions in the world. While the roles of the CCIs are clearly defined in the JJ Act, the children under the care of the JJS are a disparate group of individuals some of whom are there on account of their life circumstances and life experiences they may have faced or due to their actions. This paper describes an intervention to enhance the mental health and wellbeing of the children in within the JJS in two states in India – Tamil Nadu and Odisha.
ACEs were very commonly reported in our study with neglect being the highest and sexual abuse being the lowest. More children endorsed neglect (76% vs 29–69%) in our study as compared to a scoping review by Leloux-Opmeer et al. 33 One of the reasons for this disparity could be that our sample had nearly equal representation of both CCL and CNCP and nearly 80.9% of the children being aware of some aspect of their family of origin as compared to the review which considered only children in residential or foster care. Similarly, parental issues, including domestic violence in this study, was found to be around a total of 32% which is in keeping with the range, 15–36% reported in the literature on children in foster care 33 but, lower than the rates reported among children who were previously incarcerated (65–84%). 34 A study among adolescents rescued from child labor in India, 35 83.4% reported childhood abuse or neglect, with physical abuse being the most common at 72.7% and emotional abuse at 47.7%, and neglect in 17.4% as compared to our sample where, 15% children endorsed physical abuse and 19% emotional abuse. This difference could be related to the nature of children included in our study, which included both CNCP and CCL. Few children reported sexual abuse (4.3%), which is much lower than the international (7.9% male and 19.7% females) 36 and national (20–50%) statistics. 37 The data collected in this study was cross sectional, quantitative and did not provide the opportunity to explore this sensitive subject. Information on ACEs in this population is of interest for implementation as research has shown a dose response relationship between ACEs, including physical neglect, family violence, household substance use and household member incarceration. 38
This study also highlights the children’s environmental concerns while living in the CCIs. There is a lack of stability in the living arrangements, with about 38% having been in the current facility for less than six months and nearly 13% of the children being transferred from a different facility to the current one. As evidenced from the data, more CCL were short term residents (<6 months) of the current CCI while more number of CNCP were long term residents (>2 years). Frequent transitions may have a negative effect on the ability of children to trust and engage with the staff. Future studies may need to reflect on the reasons influencing children’s transition between CCIs.
Self reported substance use was between 7-14% in our study, which appeared to be significantly lower than studies done abroad, including among children in juvenile institutions in Sweden (55%) 5 and in India (86.44%). 14 Similarly, about 55% of the male adolescents in the community endorsed having tried substances in India. The onset of substances ranged from 10.4 years for nicotine to 13 years for alcohol and cannabis, comparable to children in the community. 39 Similarly, 13-15% of the children endorsed having the company of individuals who had used cigarettes, drugs, or alcohol. These differences could be related to including both CCL and CNCP in our study wherein we hypothesize that the CNCP who were more likely to be residents of institutional care may not have access to substances as compared to the CCL who were living in the communities before coming to institutional care.
Bullying experiences were more common among the children in our study as compared to another study from Nepal (~56% vs 16.6%) 20 . In keeping with a review by Srinivasan et al 40 from the SAARC countries, the prevalence of bullying behavior was notably similar (59% vs 16-85%). In our sample of children, verbal and physical victimization were the most common compared to threats and ostracism.
The data highlights the multiple vulnerabilities that may predispose children in CCIs to many mental health issues in the future. Thus, this program focused on MHL as a key component of its intervention. MHL was originally defined as the “knowledge and beliefs about mental disorders which aid their recognition, management, and prevention”. 41 While most of the research is focused on delivering and evaluating individual components of MHL, 42 our focus through this program was not only directed on improving knowledge about symptoms and kinds of mental health problems but also on enhancing wellbeing and empowerment to seek and receive help for the same. Furthermore, the contextualization of the material to the recipients, i.e., children, staff, administrators, and members of the JJS, was planned to address the different needs of each stakeholder. This ranged from self-care and peer support for the children, care of children and triaging for the caregiver staff, and enhancing knowledge among administrators to initiate policy level changes. This contextualization was achieved through a co-creation process with the involvement of all stakeholders at all levels.
One of the strengths of our work through this pilot project has been the inclusion of CCIs serving both CCL and CNCP and across 2 states using standardized questionnaires. Furthermore, the co-creation process using children as active participants in creating appropriate material is unique to this intervention. The limitation of this study is the use of self report questionnaires rather than an in depth and sensitive discussion about some topics, such as sexual abuse. These questionnaires also lend themselves to recall bias and a desirability bias because these children were aware that the results of their answering the questions would be shared with the staff members if there were concerns of safety.
Conclusion
Children in the JJS have multiple vulnerabilities, and this study describes the characteristics of both CCL and CNCP. These life experiences may have an ongoing component of bullying and victimization in addition to the events in the past. All these increase the risk of mental health problems. Thus, creating appropriate and acceptable methods to convey MHL and a space where children can practice and experience the same is essential to help address these vulnerabilities early in life. Further exploration on the differences between the needs of the CCL and CNCP may need to be explored and policy such as the JJ Act may have to become more nuanced based on these learnings. This is a unique pilot intervention that addresses not only the capacity of the children to help identify their difficulties but also works towards enhancing the system’s capacity to respond in case children raise such concerns. Through this project, we hope to demonstrate that a sustainable model of delivering mental health education and care to children in the JJS is possible.
Footnotes
Acknowledgements
Dr R. Thara—Vice Chairman board of directors, Ex-Director SCARF (I), Dr Suresh Kumar—Psychiatrist, Mrs Girija Kumarbabu—Ex-Chairperson of Juvenile Justice Board and Juvenile Welfare Board, Mr Sai Prasad Samal—Manager of Childline, ISRD, Ganjam District, Odisha.
Author Contributions
Conceived study and designed analysis: SP, RP
Collected data: ADB, CA, PP, RE, SSN
Analysis of data: SP, CA, RE
First draft: SP
Review and comments: SP, ADB, CA, PP, RE, SSN, RP
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This pilot project was funded by Grand Challenges Canada, NIHR – Global Mental Health Grand Challenge: Mental Health and Wellbeing of Young People (Grant number – R-GMH-POC-2107-4395).
Ethical Approval
This study was approved by the Independent Ethics Committee of Schizophrenia Research Foundation (SCARF) dated March 23, 2021.
Informed Consent
Written informed consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.