
Abstract
Background:
The Child and Youth Resilience Measure-28 (CYRM-28) is one of the few measures based on a contextually and culturally embedded understanding of resilience. However, its psychometric properties have not been examined in India which is home to the largest proportion of adolescents worldwide. The present study was conducted to address this gap.
Aims:
This study examined the psychometric properties and factor structure of the English and Hindi translated version of the CYRM-28 in the Indian context. Additionally, it investigated the role of select sociodemographic factors on the resilience levels of Indian school-going adolescents.
Method:
Using convenience sampling, data were collected from 1281 adolescents (mean = 15.28 years; SD = 1.08) enrolled in private and government schools in rural and urban parts of Northern India. Three measures were used in this study: CYRM-28, Warwick-Edinburg mental well-being scale (WEMWBS) and PERMA. Descriptive statistics, confirmatory factor analysis, reliability analysis, correlation, and multivariate analysis of variance were conducted to validate the scale and to study the effect of sociodemographic factors on resilience levels of India adolescents.
Results:
A 16-item (English and Hindi) version of the CYRM-28, with a three factor-structure was found to be the most adequate fit for the Indian context. It demonstrated good reliability and convergent validity with the WEMWBS and PERMA. Further, the multivariate results, albeit with a small effect size, showed a significant main effect for place of residence and age, with urban and older adolescents obtaining higher resilience scores than their rural and younger counterparts.
Conclusion:
The present research shows that a shorter 16-item version of the CYRM with a three-factor structure is a reliable and valid tool for use among Indian adolescents. The CYRM is a robust resilience measure being used across varied cultures—its validation in the Indian context widens the scope for resilience research in the Indian adolescent population.
Introduction
The empirical understanding and measurement of resilience, and its risk and protective factors among children and adolescents are critical in contemporary times given that children and youth worldwide are currently exposed to numerous threats to their well-being. 1 Psychological findings on resilience have significant implications in this regard as empirical studies demonstrate a strong and consistent association between resilience and mental well-being. 2
Moreover, a large and growing body of psychological literature on the risk, protective, and promotive factors on resilience focuses on identifying those factors that may be enhanced or addressed through interventions and relevant youth policies. 3 However, the initial understanding of the resilience factors centered around individual resources as was reflected in some of the initial scales that were developed for measuring resilience (e.g., CD-RISC 4 ). Such an exclusive focus on individual level factors undermines the significance of the contextual and cultural factors influencing resilience. In particular, scholars are increasingly emphasizing the role of culture in resilience. 5
It has been argued that each culture has its unique strengths, which in turn bolster the resilience of the people belonging to that culture. Further, the relative importance of the protective factors of resilience, their expression, and the ways in which they strengthen resilience may also vary greatly between cultures. 6 Taking cognizance of this complex nature of resilience, 7 over time, there has been a shift towards a more socio-ecological understanding of resilience and its factors. 8 Accordingly, the conceptualization of resilience has been expanded to include an individual’s ability to steer their way to psychological, physical, and sociocultural resources that bolster their well-being as well as their ability— individually and collectively—to bargain for these assets in culturally relevant ways. In line with this contextually and culturally embedded understanding of resilience, Ungar and Liebenberg 9 constructed the Child and Youth Resilience Measure - 28 (CYRM-28), which adopts a socio-ecological perspective in examining the resources available to youth for augmenting their resilience levels. While its culturally sensitive nature and transnational relevance has been highlighted by Windle et al., 10 they have called for more validation studies given the insufficient evidence for its construct validity.
Given the cross-cultural relevance of the construct, CYRM-28 has been validated across different countries. However, across cultures, differences in factor structures have been observed. In the original validation study, 11 a 3-factor structure is reported: individual capacities or resources, relationship with primary caregivers, and contextual factors. However, validation studies in other cultural contexts do not have a consensus on its factor structure. 12 For instance, the examination of the psychometric properties of the CYRM-28 in New Zealand 13 showed a four-factor model as having a better fit than the original 3-factor model. The original factor structure was also not a good fit in the Spanish 14 and Australian settings. 15 Other validation studies have shown a varied number of items as being more appropriate, such as a 3-factor model with 11 items was found to be most appropriate in the Iranian context, 16 and a 3-factor structure with 24 items showed a better fit than the 28-item version of the CYRM in South Africa. 17 Thus, the extant literature indicates a lack of consensus regarding the factor structure of CYRM-28 across cultures, which merits deeper exploration.
While validation studies of the CYRM-28 have been conducted across various nations and cultural contexts, it has not yet been validated in India, although India was among the 11 countries from where data was collected for its initial development. 9 Despite not being validated, some studies using the CYRM-28 are reported in the Indian literature on resilience.18,19 However, these studies neither confirmed its factor structure in the Indian context nor documented its psychometric properties. As highlighted previously, different factor structures emerged from the validation studies of the CYRM-28 in different cultural contexts; hence, it becomes imperative to establish its construct validity and examine its psychometric properties in India, both in English and in Hindi, as Hindi is the most widely spoken and understood language in our country (43.63%). 20
Additionally, examining the sociodemographic correlates of the resilience levels of Indian adolescents is equally important as it can help understand the needs of different groups of adolescents. Such findings can guide researchers and practitioners in developing culturally tailored resilience interventions and providing policy recommendations relevant to Indian adolescents. However, currently, there is a dearth of studies examining the impact of socio-demographic factors on the resilience levels of Indian adolescents. Further, there is an inconsistency in the existing findings regarding the association between resilience and sociodemographic factors among adolescents across different cultures. For instance, some studies have found a significant association between resilience and sociodemographic factors such as age and sex,
21
type of schooling (private versus public), and area of residence (rural versus urban).
22
However, some studies have not found any significant association between resilience and sociodemographic factors such as gender
23
and type of schooling.
24
Such inconsistent findings warrant further investigation. Thus, the present cross-sectional study had a twofold aim:
First, to assess the psychometric properties and factor structure of the English and Hindi translated version of the CYRM-28 in a sample of Indian adolescents, and Second, to examine the effect of sociodemographic factors, including age, gender, place of residence (urban versus rural), and type of schooling (private versus public/government), on the resilience level of Indian adolescents.
Method
Study Design and Participants
Using convenience sampling, data was collected from 1281 school-going Indian adolescents for the present cross-sectional study. Initially, the data booklets were distributed amongst 1294 students, of whom 13 students did not return the filled questionnaires. Hence, the final sample comprised 1281 adolescents aged between 13 and 18 years (mean = 15.28 years; SD = 1.08), of whom 50.5% were male and 49.5% were females, 46.3% were from an urban background and 53.7% were from a rural background, 48.2% attended private schools and 51.8% attended government schools. Further, 16.2% of the participants were in the ninth standard, 49.3% were in the tenth standard, 27.5% in the eleventh standard, and 6.9% were in the twelfth standard. A total of 3% of the participants were in standard 8 and less, with the minimum being standard 5. Lastly, 48.87% of the participants responded to the English data booklet, and 51.13% responded to the Hindi data booklet.
Measures
Child and Youth Resilience Measure—28 (CYRM-28 9 )
As noted above, this is a 28-item culturally-sensitive resilience measure. The scale items are rated on a 5-point Likert scale (1 = does not describe me at all and 5 = describes me a lot), and the respondents must indicate the extent to which each statement describes them.
Warwick-Edinburg Mental Well-Being Scale (WEMWBS 25 )
This 14-item unidimensional scale comprises only positively worded items pertaining to positive mental health. It assesses both eudemonic and hedonic aspects of well-being related to positive affect and functioning. This scale is suitable for use with participants aged 13 years and above. The scale items are rated on a 5-point Likert scale (1 = none of the time to 5 = all of the time) and evaluate the respondent’s mental well- being over the past 2 weeks. While the original version of this scale yielded internal consistency reliability of 0.89 in a UK student sample, comparable reliability of 0.84 was found in the Indian student sample. 28
PERMA 26
PERMA stands for positive emotions, engagement, relationships, meaning, and accomplishment and represents the PERMA model of well-being conceptualized by Seligman. 27 The multidimensional 49-item PERMA measure was developed and validated by Kern et al 26 in a sample of 516 Australian school students aged 13-18 years. It assesses both positive and negative aspects of well-being and comprises 4 well-being and 2 ill-being factors. The well-being factors include positive emotion, engagement, relationships, and accomplishment, and these represent 4 out of the 5 factors of the PERMA model of well-being. 27 The ill-being factors, on the other hand, include depression and anxiety. Respondents must indicate the extent to which they endorse the statements on a 10-point Likert scale (1 = not at all to 10 = completely), considering their experiences over the past month. A reduced 34-item version of this measure was found to be most appropriate for use among Indian adolescents. 28 In its Indian validation, Cronbach’s alpha values of the six factors ranged from 0.80 to 0.92. 28 In the original study, 26 the values ranged from 0.68 to 0.92.
Procedure
Test Translation
The CYRM-28 was translated to Hindi, adhering to the standard forward and backward translation procedure. 29 First, 2 bilingual experts worked independently on its forward translation. Then, 2 other bilingual experts worked on its backward translation. After that, the authors resolved the discrepancies between the 2 translations in consultation with the 4 bilingual experts. The final version of the tests was administered to the present sample.
Recruitment and Data Collection
The research team approached various private and government schools in different regions of Delhi NCR, Haryana, Rajasthan, and Uttar Pradesh for data collection. The schools that permitted the research team to collect data during school hours were given a formal letter outlining the study objectives and the consent form. Afterward, an introductory session was held with the students from grades 5 to 12 in the presence of their class teachers on a predetermined date and time.
The students who expressed interest in research participation stayed back and were explained the purpose of the study and the voluntary nature of their research participation. They were also assured of the confidentiality and anonymity of their responses and their right and autonomy to withdraw their participation at any stage. Following the provision of informed consent/assent, the data booklets was distributed among these interested students.
Two types of data booklets were prepared for this study—1 in English and 1 in Hindi. The interested and consenting students could participate in this study in either of the languages, depending on their linguistic proficiency and comfort (626 participants responded in English and 655 responded in Hindi). Both the English and Hindi booklets consisted of a consent/assent form, a demographic information sheet (age, sex, grade, area of residence, school type), and the selected measures of resilience and well-being.
The research team, as well as the class teachers, were present throughout the data collection process. After distributing the data booklets, the participants were given detailed verbal instructions for responding to the consent/assent form, study measures, and demographic information sheet. The research team was available to answer the queries of the participants regarding any statement or question in the data booklet.
Ethical Consideration
Cross-sectional survey-based research such as the present one is typically exempted from the Institute Ethics Committee approval under 45 CFR 46.101(b) Categories of Exempt Human Subjects Research. All procedures involving human participants in this research were in line with the 1964 Helsinki Declaration and its later amendments. As emphasized previously, apart from the approval of the school authorities, informed consent/assent of the participants was sought and obtained. Besides, the information obtained from the participants were recorded and analyzed anonymously and they were not identified directly or through any identifiers linked to them.
Data Analysis
Firstly, the percentage of missing values was ascertained using Statistical Package for Social Sciences (SPSS) version 20.0. Since it was less than 5%, the missing values were imputed using regression analysis as recommended by Tabachnick and Fidell (2007). 30 After that, descriptive statistics, confirmatory factor analysis (CFA), reliability analysis (Cronbach’s Alpha), correlation analysis (for convergent validity), and multivariate analysis of variance (MANOVA) were conducted.
For ascertaining the convergent validity of the CYRM, correlations were computed with two well-being measures: the WEMWBS and PERMA, and for MANOVA, the benchmarks for interpreting the effect size (partial eta squared) were 0.01, 0.06, and 0.14, representing a small, medium, and large effect size, respectively. 31 SPSS was used for descriptive statistics, reliability analysis, and MANOVA; R version 3.3 was used for confirmatory factor analyses and invariance testing.
Results
Confirmatory Factor Analyses of the CYRM Scale
At the outset, we conducted preliminary item analyses for the English version (n = 626) and the translated Hindi version (n = 655) of the CYRM. The analyses revealed that the item means ranged from 3.83 to 4.56 (SD: 0.82-1.08) for the English version and between 3.87 and 4.61 (SD: 0.74-1.10) for the Hindi version. The absolute skewness (English: –2.04 to –0.59; Hindi: –2.23 to –0.58) and kurtosis (English: –0.81 to 3.80 to 0.67; Hindi: –0.24 to 5.63) were also examined in order to check for possible non-normal distribution of scores. However, the skewness (< 2.0) and kurtosis (< 7.0) were in the acceptable range, which indicated a normal distribution of the scores.
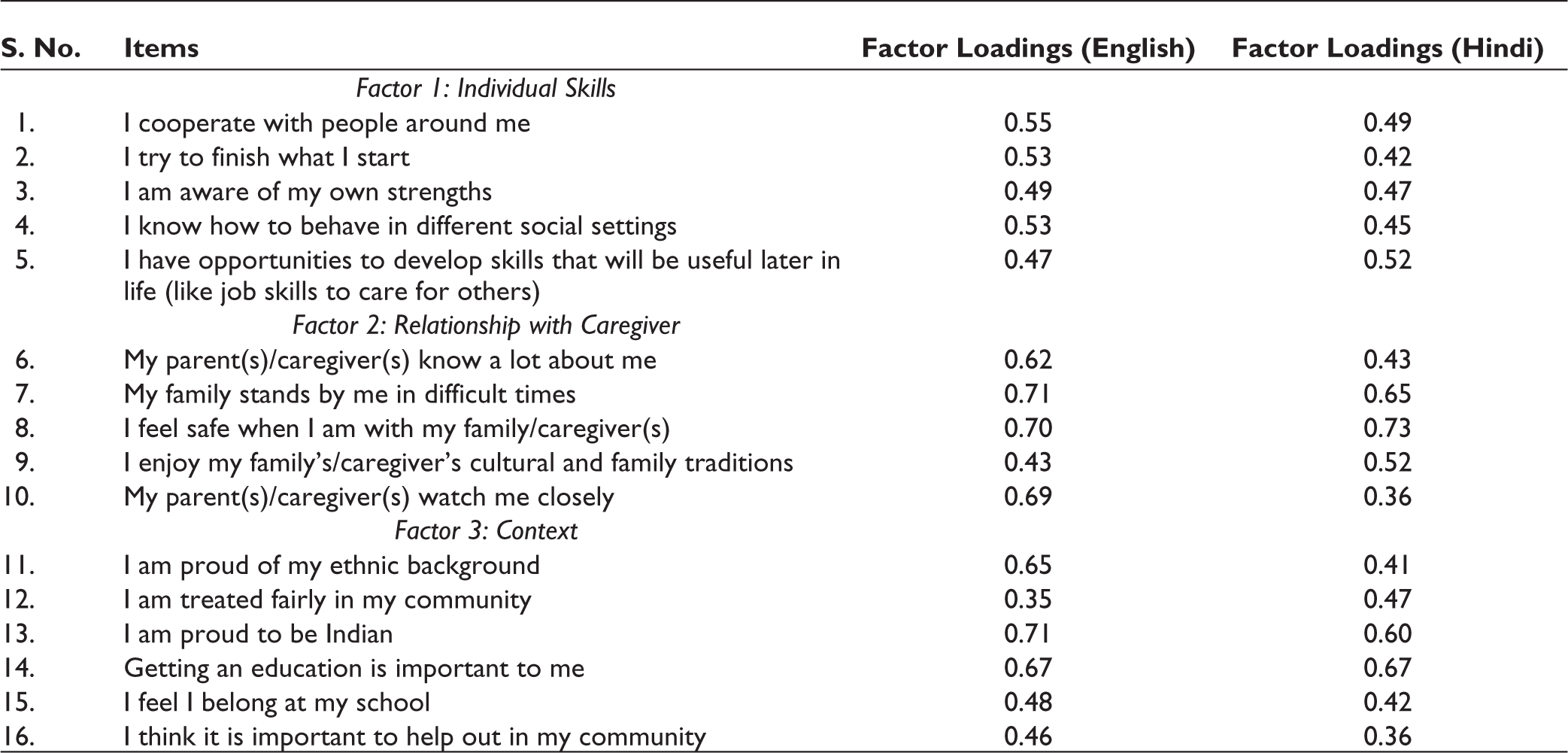
Out of the original 28 items of the CYRM scale, 16 items were retained after the deletion of 12 items from the original pool based on the values of factor loadings (values less than 0.30 were deleted). With these 16 items, the model fit the data to an acceptable level for both English (n = 629; χ2 (120) = 2604.55, P < .001, CFI = 0.93, RMSEA = 0.06, SRMR = 0.05) and Hindi versions (n = 659; χ2 (120) = 2047.16, P < .001, CFI = 0.88, RMSEA = 0.06, SRMR = 0.05) (see Table 1). We also conducted measurement invariance testing across languages. The specified model achieved metric invariance which indicated that the items were sufficiently invariant across groups. We used the Hirschfeld and Von Brachel 32 criteria to establish invariance, with ΔCFI values that exceeded 0.01 being understood as an indication of the same (for detailed results, see Table 2).
Final Items of the CYRM Scale.
Results of Measurement Invariance Testing Across Languages.

X
Reliability and Convergent Validity
The scale shows acceptable reliability. Cronbach alpha for 16 items scale was 0.86 for the English version and 0.82 for the Hindi version, which shows high reliability. We computed correlations with PERMA and WEMWBS scales to establish convergent validity. The CYRM scale and all its dimensions correlated significantly and positively to PERMA and WEMWBS scales, indicating the convergent validity of the CYRM scales. Detailed information on descriptive statistics and convergent validity appears in Table 3.
Descriptive Statistics and Convergent Validity.

**P < .01; Cronbach alpha values appear across the diagonal in brackets and bold. CYRM indicates mean resilience scores. CYRM/WEMWBS/PERMA = overall descriptive statistics, individual, caregiver, context = factor wise descriptive statistics.
Demographic Variables and Resilience
To study the relationship between our selected demographic variables, namely age (ages 13-15 years; mean = 3.85 and ages 16-18 years; mean = 3.96), gender (male mean = 3.89 vs female mean = 3.89), place of residence (rural mean = 3.74 vs urban mean = 4.07), and schooling (government mean = 3.87 vs private mean = 3.93), and various domains of resilience in the CRYM scale, namely, individual skills, relationship with caregivers and context, multivariate analyses was used.
Results from the multivariate analyses indicated a significant main effect for age and place of residence. The effect sizes, however, were small. Further, a significant main effect of small size was also observed for the interaction of age and place of residence, and sex and place of residence, and for a 3-way interaction between sex, school type, and place of residence. For complete results, see Table 4.
Main Effect of Demographic Variables on Resilience.a

aDependent variable = mean resilience score on CYRM.
Multivariate analyses also revealed that individual skills, relationship with the caregiver(s), and context had a greater impact on the resilience levels of rural children than urban children. All these factors were also more crucial at a younger age (13-15 years) compared to ages between 16 and 18 years. Results of multivariate analyses are summarized in Table 5.
Effect of Demographic Variables on Different Resilience Indicators.
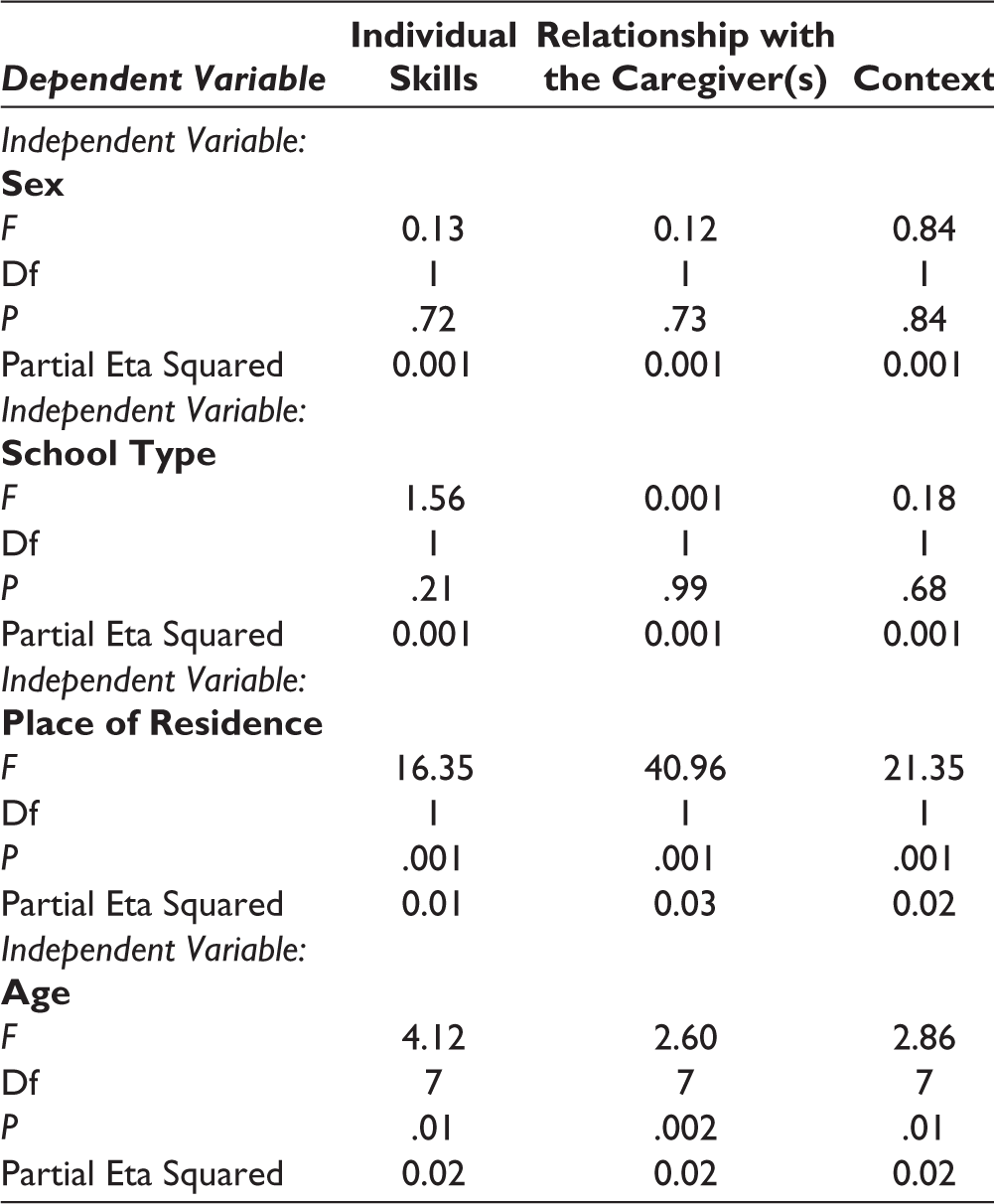
Resilience indicators (CYRM) = individual skills, relationship with the caregiver(s) and context
Demographic variables = sex (coded 0 = male, 1 = female), school type (coded 0 = government/public and 1 = private school), place of residence (coded 0 = rural, 1 = urban) and age (coded 0 = 13-15 years and 1 = 16-18 years).
Discussion
This study presents the psychometric properties of the English and Hindi translated versions of the CYRM-28 in a sample of Indian adolescents. A brief 16-item version of the CYRM with a 3-factor structure exhibited a good fit in the Indian context. The 3 factors of the CYRM derived from the present research were individual skills, relationship with caregiver(s), and context, thus, confirming its original factor structure in the Indian context.
Similar to the results of the present Indian validation, an Iranian 16 and a South African validation study of the CYRM-28 17 also found a shorter version of this measure to be more appropriate in their respective cultural contexts. While the Iranian study found an 11-item version to be a good fit in the Iranian context, the South African validation showed a 24-item version to yield a better fit in the South African context. Furthermore, consistent with our findings, the 3-factor structure was also confirmed in these studies.
On the other hand, the validation of the CYRM-28 in Nicaragua (a Central American country) found a 21-item version of the CYRM with a 6-factor structure to have a better fit than the 28-item measure and its 3-factor structure. 33 While validation studies of the CYRM in India, Iran, South Africa, and Nicaragua yielded a shorter version as more culturally appropriate, a Spanish validation study found a longer 32-item version of the CYRM with a 3-factor structure as having a better fit compared to the 28-item version. 14
Contrary to these results, validation studies of the CYRM-28 in Jamaica 34 and New Zealand 13 retained all 28 items of the original measure. However, these studies found a 4-factor structure to be more relevant and appropriate in their respective cultural contexts. On the other hand, a Persian 35 and Dutch validation 36 of the CYRM-28 not only retained all 28 items but also confirmed its original 3-factor structure.
To the best of our knowledge, the present study is the first to have examined the psychometric properties and factor structure of the CYRM-28 in India. The brief 16-item version of the CYRM that emerged as having a good fit in the Indian context demonstrated good reliability and convergent validity, as evident from its significant positive correlation with measures of well-being, namely PERMA and WEMWBS. Existing studies also report a positive relationship between resilience and well-being,2,37 thus supporting the present findings.
The present research also examined the effect of select sociodemographic factors on the resilience levels of Indian adolescents. It was observed that there was no significant main effect of gender on resilience scores which is consistent with some existing findings.23,38 In contrast, a few other studies21,39 have found gender to be a significant sociodemographic variable impacting the resilience level of adolescents.
We also did not find any significant impact of the type of schooling on resilience levels. Contrary to our findings, Singh et al 28 found the type of schooling to have a significant association with adolescents’ resilience levels. Adolescents studying in private schools were found to have lower levels of resilience in their study. The type of schooling has not been subject to much systematic investigation as a sociodemographic variable impacting resilience, and these inconsistent findings warrant further investigation.
In contrast to gender and type of schooling, age (early and late adolescence) and place of residence (rural versus urban) were found to have a significant main effect on resilience levels. This is in line with previous studies showing a significant association of resilience with adolescents’ age 21 and their place of residence. 28
Interestingly, the present findings show that the younger adolescents obtained lower (mean) scores on all 3 resilience factors, namely individual skills, relationship with the caregiver(s), and context. Consistent with the present finding, existing studies on the adolescent population reveal that early adolescence is characterized by greater challenges and developmental transitions than late adolescence. 40 In light of the challenging transitions and potential for developing mental health problems, 41 resilience and its protective factors acquire greater significance during early adolescence.
The study findings also reveal the significance of these resilience factors (namely, individual skills, relationship with caregiver(s), and context) for rural adolescents relative to their urban counterparts. In contrast, a study on Nepalese adolescents showed that living in an urban area was associated with having lower resilience levels than living in a rural area. 28 On the other hand, existing research from India 42 shows no significant difference in the resilience levels of rural and urban adolescents. However, given the paucity of Indian studies on the role of socio-demographic variables on the resilience level of adolescents, future research is warranted.
Overall, the present multivariate results suggest that the protective factors of resilience need to be strengthened among rural Indian adolescents and those in the early adolescence phase. However, although the present research found a significant main effect of age and place of residence on resilience scores, the effect sizes were small. The P value reveals whether an effect exists, ie, whether or not there is statistical significance. However, to understand the size of the effect and its practical significance, one must examine the effect size, and scholars are increasingly emphasizing the importance of measuring and reporting effect sizes. 43 In sum, in the case of the present multivariate findings, the obtained P values should be considered in light of their effect sizes.
The results of the present study must also be understood within the context of its limitations. One of the key limitations was the lack of inclusion of at-risk adolescents, including the homeless, tribal adolescents, school drop-outs, substance abusers, and juvenile delinquents. Further, the data was collected predominantly from the Northern Indian region. Data collected from all segments of the adolescent population belonging to different Indian states/regions would have made the findings more generalizable and given a more nuanced understanding of resilience in Indian adolescents.
Footnotes
Acknowledgements
This research was part of a project that was founded by the Indian Council of Social Science Research (ICSSR). All the authors would like to thank the ICSSR for funding this project, and all the schools and their students for their research participation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was supported by the Indian Council of Social Science Research (ICSSR) [Grant number: RP03106].
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.