
Abstract
Background:
Previous studies have shown that the prevalence of anxiety among primary school students in rural areas is relatively high. Also, this stage is a critical developmental stage of academic life. Childhood anxiety disorders lead to significant disruption and interference with other aspects of life, including behavioral, emotional, cognitive, and academic achievement.
Aims:
This study aimed to find the frequency of 6 subtypes of anxiety disorders and to determine the potential sociodemographic factors of anxiety disorders among primary school students in a rural area of Malaysia.
Methods:
This was a cross-sectional study in which 411 students answered the Spence Children’s Anxiety Scale-Child version (SCAS-C). Descriptive analyses elucidated at-risk students, and multivariate analysis of variance and multiple linear regression presented potential predictors of anxiety disorders.
Results:
The most common abnormal level was for social phobia (SP) (n = 109/18.6%), and the least common were panic/agoraphobia (n = 85/14.1%) and physical injury fears (PIF) (n = 82/13.6%). Multivariate analysis of variance revealed that age (P < .05), gender (P < .05), father’s employment (P < .05), and mother’s educational level (EL) P < .05) were predictors of overall anxiety. A Tukey post-hoc test revealed that older children are more likely to suffer from overall anxiety, separation anxiety (SA), SP, and obsessive-compulsive problems. Children of low-income families were less likely to suffer from SA than those of middle-income families. Children of stay-at-home mothers were less likely to suffer from overall anxiety, SA, and SP than mothers who worked more than 8 h per day. Multiple linear regression could predict 6 models of anxiety based on sociodemographic factors.
Conclusion:
According to our findings in this study, promoting mental health by providing preventive strategies and screening programs is more recommended for students with sociodemographic risk factors for anxiety disorders.
Keywords
Introduction
Pathological anxiety is a prevalent mental health disorder characterized by a persistent or considerable degree of avoidance and anxiety, associated with extensive psychosocial, developmental, and psychopathological complications.1,2 Anxiety disorders are the most common mental health condition in childhood. 3 A prevalence of 6.5% is estimated for anxiety disorders among children, making them a crucial public health concern. 4 For example, generalized anxiety (GA) disorder, separation anxiety (SA) disorder, and social phobia (SP) are the most common anxiety disorders among children, having mean prevalence rates between 2.2% and 3.6%. The prevalence of agoraphobia (1.5%) is lower, while panic disorder and obsessive-compulsive disorder (OCD) are low (ie, below 1%). 5 Childhood anxiety disorders usually tend to become chronic or long term. 6 They lead to significant impairment and interference with other aspects of life, including behavioral, emotional, and cognitive domains and academic achievement. 7 Meanwhile, rural children were more likely to suffer from mental disorders and internalizing problems. 8
To some extent, initially observed higher prevalence of anxiety among rural primary school students 9 may be the consequence of underlying differences in sociodemographic factors and characteristics among rural and urban students. The available research determines increased risk for adverse outcomes among socioeconomically disadvantaged children. However, there is little research on the prevalence of anxiety disorders and related risk factors for low-income rural children. 10
The first step in preventing and managing childhood mental disorders is to get enough information. In this regard, it is necessary to increase studies in this field in order to inform mental health policies. 10 The interplay between different etiologies, which results in the inability to regulate stress and fear, causes and maintains anxiety disorders. 11 Information on sociodemographic factors can help develop evidence-based education and prevention strategies. This information will help target these precursors and guide endogenous and exogenous effects in comorbidities. 12
Potential sociodemographic vulnerability factors were carefully selected based on a conceptual model for risk factors, which addressed endogenous and exogenous familial etiologies of internalizing disorders.13-16 According to the vulnerability-stress model, etiologies of anxiety disorders are classified into precipitating factors (such as recent stressful life events) and predisposing factors (like genetics, development, and personality). 17 In this study, the intrinsic factors investigated include demographic characteristics and acute internal lifetime events, while the extrinsic ones include socioeconomic status (SES), familial factors, and external lifetime events.
Conceptualizing dependent variables as potential anxiety disorders, that is, Age, gender, SES (family monthly income, parental EL, and father employment), major lifetime events (past: parental divorce, parental death in the previous year; recent: chronic disease and long-term medication), and family factors (birth order, number of siblings and mother’s work hours per day). Then, their correlational and regression-based effects on anxiety disorders, as an important part of mental health problems among primary school students, 18 were examined. Potential sociodemographic factors were selected based on a conceptual model of risk factors, which addresses endogenous and familial exogenous etiologies of internalizing disorders. 14
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 19 anxiety disorders include social anxiety disorder, selective mutism, GA disorder, specific phobia, SA disorder, panic disorder, and agoraphobia. The DSM-5, unlike the DSM-IV, 20 does not consider OCD to be an anxiety disorder. Despite this, OCD’s removal from the mentioned category is controversial and has been criticized (for more review, see 21 ).
There are many changes in a child’s life during middle childhood, and mental, physical, and social skills begin to develop quickly. 22 It is a critical period due to the vulnerability of children.23,24 Across cultures, middle childhood is also differentiated from adolescence largely by the onset of puberty. 25 The aim of this study was to find the frequency of 6 subtypes of anxiety disorders and to determine the potential sociodemographic factors associated with anxiety disorders among primary school students of middle childhood age in a rural area of Malaysia. Furthermore, we hypothesized that anxiety disorders are associated with endogenous and exogenous familial factors of SA, SP, OCD, GA, panic and agoraphobia (Panic/A), and PIF.
Materials and Methods
Participants
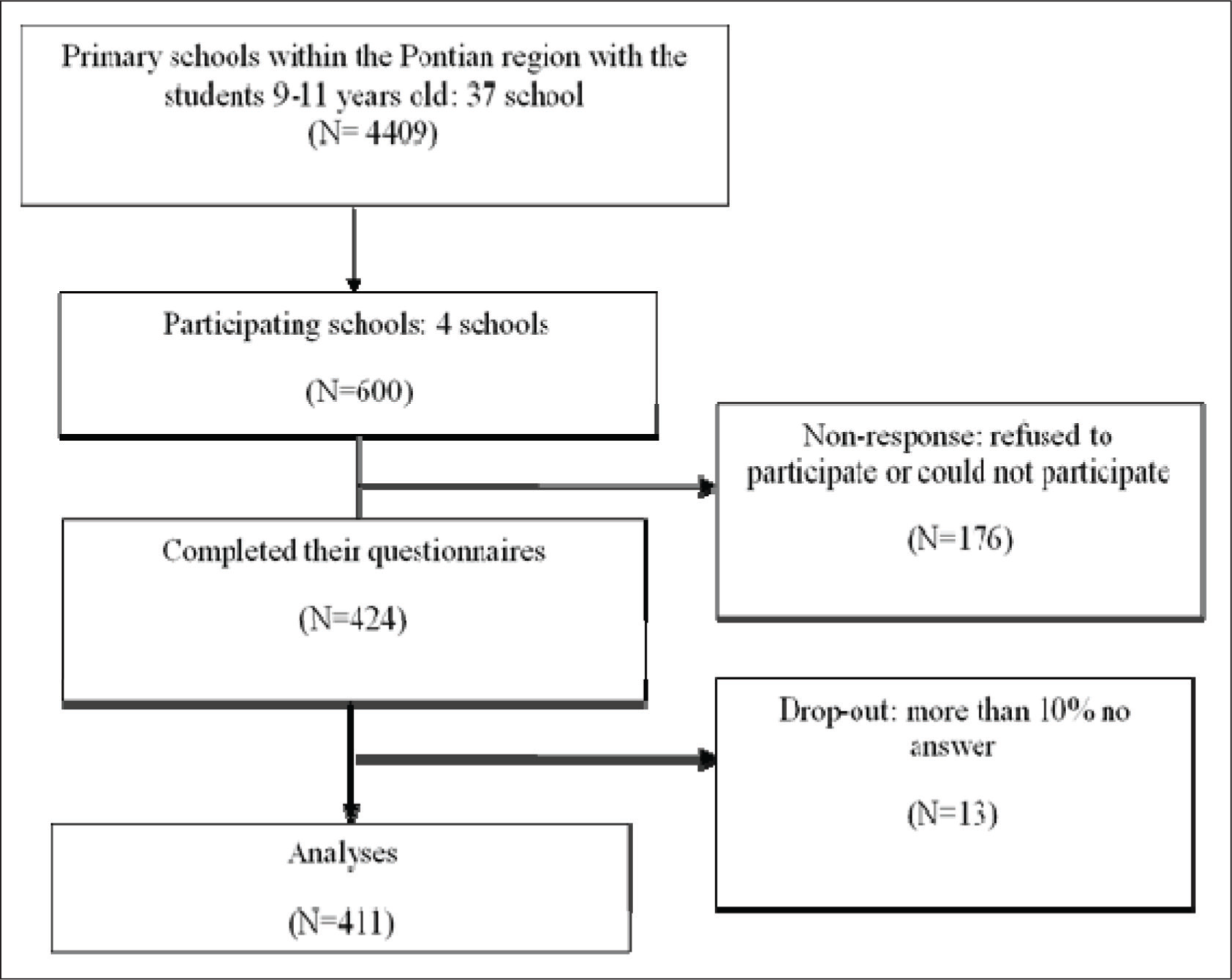
This was a cross-sectional study in which the participants were 600 children. The sample consisted of 9 to 11-year old (mean = 10.17, 53.8% female) students. They were invited to answer the Spence Children’s Anxiety Scale-Child version (SCAS-C) Malay version. The main criteria for inclusion were (1) Pontian citizens (a rural district of Johor in southern Malaysia). Participants were residents of the rural area for at least 1 year; (2) without a history of untreated psychiatric disorders; (3) only schoolchildren were aged between 9 and 11 years old. Exclusion criteria included (1) refusing to participate in the study; (2) failing to answer more than 10% of the questions on any questionnaire; and (3) people suffering from severe physical illnesses.
Procedure
The Ministry of Higher Education, University Technology Malaysia, as well as the Ministry of Education, respectively, approved this cross-sectional descriptive study. The Ethical Approval Code is FRGS/2/2013/SS02/UTM/02/6 (
Assessment Tools
Sociodemographic Information
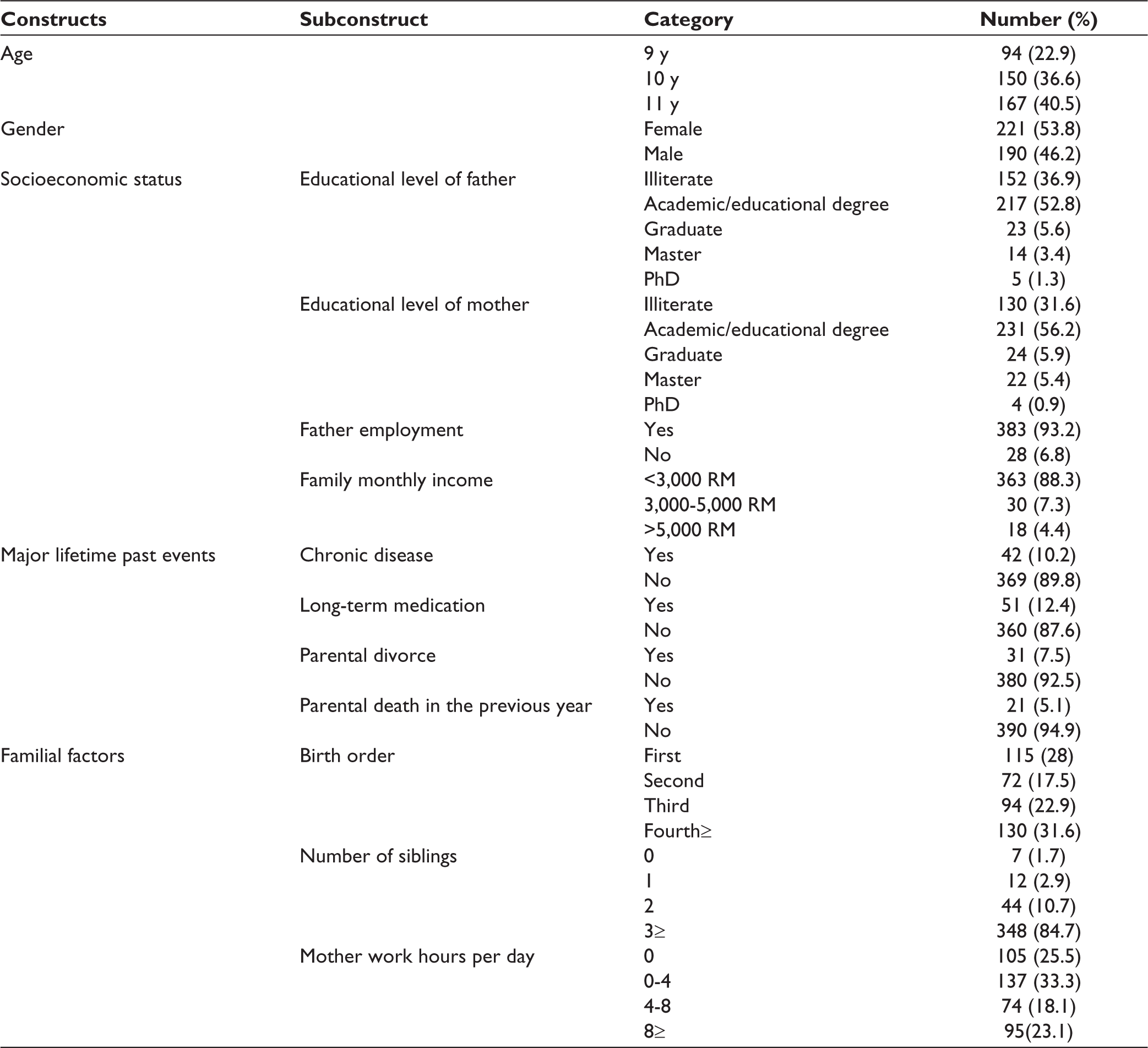
The sociodemographic checklist included the below factors: results can be seen in Table 1: age, gender, SES (family monthly income, parental EL, and father employment), major lifetime events (past: parental divorce, parental death in the previous year, recent: chronic disease and long-term medication), and family factors (birth order, number of siblings, and mother’s work hours per day).
Malay SCAS-C
The SCAS-C in this study had 44 items where 38 items were arranged into 6 subtypes: SA, SP, OCD, GA, panic/agoraphobia (Panic/A), and PIF and 6 items as positive fillers. SCAS was cross-culturally adapted into the Malay language in 2015. 26 Cronbach’s alpha was 0.86 for both SCAS versions (child and parent versions). The lowest subscale alphas were for GA, PIF, and OCD, with values of 0.50, 0.53, and 0.51, respectively. The subscale with the highest alpha was P/A, with a value of 0.68. The SA and SP subscale alpha values were 0.63 and 0.61, respectively. The total SCAS-C anxiety score and its subscale scores were significantly correlated with the total Spence Children’s Anxiety Scale-Parent Version (SCAS-P) scores. The correlation coefficient for SCAS-C against SCAS-P was 0.53. 27
Statistical Analyses
The data was analyzed with SPSS Version 22. Descriptive analysis clarified students who are at risk of anxiety disorders and the mean scores of anxiety disorders. MANOVA compared the difference between the categories of factors with all types of anxiety disorders. Finally, multiple linear regressions examined whether potential vulnerability factors predict students who are at risk of anxiety disorders.
Results
Table 1 shows the socioeconomic demographic characteristics of all 411 students in the study. There were 9, 10, and 11 years old in both genders. Most of the parents had below graduate degrees. Most of the fathers were employed. Income of most families were less than 3,000 Ringgit Malaysia. Most of the students were healthy and lived with both parents. Their birth order and number of siblings as well as their mother work hours per day are mentioned.
Socioeconomic Demographic Characteristic of Students in Real Research.
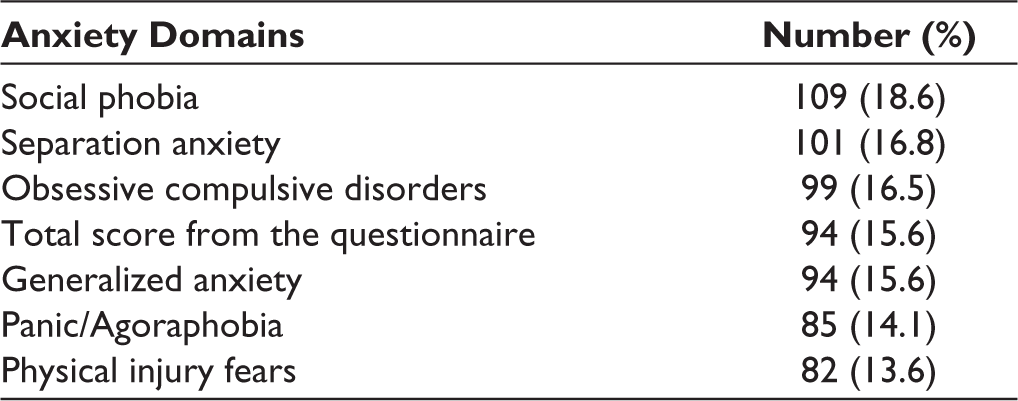
The first aim of the current study was to identify students at risk of anxiety disorders in this rural population as measured by the SCAS-C Malay version. As the author of the instrument defined, a T-score of 10 above the mean of 50 represents a value of 1 standard deviation (SD) above the mean and is indicative of subclinical anxiety. In the absence of a clinical interview, she suggests using a T-score of 60 as indicative of subclinical or elevated anxiety levels. Thus, in this research, all children who scored above a 1 SD cut-off score were considered at risk of anxiety disorders. The most common abnormal level was SP (n = 109/18.6%), and the least common was Panic/A (n = 85/14.1%) and PIF (n = 82/13.6%) (Table 2).
Frequency of Anxiety Disorders Among the Sample.
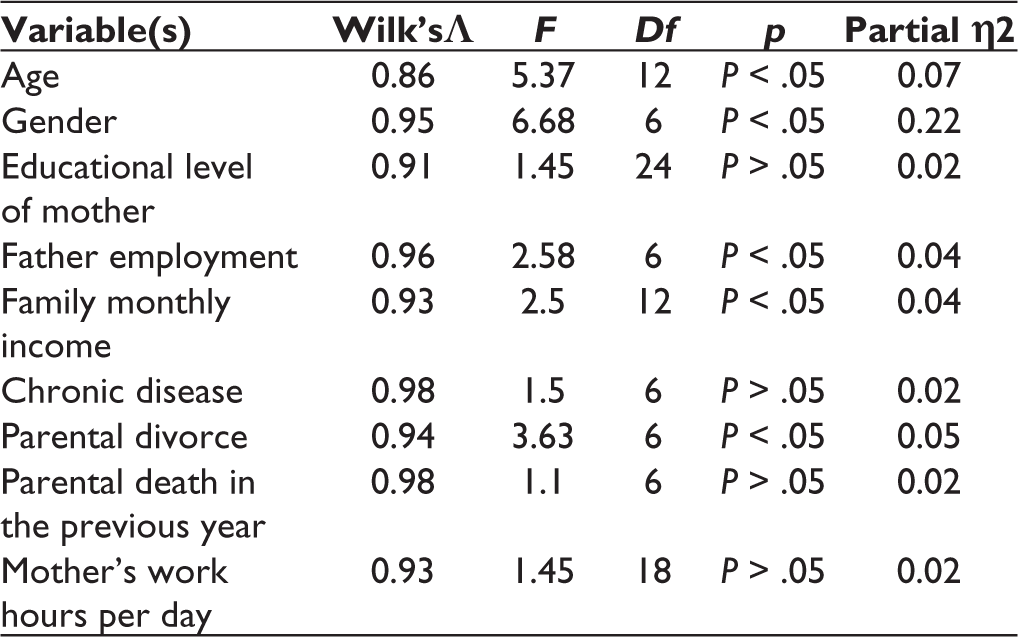
According to Table 3, a one-way MANOVA revealed a significant multivariate main effect for gender, F (6,404) = 6.68, P < .05. Girls reported more anxiety in all constructs that were significant for overall anxiety, SA, and PIF. For other types of anxiety, it was not obvious. It is significant for parental death, F (6,404) = 1.1, P < .05, too. However, all children who had experienced parental death in the previous year had nonsignificantly more symptoms of anxiety than children who had not had this experience. This difference was only significant for GA. The significance was for parental divorce, F (6,404) = 3.63, P < .05. Children of divorced parents yielded significantly less SP than children who lived with both parents. The overall score level, SA, SP, and OCD, was higher in children of nondivorced parents, and the levels of Panic/A, PIF, and GA were higher in children of divorced parents. In addition, one-way MANOVA revealed a significant multivariate main effect for father employment, F (6,404) = 2.58, P < .05. Children with unemployed fathers stated significantly higher overall anxiety, SA, and PIF levels than children who had employed fathers. Children of unemployed fathers showed a higher level of other types of anxiety. This effect was nonsignificant for chronic disease, F (6,404) = 1.5, P > .05. Children who suffered from chronic diseases reported more GA. Also, they had a higher mean score for all types of anxiety, except SA. No significant multivariate or univariate differences were found between long-term medications. There was a significant difference between age groups for overall anxiety, SA, SP, and OCD, F (12,802) = 5.37, P < .05. This test presented a nonsignificant multivariate main effect for mother’s work hours per day, F (18, 1137) = 1.45, P > .05, mother’s EL, F (24, 1400) = 1.45, P > .05, and family monthly income, F (12,806) = 2.5, P > .05. There was an obvious differentiation between the mother’s work hours for overall anxiety, SA, and SP. Children of stay-at-home mothers had the lowest level of anxiety among all groups. There was a significant difference between the levels of mothers’ EL for Panic (F (4, 402) = 4.53, P = .003). There was a significant difference between the levels of family monthly income (low, middle, and high) for SA and Panic/A. There were no significant multivariate and univariate differences between groups for other independent variables. Post-hoc test revealed older children have more overall anxiety, SA, SP, and OCD. Children of low-income families had lower SA than children of middle-income families. Children of stay-at-home mothers had lower overall anxiety, SA, and SP than children of mothers who worked more than 8 h per day.
Significant Multivariate Effects of Sociodemographic Factors.
Multiple linear regression was run to predict types of anxiety from independent variables. Related assumptions were fulfilled (Table 4).
Multiple Linear Regression Analysis of Prediction for Anxiety Disorders With Sociodemographic Factors.
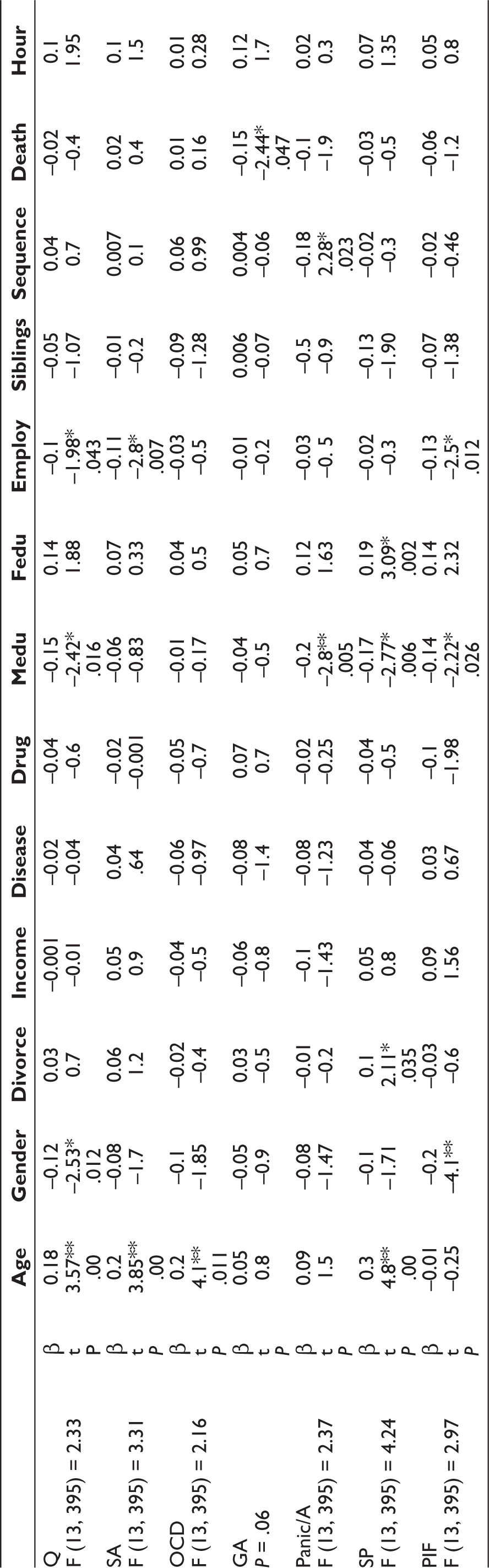
**P is significant at the .01 (2-tailed).
Model one: age (P = .00), gender (P = .012), father employment (P = .043), and mother’s EL (P =.016) significantly predicted overall anxiety, F (13, 395) = 2.33, P < .005, R2 = 0.10.
Model two: age (P = .00) and father employment (P = .007) obviously predicted SA, F (13, 395) = 3.31, P <. 005, R2 = 0.10.
Model three: mother’s EL (P = .005) and child’s birth order (P = .023) notably predicted panic, F (13, 395) = 2.37, P = .005, R2 = 0.07.
Model four: gender (P = .00), father employment (P = .012), and mother’s EL (P = .026) significantly predicted PI, F (13, 395) = 2.97, P < .005, R2 = 0.09.
Model five: remarkably age predicted OC (P = .00), F (13, 395) = 2.16, P = .011, R = 0.07.
Model six: age (P = .00), parental divorce (P = .035), mother’s EL (P = .006), and father’s EL (P = .002) predicted SP, F (13, 395) = 4.24, P < .005, R2 = 0.12.
Parental death in the previous year (P = .047) predicted GA, but the model was not significant (P > .05).
Discussion
This study showed a considerable frequency of 6 subtypes of anxiety disorders with different percentages. According to some epidemiological studies, anxiety disorders are common among primary school students,28,29 and if these problems persist and go untreated, they have negative long-term consequences. 30 The primary school stage is an important developmental stage in academic life where anxiety disorders first begin to develop or tap into the prodromal period of anxiety. 31 Screening for anxiety disorders in rural primary schools is limited in the literature. The study in rural north-eastern Uganda found that the most common prevalent anxiety disorder was SP. 32
A study that measured subtypes of anxiety by applying SCAS somehow supported this study outcome, which is that SP and Panic/A are the most and least common, respectively, among Spanish children 33 but they were secondary school students. Inconsistent with these results, in Iran, PIF was the most prevalent, and SP was the least, among the 10 to 14-year-old range. 34 Some outcomes may be related to the different age spans considered for the sample. There are substantial cultural characteristics in the epidemiology and symptomatology of anxiety disorders. In this regard, Lewis-Fernandez et al, 35 in a comprehensive review, showed the degree of cross-cultural variability in the prevalence of anxiety disorders, even when the same diagnostic instrument is applied. For instance, perception of social norms is a cultural factor that affects SP. 36 In East Asia, SP symptoms on self-reported scales are endorsed more frequently than in European schools and the United States. 37 It may be associated with a mismatch between self-constructs and culturally defined social roles. 38 Dissimilarities in personality, genetic, environmental, and demographical factors in various cultures may affect the prevalence rate of pediatric anxiety disorders. 39
For early interventions, more detailed analysis of the interplay between various endogenous and exogenous etiologies, both distal and proximal to the child, is necessary. 40 In this research, a significant difference between male and female students for the risk of some anxiety disorders was supported by Malak and Khalifeh, 41 who did not focus on subtypes. Gender-based differences may emanate from biomedical, psychosocial, cultural, social, and developmental processes.42,43
Sometimes, older students showed less anxiety related to more psychological adjustment in mental development, 44 but this study presented similar results to Abbo et al. 32 It seems that fears of failure, criticism, social threats, being kidnapped, and school and test performance increased with age. 45 Although this is not a longitudinal study, it does provide some insight into the progression of anxiety disorders in middle childhood.
Stressful life conditions can cause negative biological and health outcomes in children. Surprisingly, in terms of life events, nondivorced parents had children with more SP in this study, which is not supported by literature. 46 Single-parent students are not only obliged to be in contact with others with less parental support but they also have more social responsibilities in comparison with 2-parent students. Both explanations may help them enhance their social skills while they get rid of severe familial and parental conflicts. In addition, sometimes the elimination of severe marital conflicts after divorce reduces students’ SP.
The association between most of the risk for anxiety disorders and suffering from a chronic disease is somehow consistent with the previous findings, which elucidated very strong evidence for the association between physical illness and anxiety. 47 Martinez and Ercikan 48 did not find any relationship between chronic diseases in childhood and emotional disorders.
In this study, a significant correlation between parental death and the risk of GA may be related to students’ fear of abandonment by a parent on whom they cannot rely for future care. 49 In this support, Himaz 50 stated that middle-aged students parents’ deaths influence subjective well-being and psychosocial characteristics.
Some studies showed the social-educational environment of the family has a significant influence on developing pediatric fears and anxiety. 51 This study illustrated some of these deficiencies, even though this rural community was somehow homogeneous and predominantly low class. Mother’s EL is included in the model of anxiety prediction for overall anxiety, SP, Panic/A, and PIF. Moreover, the father’s EL was a predictor for the SP model. Lower anxiety in children with middle-educated parents compared to children with low- educated parents is supported by some previous studies. 32
There were no differences between students with high- and middle-educated fathers in some previous research. 52 Although, our outcome may be justified in that higher expectations and more limited child-parent relations in families with highly educated parents might lead to more anxiety than students of middle-educated parents. 53
In this research, students from low-income families had lower SA than students from middle-income families, but income could not significantly predict any anxiety disorder types. Unlikely, middle socio-economic students in India presented more anxiety than those from low and high socio-economic families. 53 Karlsen et al 54 stated that SP has the strongest association with SES among all students’ anxiety disorders. Children of middle-educated parents had the lowest mean scores of all types.
The father’s unemployment not only predicts his anxiety but also the anxiety of his offspring. 55 Low-SES children with unemployed fathers grow up in environments that lead them to think about life as a threatening occurrence. Further, children of unemployed fathers are more likely to encounter adverse life events. 51
Students whose mothers worked more than 8 h per day had a significantly higher risk of overall anxiety, SA, and SP than children whose mothers stayed at home. The prolonged separation of a mother creates emotional distress for students, but nonprolonged separation decreases students’ anxiety. By the way, many studies support that working mothers have more anxiety related to their job and could transfer it to their children. 55 However, other researchers found no association between mothers’ work hours and children’s behavioural problems. 56 Interestingly, in current research, the level of anxiety disorders has shown increasing trends due to mothers’ working hours in most of the domains.
In this research, there was no significant effect of the number of siblings on anxiety disorder models. Regarding GA, there are opposite findings; only-children had more anxiety 57 and less anxiety than sibling-children. 58 Previously, not only was the protective effect of siblings on reducing psychiatric morbidity not observed but also whenever family size increased above 3 (large family size), psychiatric morbidity increased. 59
Simply put, children in their final years of primary school, females, students with unemployed fathers, uneducated parents, and full-time working mothers require more consideration than students in their middle grades of primary school, males, students with employed fathers, educated parents, and stay-at-home mothers. The mother’s EL had a significant effect on anxiety prediction, demonstrating the importance of mothers’ knowledge and literacy on their children’s mental health. Overall, the role of SES factors in the models of anxiety disorders attracts the views of the government on promoting the level of indicators of SES among rural students when they aim to elevate their mental health.
A few studies in Asia focus on rural areas across a large sample. In the present study, socioeconomic factors were investigated in relation to 6 dimensions of anxiety disorders using a large sample and rural areas. However, some limitations have to be considered. First of all, this study was held in a rural area. Therefore, the results cannot be easily generalized to all rural and urban locations. Future studies could replicate our findings using samples of children drawn from urban areas. In addition, a 1-time assessment was conducted for each participant in this study. Finally, some children and their parents did not participate in the study.
Conclusions
According to studies, internalizing disorders are becoming more common among students. Mental disorders, such as pathological anxiety, are prevalent. It is linked to many psychological, developmental, and psychopathological issues. This study attempted to highlight rural students who are exposed to anxiety disorders. Therefore, it is necessary to identify students with characteristics such as females, students from higher grades, children of illiterate parents, children who experienced parental death, first birth order, and high birth order children. In addition, it is recommended to provide early screening programs for students who show mental health difficulties and are suspicious of anxiety disorders. A whole-school program using some of the suggested strategies is recommended.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University Technology Malaysia (UTM) for financial support of this research under Institutional Grant, VOT: 4F304.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.