
Abstract
Objectives:
To study the prevalence of sleep deprivation (SLD) and associated risk factors among school-going adolescents of 9th to 12th grades (13-18 years) in an urban setting in Thiruvananthapuram, Kerala, India.
Study Design:
Descriptive, cross-sectional study.
Methodology:
The participants were selected through random sampling. Self-administered structured questionnaire focusing on sleep habits, study habits, before bed screen-time, and parental sleep habits was administered to them. Weight and height were measured to calculate Body Mass Index.
Results:
Out of the 426 students, 29 were excluded and 302 students (76.07%) had SLD. Mean age was 15.79 years (standard deviation: 1.23). Univariate analysis showed adolescents above 15 years (odds ratio [OR] = 2203, 95% confidence interval [CI]: 1.380-3.517), students of 11th and 12th (OR = 2.205, 95% CI: 1.380-3.523), sleeping after 10 PM (OR = 19.617, 95% CI: 10.586-36.355), waking up before 6 AM (OR = 2.586, 95% CI: 1.554-4.304), sleeping after parents (OR = 2.356, 95% CI: 1.415-3.922) had significant risk.
On multivariate analysis, students of 11th and 12th (adjusted OR [aOR] = 3.197, 95% CI: 1.107-9.234), going to bed after 10 PM(aOR = 51.49, 95% CI: 20.211-131.180), waking up before 6 AM (aOR = 51.49, 95% CI: 20.211-131.180), and sleeping after parents (aOR = 1.927, 95% CI: 1.011-3.673) were significant.
Conclusion:
Prevalence of SLD among adolescents aged 13 to 18 years was 76.07%. Higher secondary classes, going to sleep after 10 PM, waking up before 6 AM, and sleeping after parents had significant SLD. Good sleep habits can be promoted by including their importance in school curriculum.
Introduction
Adolescence is a critical period of normal growth and development during which gradual transition from childhood to adulthood occurs with onset of puberty and related maturation. 1 Along with many other processes, sleep plays a key role in adolescence as their neurohormonal milieu undergo dramatic maturation and regulation during the sleep state. 2
The American Sleep Association (ASA) defines sleep deprivation (SLD) as “not obtaining adequate total sleep.” 3 The American Academy of Pediatrics (AAP) has endorsed Childhood Sleep Guidelines by ASA and recommends that adolescents aged 13 to 18 years should get 8 to 10 h of sleep per 24 h regularly to promote optimal health. A panel of 13 experts in sleep medicine used a modified RAND Appropriateness Method to develop these recommendations.4, 5
Various sociocultural and environmental factors are responsible for changes in sleep pattern. 6 Psychosocial factors like academic and social demands,7–9 physiological concomitants of puberty, 8 and environmental factors like reduced parental influence on bedtimes, extracurricular activities, watching television, using Internet and computer, and playing videogames causes a reduced sleep time. 10 A study among Chinese high school students showed that supplemental learning classes after school hours was one of the reasons for SLD. 11
A study by Owens et al 12 showed that consequences of insufficient sleep among adolescents range from inattentiveness, reduction in executive functioning, and poor academic performance to increased risk of obesity and cardiometabolic dysfunction, mood disturbances which include increased suicidal ideation, a higher risk of engaging in health risk behaviors such as alcohol and substance use, and increased rates of car crashes, occupational injuries, and sports-related injuries. 12
Singh et al 13 found that prevalence of SLD in adolescents in a school in Delhi increased with age, from 83.7% to 87.1% in 11 to 12 years to 90.5% to 92.5% in 13 to 15 years. Gupta et al 14 found that the mean total sleep time in adolescents in urban school-going adolescents in New Delhi was 7.8 h/day and that adolescents of higher grades had lesser total sleep time and more frequent nocturnal awakenings. Paiva et al 15 in a study, in Portugal among 3,476 adolescents, found that the SLD is 18.9% among adolescents. Nasim et al 16 in a study, in Saudi Arabia among 12,121 adolescents, found that the prevalence of SLD is 46% on weekdays and 33% on weekends.
It was thus important to study about the prevalence and causes of SLD among adolescents. Sleep patterns change depending on lifestyle and cultural factors. To the best of the author’s knowledge, there was no data published from Kerala about the prevalence of SLD and its associated factors in adolescents. Therefore, this study was conducted to know the prevalence of SLD and the factors that affect the sleep patterns of adolescents in an urban setting in Kerala.
Methods
This descriptive, cross-sectional study was conducted among 13 to 18 years old adolescents studying in 9th to 12th grades in schools of Thiruvananthapuram Corporation.
The sample size was calculated taking p (same proportion) as 18.9 (15) and was found to be 412. Three schools were selected from a list of all the schools under Thiruvananthapuram corporation using a random number table. From each school, around 140 participants were required. A list of all students separately for each grade 9th to 12th was obtained and 50 participants were selected using a random number table from each grade. The rationale of the study was explained to those participants and assent was taken from them. A parental consent form was given to them and the investigators decided to include all the participants who brought back signed consent forms in the study. We returned on another day and distributed self-administered structured questionnaires to students who brought signed consent forms. Each item of the questionnaire was explained and the participants were asked to clarify any doubts they had for any question before filling their responses. The weight and height of the participants were measured. After collecting the questionnaire, a class on good sleep habits was taken for the students.
The questionnaire was made available in English and the mother tongue (Malayalam). The questions in the proforma and the multiple response answers were prepared after brainstorming sessions with content experts. The sociodemographic variables collected were age, sex, place of residence (rural/urban) and grade. Height and weight were collected to calculate Body Mass Index (BMI). BMI was calculated as per BMI for age Indian Academy of Pediatrics (IAP) 2015 charts (obesity is above 27th adult equivalent line, overweight above 23rd adult equivalent line, thinness below 3rd percentile). 17 Data for all questions related to sleep were inquired separately for schooldays and weekends. Time of going to sleep and waking up were asked to calculate the total duration of sleep for assessing presence of SLD. Adolescents are considered to have SLD if they slept less than the required amount of hours (8-10 h, according to ASA).4, 5
Students were asked if they felt sleepy during the day and also whether they used to take nap in the evening after school and its duration. Night time awakenings and the reasons behind it were also asked. The questionnaire also collected data about when students left for school in the morning, and school start and finish times. Students were also inquired about the marks in the last exam, whether they were tensed about marks, if it affected sleep badly and their preferred study time (late night/early morning/nothing in particular). They were asked whether they go for tuitions and if they did, duration and time (morning/evening/both) of tuitions were also collected. Any type of screen time before bed and its duration was noted. Students were also asked about their parents’ sleep habits including when they go to sleep and whether the child slept “before” or “after” the parents.
The permission for this study was obtained from the Human Ethics Committee of our institution. Permissions were also obtained from respective school managements and Parent Teacher Association (PTA) officials.
The inclusion criteria was all students of grades 9th to 12th in the age group of 13 to 18 years. Students who did not fall into age group of 13 to 18 years, or did not want to take part in the study or those who had illnesses that affected sleep (like asthma, mental health issues, migraine, etc 12 ), or did not obtain parental consent were excluded from the study. An enquiry was done with those children who failed to fill the form completely and attempts were made to make them fill the forms satisfactorily. Even after such attempts, some students failed to completely fill up the forms and they were excluded from the study.
Statistical Analysis
Collected data from the questionnaires were entered into Excel sheets and analyzed using SPSS Version 22. All quantitative variables were expressed as mean and standard deviation and all qualitative variables were expressed as proportion. Prevalence was found with 95% confidence Intervals. Risk factors studied for the outcome were sociodemographic factors, BMI, preferred study time, tuition hours per week, before bed screen time, and parents’ time of going to sleep at night. These were selected based on previously conducted studies.6–11, 13, 14, 16 Odds ratio were calculated for each risk factor. Chi-square test was used as test of significance. Multivariate analysis was done by creating regression models using binary logistic regression.
Results
Out of the 426 students who took part in the study, 29 students were excluded (including 15 with medical illnesses affecting sleep). Among 397 students, 225 (56.7%) were males and 172 (43.3%) were females. Mean age was 15.79 years (SD 1.23).
A total of 225 students were males (56.7%), while 172 students were females (43.3%). A total of 295 students (74.3%) lived in urban locality, while 102 (25.7%) lived in rural locality (Table 1).
Baseline and Daily Routine Characteristics Related to Sleep.
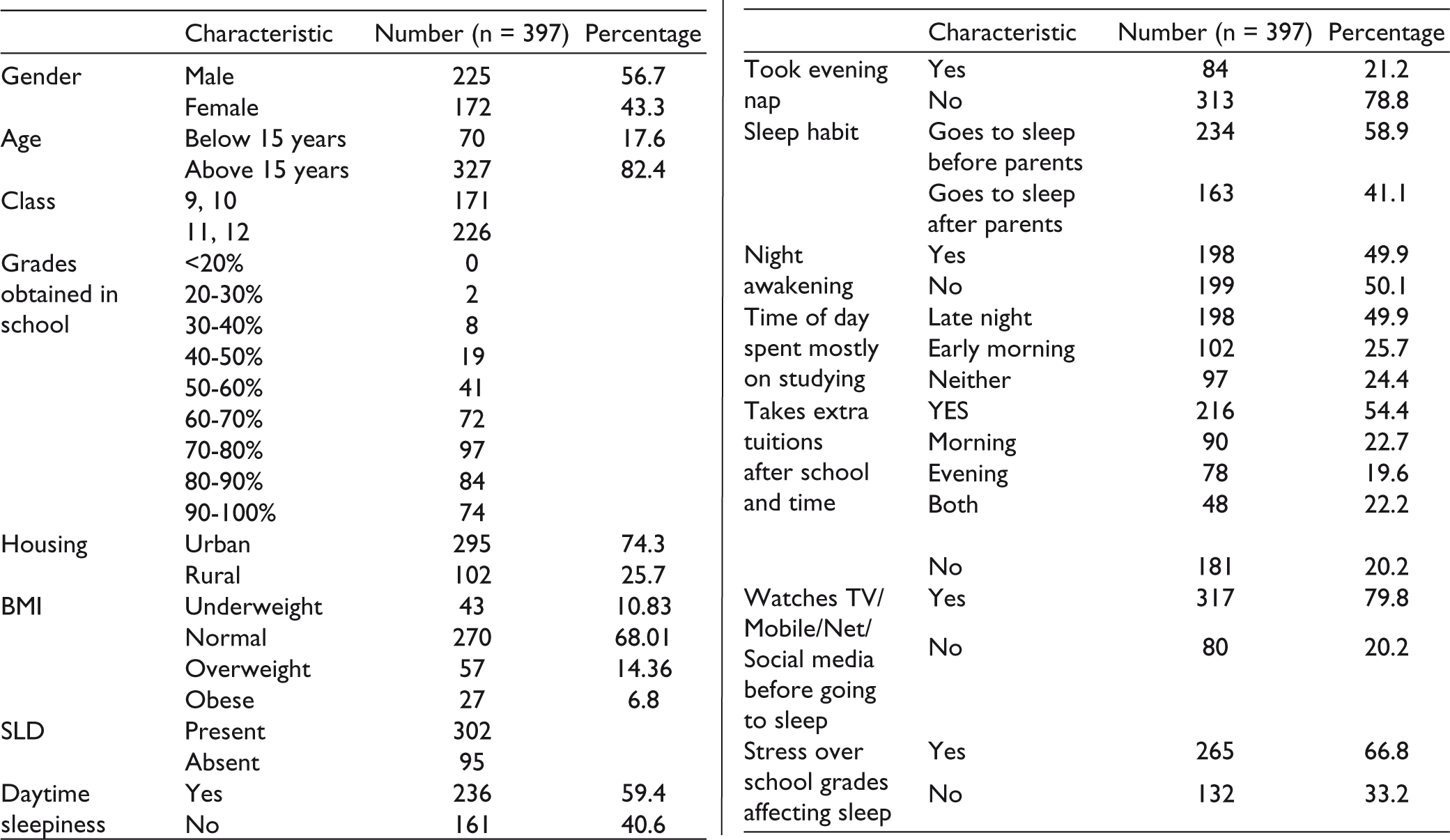
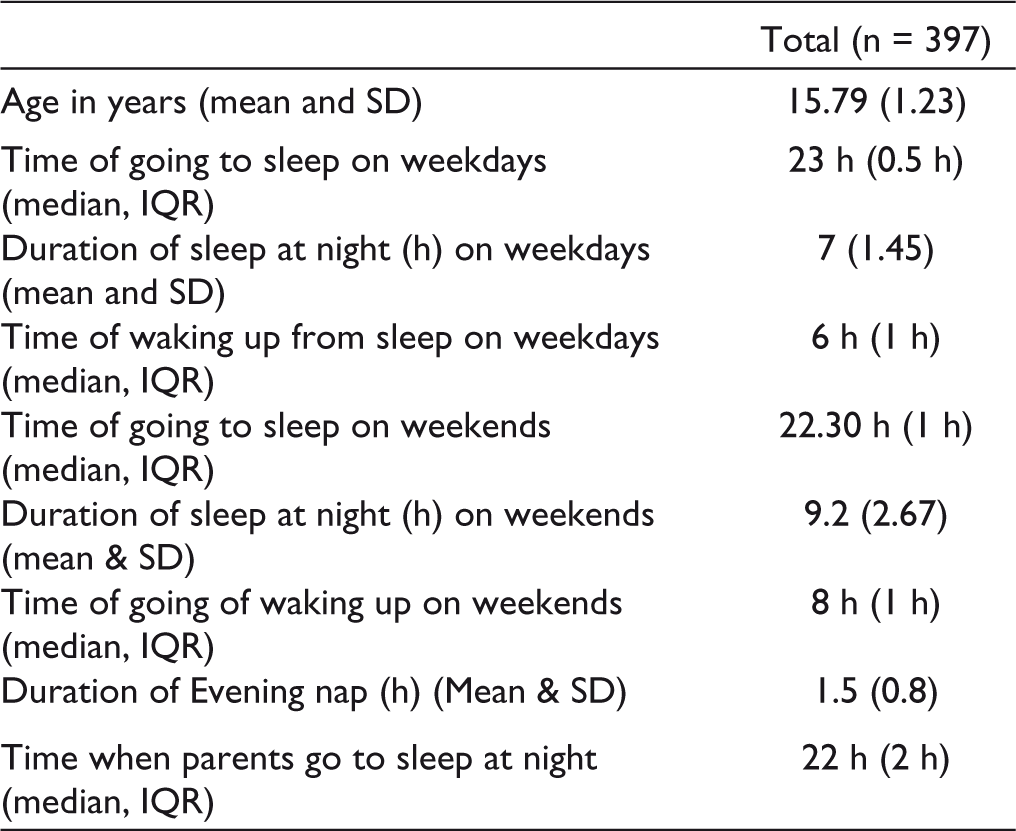
Mean duration of sleep on weekdays was 7 h (SD 1.45). A total of 302 students (76.07%) had SLD (Table 2).
Summary Statistics of Sleep Pattern of Study Subjects and Their Parents
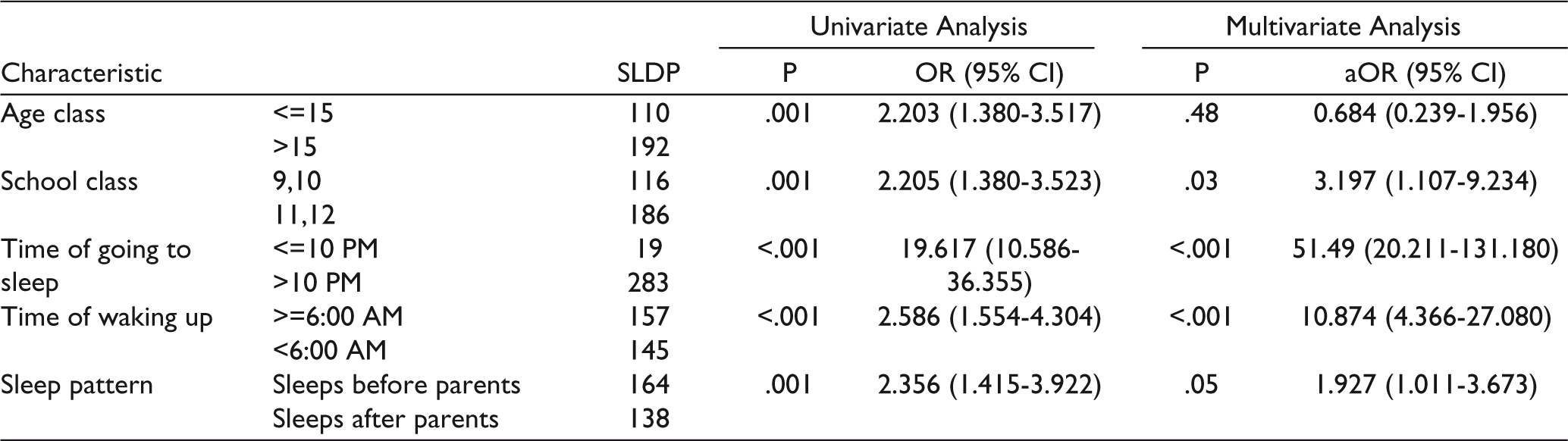
Univariate analysis was done. Compared to adolescents aged 15 years or below, those above 15 years had more risk of SLD (OR = 2.203, 95% CI: 1.380-3.517). Students of classes 11th and 12th had more risk of SLD than students of classes 9 and 10 (OR = 2.205, 95% CI: 1.380-3.523). Compared to students who go to sleep at 10 PM or earlier, those who go to sleep after 10 PM had more risk of SLD (OR = 19.617, 95% CI: 10.586-36.355). Those who wake up before 6 AM had more risk of SLD than those who wake at 6 AM or later (OR 2.586, 95% CI: 1.554-4.304). Compared to students who sleep before their parents, students who sleep after their parents had more risk of SLD (OR = 2.356, 95% CI: 1.415-3.922).
On multivariate analysis, age was found to be not significant. Students of 11th and 12th (adjusted OR [aOR] 3.197, 95% CI: 1.107-9.234), going to bed after 10 PM (aOR 51.49, 95% CI: 20.211-131.180), waking up before 6 AM (aOR 51.49, 95% CI: 20.211-131.180), and going to after parents (aOR 1.927, 95% CI: 1.011-3.673) were significant (Table 3).
Variables like sex, place of residence, BMI, tuition hours, and before bed screen time were not found to be significant.
Details of Univariate and Multivariate Analysis Showing Association Between Proposed Risk Factors and SLD
Discussion
The present study investigated the prevalence of SLD and also the risk factors for SLD among school-going adolescents in an urban setting in Thiruvananthapuram, Kerala.
The sample has a good representation with a total of 402 adolescents, from 3 schools in urban Thiruvananthapuram with around 56.7% male and 43.3% female students. The study results can be generalized to adolescents of classes 9 to 12 in the state of Kerala with higher academic expectations.
SLD prevalence among school-going adolescents in the urban setting of Thiruvananthapuram district was found to be 76.07% (302 out of 397 students). Higher secondary classes, going to sleep after 10 PM, waking up before 6 AM, and going to bed after parents were the factors associated with SLD found in this study.
Studies have shown that there is a biological delay in time of sleep onset in adolescence due to changes in processes involved in sleep regulation; the circadian system and homeostatic sleep-wake system. 8 But, the time for waking up remains constant due to school start timings not changing in high school, hence leading to occurrence of SLD.
Majority of school-going adolescents in Thiruvananthapuram were found to have SLD (76.07%). The prevalence of SLD among school-going adolescents in the urban setting of Thiruvananthapuram district (76.07%) is comparatively lesser than the prevalence in Delhi (90.5-92.5%), 13 but much higher than the prevalence of Portugal (18.9%) 15 and Saudi Arabia (46%). 16 Majority of schools in Delhi have early start times and previous studies, like by Carskadon et al 18 found that early school start times were associated with significant SLD and daytime sleepiness. Also, the study by Singh et al 13 took cut-off of 8.5 h of sleep for SLD, unlike 8 h considered in this study.
Students of higher grades had greater SLD as compared to students of lower grades. Similar observations were observed in a study conducted among Indian school students in Bahrain, adolescents of grade 12 obtained only 6.1 h of sleep as compared to grade 6 students who obtained 7.7 h of average sleep. As Indian adolescents enter into higher grade levels, they spend more time in project and assignment in addition to private tuitions. 1 There is a lot of pressure among students regarding their future careers and entrance coaching. This was also shown in our study with around 66.8% of students being tensed about their marks.
Age was significant in univariate analysis but was not significant on multivariate analysis. This could be due to the fact that class is a more important variable than age as academic burden increases with class.
In our study, 84.6% of adolescents who slept after their parents had significant SLD, whereas 72.6% who slept before their parents were found to have SLD. Adolescents are also entering a period in which they are striving for autonomy and want to make their own decision including when to go to sleep but studies suggest adolescents do better in terms of mood and fatigue levels if parents set their bed time and choose time which is realistic for the child’s needs. 19 When child sleeps before the parents do, parents could effectively monitor the sleep-wake cycle of the child.
This study did not find significance of before bed screen time with SLD, unlike the study in Portugal. 15 A probable reason could be that majority of students had access to mobile phones in the Kerala setting. There was no significance with sex in this study similar to the study conducted in Bahrain. 1 Increased BMI was not found as a risk factor for SLD in this study though previous studies have shown that obesity is a risk factor for obstructive sleep apnea in adolescents which can cause poor sleep. 12
With the rising competition and academic pressures for adolescents, it is very important to discuss about importance of good sleep. In our study, adolescents in an urban setting in Kerala got an average of 7 h of sleep on weekdays. In a study among South Korean adolescents, the average sleep duration was found to be only 4.9 h a day. The yearly suicide rate among South Korean adolescents is also relatively high (10.7 per 1,00,000) and researchers believe that chronic SLD has a role to play with this.6, 18 Studies have shown about links of SLD with mental health problems like depression, and so on. 12 Suicide rate among 15 to 19 years in Indian population according to World Health Organization is 10.4 per 1,00,000 (2019 data). 20 A study in 2004 in rural south India found the suicide rates in 10 to 19 year age group to be 148 per 1,00,000 among females and 58 among males. 21 Studies have shown a temporal relationship between sleep problems and completed suicides in adolescents. 22 So far, no study has been conducted to consider the relationship of sleep disturbances with adolescent suicides in India.
The limitation of the study is that the data is based on responses given by students through the questionnaire. Answers given by students might have been to please the investigators (social desirability bias).
According to our study, children who slept before 10 and woke up after 6 had less SLD. This time frame of 10 PM to 6 AM ensures that the adolescent gets the minimum 8 h of sleep daily.
The implication of this study is to raise awareness on the increased prevalence of SLD among adolescents and to take methods to reduce it. This can help reduce future health risks, mental health issues, and suicides. Even policy changes can be implemented. In America, various schools took measures to shift the school’s start time which helped students to catch one more hour of sleep every night. 19 In a 2010 study in Rhode Island, a 30 min delay in school start time was found to increase night sleep duration by 45 min and students reported having better mood and motivation. 23 Involvement of parents also in the process has also found to help improve sleep.24, 25
Footnotes
Acknowledgements
The authors would like to thank Indian Academy of Pediatrics for selecting this research to fund as part of their Undergraduate Research Award. Dr Arjun C, MBBS, House Surgeon, Government Medical College, Thiruvananthapuram for assisting in data collection and entry. Dr Arun B Nair, Associate Professor, Department of Psychiatry, Government Medical College, Thiruvananthapuram, and Dr Arya Rahul, Senior Resident, Department of Community Medicine, Government Medical College, Thiruvananthapuram for their guidance. The principals, teachers, and PTA officials of the schools involved for giving permission to conduct the study.
Author Contributions
GZ conceived the idea, designed the methodology, collected the data, interpreted the results, and prepared the manuscript. PS guided the conduct of the study, designed the methodology, analyzed the data, interpreted the results, and critically reviewed the manuscript. GSI collected the data, interpreted the results, and critically reviewed the manuscript. AR collected the data, interpreted the results, and critically reviewed the manuscript. MRS collected the data and critically reviewed the manuscript. All the authors approved the final version of manuscript and are accountable for all aspects related to the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from Human Ethics Committee, Medical College, Thiruvananthapuram on October 15, 2019. HEC No. 09/33/2019/MCT.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the “Indian Academy of Pediatrics Research Award (Grant) – Undergraduate category”.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.