
Abstract
Background:
Although the concept of a slim body was first introduced in Western societies, body dissatisfaction and disordered eating became a globalized issue, and appeared in India and other Asian cultures as well. However, we know much less about the background variables in this region.
Aim:
To further examine potential risk and protective factors for disordered eating, we aimed to detect the role of online activity (smartphone addiction, time spent online), social anxiety and social support as well as Body Mass Index (BMI), academic performance, and sociodemographics in elevating the risk of disordered eating among a sample of Indian adolescents.
Methods:
This study employed 112 high school students (aged between 14–18 years; mean age = 16.01 years; SD = 1.08; 47.3% females) from a private high school located in Vadodara, India. Besides sociodemographics, weight and height (Body Mass Index, BMI), academic performance, and average screen time on weekdays/weekends) were asked. We used four different instruments for exploring the psychological variables: Eating Attitudes Test (EAT-26), Smartphone Addiction Scale – Short Version (SAS-SV), The Kutcher Generalized Social Anxiety Scale for Adolescents (K-GSADS-A), and Multidimensional Scale of Perceived Social Support (MSPSS).
Results:
Using a cut-off score of 20 points, 9.8% of the students were evaluated as being at risk for disordered eating. Besides time spent online on weekdays, smartphone addiction, social anxiety and avoidance, and higher BMI scores elevated the risk of disordered eating in bivariate logistic regressions, while social support served as a protection. In the final multivariate model, only two factors remained significant contributors: being online on weekdays (risk) and being online on weekends (protection).
Conclusion:
These findings highlight the different roles of Internet use in the risk of disordered eating (weekdays: risky, weekend: protective) among this sample of Indian adolescents which can be explained by a possible shift in students’ social connections (from peers to family) during the different period of the week.
Keywords
Introduction
Eating disorders are complex conditions characterized by disruptive eating behaviors that particularly affect adolescents as the most vulnerable group due to dramatic changes in their physical and psychosocial functioning, such as body image and self-perception. 1 The prevalence of eating disorders, including anorexia nervosa (AN), bulimia nervosa (BN) and binge eating disorders (BED) as most common types, is estimated approximately 6% to 8% among adolescents. 2 Although more frequently detected among female adolescents, eating disorders occur in all genders, races, ages, ethnicities, sexual orientations, body types and social classes. Eating disorders can be accompanied by severe somatic symptoms as well, such as drastic hormonal changes, electrolyte imbalance, arrhythmias or blood cell anomalies. 3 Besides eating disorders, however, disordered eating, such as weight-loss dieting or unhealthy weight-controlling behavior also need attention, particularly since they elevate the risk of eating disorders. 4 Therefore, investigation on the background variables of adolescents’ disordered eating may be useful in prevention of eating disorders. In addition, these background variables can play different roles in distinct cultures.
When Western societies introduced the concept of a slim body as a symbol of female beauty, it triggered a higher level of body dissatisfaction in the countries concerned. 5 However, a growing number of studies revealed that disordered eating patterns have become a global issue in the 21ST century and eating disorders now are a salient problem in India and other South Asian countries as well.6,7 Although a plump body shape has traditionally been accepted in Indian culture, urban adolescent girls tend to follow Western standards for the ideal body shape. In this process, urbanization, modernization and the globalized media play a crucial role. 8
In a sample of Indian adolescent girls aged 13–18 years from Allahabad, Uttar Pradesh, the prevalence of disturbed eating was 26.7% and it was associated with a number of psychological variables such as perfectionism, negative life events and lack of appropriate social-emotional support. 9 As it seems, among adolescents, group processes and social activities can play a decisive role in their behavioral decision on eating patterns. Social support and social acceptance help adolescents develop positive attitudes toward themselves. On the other hand, the lack of them, e.g., lower familial support was related to disordered eating in a sample of late adolescents from the US. 10 In another study of American high school students, family connectedness especially served as a protective factor against body dissatisfaction and disordered eating. 11 Thus social support seeking can be serving as a way of coping in body image and dieting problems. 12
Among the social variables, social anxiety and disordered eating are often comorbid conditions since the fear of negative evaluation involves shape concerns and appearance anxiety. 13 Stress often mediates between these health problems similarly to low self-esteem. 14 Disordered eating, together with body dissatisfaction, often stem from a feeling of loneliness and fear of social rejection, features of social anxiety, particularly when it goes together with a lower level of self-esteem. For adolescents, peers’ opinion is extremely relevant and social comparison of their physical appearance can lead to disordered eating when it is unfavorable. 15
Other social influences can also be important contri- butors. Media is a powerful influencing factor in shaping young people’s body image and eating behaviors through idealized images and messages. 16 In the digital era, excessive smartphone and internet use can particularly play a decisive role in forming adolescents’ lifestyles, health attitudes and behavioral choices. 17 The severity of eating disorders was found to be associated with internet and smartphone application usage. 18 In Southeast Asian countries, like Malaysia or Indonesia, pathological internet use contributed significantly to the risk of eating disorders. 19 School-chidren’s recreational screen media use was found to be influenced by family factors, like parental education or having only a single parent, low socioeconomic status, but above all, household screen use. 20
In addition to social variables, some additional (individual) factors also need to be examined, such as Body Mass Index, academic achievement or sociodemographics. A study of adolescents from Cyprus revealed that risk and protective factors of disordered eating did not differ significantly by gender or BMI. 21 The relationship of BMI with disordered eating is often mediated by the adolescents’ body dissatisfaction 22 ; this latter evaluation is not necessarily depending on the objective body weight status. 23 In terms of academic performance, the risk of eating disorders was negatively correlated with grades in school 24 and high school achievement was found to act as a protective factor against disordered eating. 25
Despite a growing number of research on eating disorders from India over the past several decades, this is still an under-reported field, particularly the issue of disordered eating and its psychological and social correlates. 26 In addition, most studies done on adolescent populations with only small samples and limited to restricted number of variables/scales.27, 28 Actually more research is needed to explore Indian adolescents’ risk of disordered eating including potential contributors. Therefore, this cross-sectional study aimed to further examine risk and protective factors for disordered eating in a sample of Indian adolescents with special attention on a set of social variables, and digital device activities in particular. First, students with or without the risk of disordered eating were compared along the study variables. Then the main focus was to investigate the role of smartphone addiction, time spent online, social anxiety and avoidance, Body Mass Index, academic performance and sociodemographics in determining the risk of disordered eating by using bivariate and multivariate logistic regression analyses.
Sample and Methods
This cross-sectional research was carried out from June 2021 to August 2021 and involved high school students from a private high school, located in Vadodara, India (n = 112). All students of the school were invited to participate in the study (N = 156) and 112 filled in the questionnaire giving a response rate of 72%. Before conducting the research, ethical approval has been granted by the ethical committee of the Doctoral School of Education, University of Szeged (reference number: 4/2020). After getting permission from the school principal, a written informed consent from the parents and their children were obtained before the survey. Those who sent back this form received an e-mail through the school mailing list that provided students with a link to access the survey on Google Forms. Participation was anonymous and voluntary.
In the first part of the online survey, there were questions about sociodemographics, body weight and height – for later calculating BMI scores –, academic performance (school grades on a 7-point scale), and the average time spent online on weekdays and weekends (using a 10-point scale from a few minutes through one hour, two hours… more than eight hours). This section was followed by four different scales for exploring the examined psychological variables.
Disordered eating was measured by the Eating Attitudes Test (EAT-26). 29 The self-reported scale evaluated attitudes (e.g., dieting, bulimic or oral control), beliefs and behaviors concerning food, body weight and shape with responses on a 6-point Likert scale. The cut-off score ≥ 20 had the meaning of being ‘at risk’. This scale is widely used on Indian adolescent populations.9,30 The reliability value (Cronbach alpha) was 0.91 in our current sample.
The Smartphone Addiction Scale Short Version (SAS-SV) was used to identify the level of smartphone addiction. 31 It consisted of six items with responses on a 6-point Likert scale. Similar to the previous scale, this measurement has already been applied on Indian populations. 32 Cronbach alpha coefficient was 0.92.
The Kutcher Generalized Social Anxiety Scale for Adolescents (K-GSADS-A) 33 had two subscales: social anxiety and avoidance. Each item is rated on a scale of 0 (none) to 3 (severe/total avoidance) for a) the level of discomfort/distress/anxiety and b) the adolescent’s level of avoidance of the situation (e.g., asking a stranger for directions). Cronbach alpha values was 0.97 for both subscales.
Multidimensional Scale of Perceived Social Support (MSPSS) comprises a 12-item scale that measures the perceived support received from family, friends and significant others. 34 Answers were evaluated on a 7-point Likert-type scale. Reliability value was found to be 0.95.
Although some of these scales have been widely used on Indian population (e.g., a hindi version is also available of EAT-26), since they have not been validated yet we used the English version of the scales and in each case the reliability values proved excellent.
SPSS for MS Windows Release 22.0 was used to analyze the data, with a maximum significance level set at 0.05. The analysis started with an examination of descriptive statistics where Student’s t-tests were used to detect significant differences by grouping students whether they are at risk or not in terms of disordered eating. Next, binary logistic regression analyses (bivariate and multivariate) were used to examine correlates of EAT risk by calculating odds ratios (OR) with 95% Confidence Intervals (CI). An odds ratio > 1.0 indicates that there is a positive association between the factors of interest to the baseline odds, while a value < 1.0 indicates the opposite.
Results
The participants’ age varied between 14-18 years; mean age = 16.01 years; SD = 1.08; 47.3% females. The sample’s distribution of age well represented the structure of the high school (34.8% aged 14 or 15; 30.3% aged 16; 34.9% aged 17 or 18). Detailed sociodemographic characteristics of the sample can be seen in Table 1.
Sample Characteristics (N = 112).
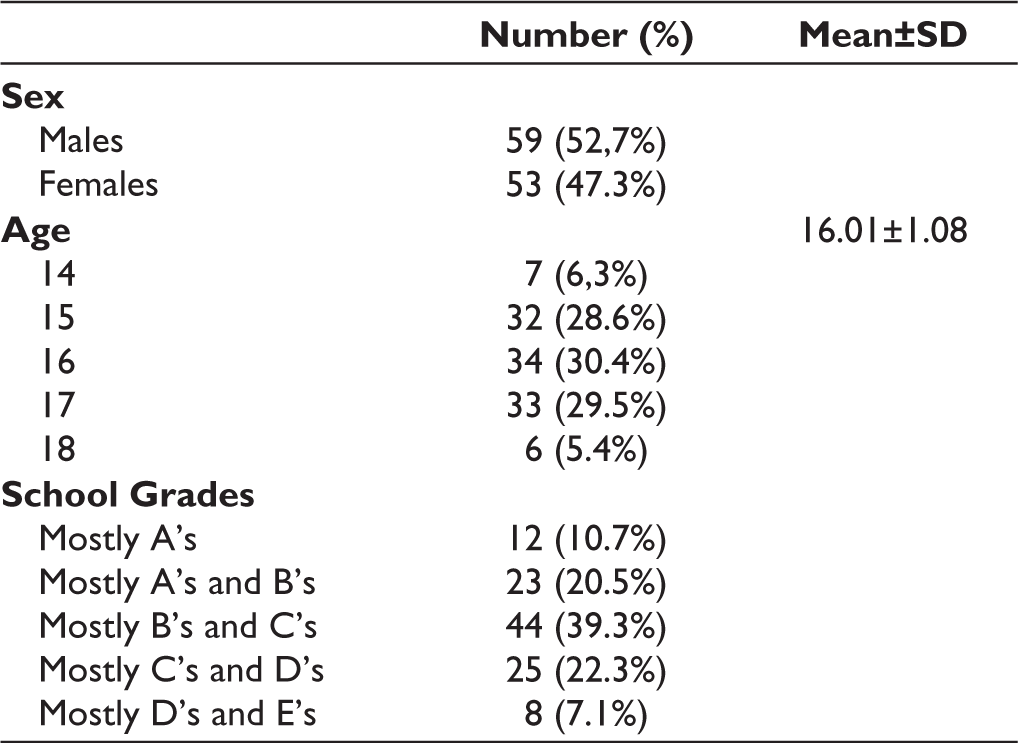
Most students reported being online for more than six hours on weekends (36.6%), while 21.4% of them spent 4 to 5 hours online on weekdays. Using a cut-off score ≥ 20 points, 9.8% of the students were evaluated as being at risk of disordered eating (oral control, diet, or bulimic behavior); 11.3% of girls and 8.5% of boys [χ²(1; N = 112) = 0.25; P > .05]. Table 2 presents descriptive statistics (mean, SD, minimum and maximum values) for the study variables with a comparison of two groups: with and without the risk for disordered eating (EAT risk).
Descriptive Statistics and Group Differences for the Psychological Scales and Other Variables (N = 112).
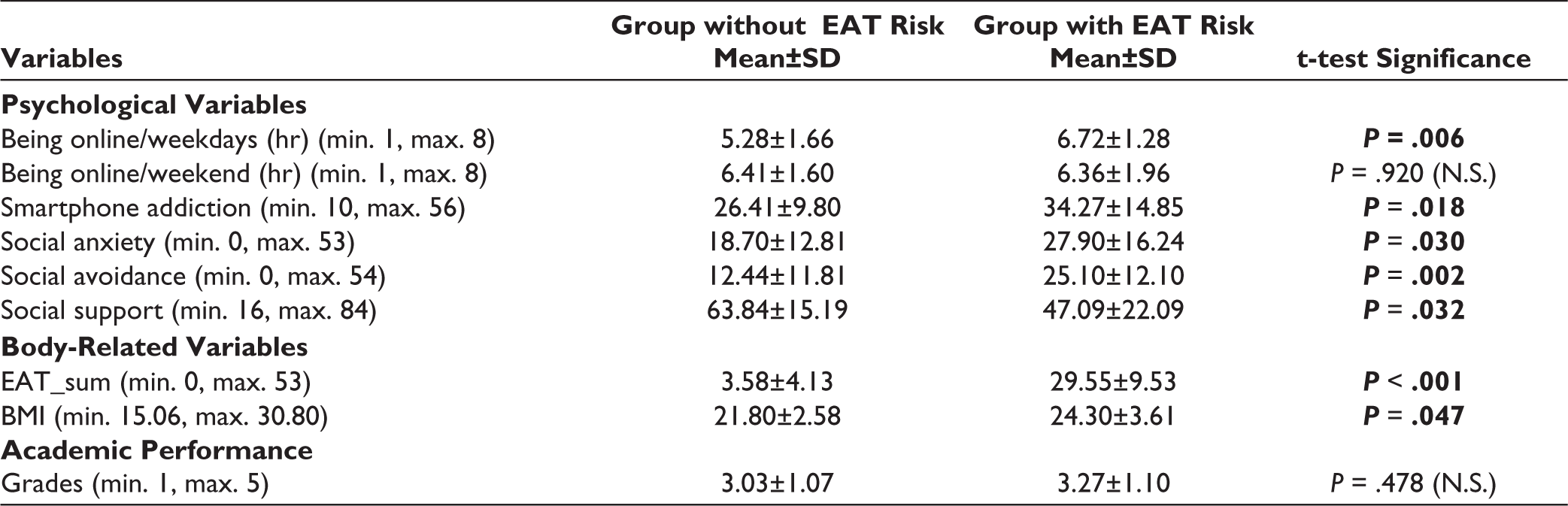
Significant differences were found in several cases. Those being at risk for disordered eating scored higher on the smartphone addiction scale [t (110) = –2.39, P = .018], social anxiety scale [t (110) = –2.20, P = 0.030], social avoidance scale [t (106) = –3.22, P = .002], eating attitude scale [t (110) = –8.94, P < .001], Body Mass Index [t (110) = –2.23, P = .047] and time spent online on weekdays [t (110) = –2.81, P = .006]. In addition, they scored lower on the social support scale [t (110) = 2.45, P = .032].
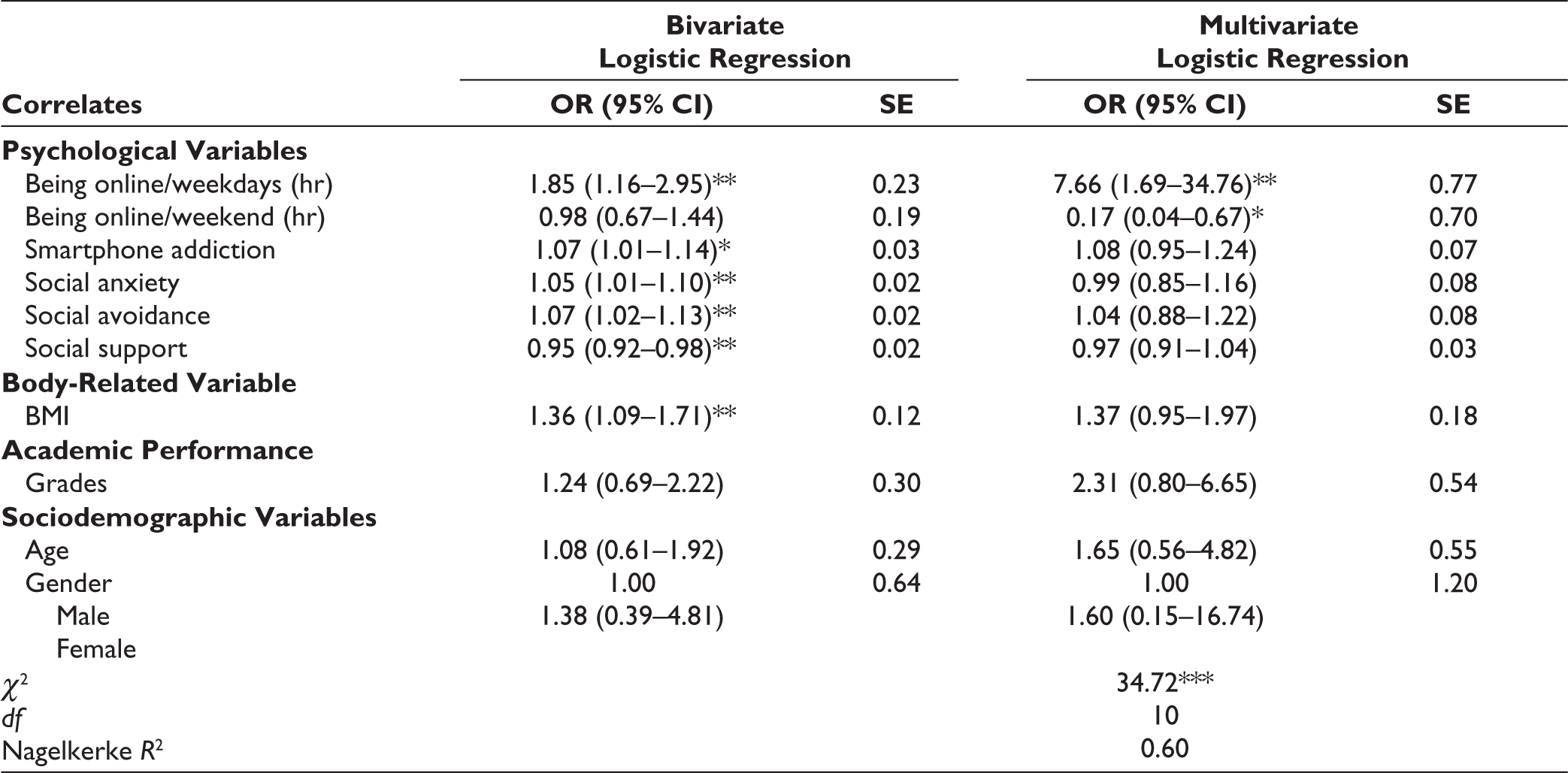
Table 3 presents the results of bivariate and multivariate logistic regression analyses. This analysis aimed to detect the risk or protective nature of independent variables determining the odds of disordered eating (as a dichotomous variable). Using bivariate calculations, being online on weekdays, smartphone addiction, social anxiety, avoidance, and social support were significant contributors, besides the BMI score. In the final multivariate logistic regression model, two variables remained significant: being online on weekdays increased (OR = 7.66, 95% CI = 1.69–34.76, P < .01), while being online on weekends decreased the odds (OR = 0.17, 95% CI = 0.04–0.67, P < .05). The goodness of fit was significant (χ2 = 34.72, df = 10, Nagelkerke R2 = 0.60).
Bivariate and Multivariate Logistic Regression Estimates for the Risk of Disordered Eating (EAT Risk).
Discussion
The present cross-sectional study aimed to further investigate potential contributors to elevating the risk of disordered eating in a sample of Indian adolescents. Namely, we aimed to examine the role of several variables determining the risk of disordered eating with special attention put on online activities (being online on weekdays and weekend, smartphone addiction) and social variables (social anxiety and social support), together with academic performance, BMI and sociodemographics. Although a growing body of research are focused on youth’ eating disorders among Indian populations,26–28 we need more research on possible correlates, particularly in terms of disordered eating without pathologizing eating behavior.
Altogether 9.8% of the students (11.3% of girls) were at risk of disordered eating which was lower than a previous result found in a study of Indian adolescents of similar ages. 5 There were no significant gender differences it EAT scores supporting previous description that eating disorders might occur regardless gender, race, age, body type or social class.1,2 However, we found significant differences in contributors between students with or without the risk of disordered eating.
Those who were at risk for disordered eating scored higher on the smartphone addiction scale and spent more time online on weekdays. This suggests that time spent online may have an important role in forming youth’s ideas about eating patterns and eating behaviors. Previous studies also reported that media messages, particularly on online platforms, were important resources for youth in the formation of their attitudes towards their body and eating patterns.16–18 Online conversation and messages, pictures and recommendations can trigger disordered eating, particularly for sensible adolescents for whom social acceptance is important. Not surprisingly, we found that students being at risk scored higher on the social anxiety and social avoidance scales, and lower on the social support scale. These findings are in concordance with other studies on social support and social anxiety.9, 11, 13 Students at risk for disordered eating also reported higher levels of BMI. This suggests that the higher the adolescents’ Body Mass Index, the more they were involved in dieting practices, although previous studies emphasized the subjective evaluation of body weight status. 23 Good academic performace did not make a difference in the risk of disordered eating directly in our study.
The main focus of our research was to determine the risky/protective nature of a set of social and other variables for disordered eating. Our results support that time spent online on weekdays, smartphone addiction, social anxiety and social avoidance as well as higher Body Mass Index elevated the risk of disordered eating, while social support served as a protection. Academic performance and sociodemographic factors (age, gender) were not significant contributors.
In the final multivariate model, only two factors remained significant contributors: being online on weekdays (positive) and weekend (negative). The most relevant finding of our study emphasizes the role of being online on weekdays, while this is not the case in terms of the weekend. One possible explanation can be a shift in students’ social connections during the different days of the week. On weekdays, adolescents are usually together with peers and their online activity is different compared to the weekend when they spend more time with family and may experience a higher level of parental control. This peer effect on weekdays may manifest in their shared attitudes towards their body and dietary behavior through personal contact and social media. Earlier studies also emphasize the role of parents in setting rules for online activity. 35 Social-emotional support from the parents would even be more important to prevent both Internet addiction and disordered eating.10–12
Study Limitations
Since our study is cross-sectional, cause-and-effect relationships could not be justified. In addition, due to the relatively small sample size and the type of school (private) these findings cannot be generalizable. We should also keep in mind that this study has been done at the time when the country was just recovering from the second peak of COVID-19 which could elevate the screentime among schoolchildren. All in all, a more detailed and elaborated model with a representative sample is necessary for future research to get a deeper insight into the background variables of adolescents’ disordered eating in India. Finally, validation of the scales on Indian population has not been undertaken yet, this is the reason for using the scales in their original (English) language. We should also mention here that we did not investigate eating disorders with a diagnosis, our findings only explored contributors to elevating the risk of disordered eating that might be also potential risk factors for eating disorders as well.
Conclusion
Although our findings are preliminary, they highlight that excessive online activity on weekdays can elevate the risk of disordered eating among Indian adolescents, while time spent online on weekends does not have a similar role. Further research is needed to clarify these associations, including leisure time spent with the family or the parents’ rules for online activities which can be protective on weekends. Hopefully these findings can trigger further examinations on the role of digital device activities and social variables.
Authors Contributions
All the authors made substantive intellectual contributions to the study. PBF was primarily responsible for drafting the manuscript, KH and PK critically reviewed it. PBF, KH and PK were involved in the conceptualization of the project. PK was responsible for data collection, PBF, KH and PK analyzed the data. All authors read and approved the final manuscript.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Doctoral School of Education, University of Szeged, Hungary (No. 4/2020).
Informed Consent
A written informed consent were received and obtained respectively before initiating the study from all participants, including parents and children.