
Abstract
Introduction:
Fear and uncertainty are the 2 ingredients of psychological challenges brought about by coronavirus (COVID-19). Fear and intolerance of uncertainty can affect decision-making. Because of the pandemic and owing to their phase of cognitive development, adolescents are more susceptible to such influence.
Objective:
To explore and understand the effects of COVID-19 on emotion and cognition by investigating the association between fear of COVID-19, intolerance for uncertainty, and decision-making in Indian adolescents.
Method:
The sample constituted 136 Indian adolescents aged 15 to 19 years. The sampling technique used was a nonprobability sampling technique called snowball sampling. The sample was collected through an online platform, ie, WhatsApp, Facebook, and most responses were received from Delhi, Sirsa (Haryana), and Chandigarh. The tools administered were the fear of COVID-19 scale (FCVS-19), the Intolerance of Uncertainty Scale (IUS-12), and the adolescent decision-making questionnaire (ADMQ). Correlational, regression, and mediational analyses were conducted to study the associations and interactions between the 3 study variables.
Results:
The sample consisted of 51.5% females and 48.5% males. The correlational analysis reported significant positive relationships between fear of COVID-19, intolerance of uncertainty, and maladaptive decision-making. Further, mediation analysis reported: (a) the intolerance of uncertainty mediates the relationship between fear of COVID-19 and maladaptive decision-making patterns and (b) fear of COVID-19 mediates the relationship between intolerance of uncertainty and maladaptive decision-making patterns.
Conclusion:
The findings indicated that emotions experienced by adolescents during the COVID-19 pandemic could have a negative and significant effect on their decision-making. Thus, it is necessary to mitigate these effects to ensure optimal development of their cognitive skills during calamities such as the COVID-19 pandemic.
Introduction
Adolescence is characterized by sensitivity to psychological and social transformation, making this age group highly vulnerable to the psychological adversities brought by the novel coronavirus pandemic (COVID-19). Such an impact has been extensively studied1–3 and an elevation in the prevalence of anxiety and depression has been reported. 4
Fear underlies this rise in anxiety and depression during COVID-19. Schimmenti et al 5 proposed the 4 horsemen of fear model to organize the fear experienced during the COVID-19 pandemic around 4 domains: (a) bodily feature, (b) interpersonal feature, (c) cognitive feature, and (d) behavioral feature. 5 There have been cases where high fear of COVID-19 had led to death by suicide as the individuals believed they had contracted the coronavirus infection, despite the evidence that they had not.6, 7
Fear has been accompanied by another key characteristic of the pandemic: uncertainty. A perpetual state of uncertainty can become a problem, as overtime, individuals find it “intolerable.” Intolerance of uncertainty (IU) is an “individual’s dispositional incapacity to endure the aversive response triggered by the perceived absence of the salient, key, or sufficient information, and sustained by the associated perception of uncertainty.”8, 9 Studies have found a direct and significant effect of IU on mental well-being in the context of the COVID-19 pandemic. 10 Additionally, an association between IU and later dimensions of health anxiety has been found. 11 Furthermore, it has been found that IU is positively related to distress, greater uncertainty perceptions about the outcome, and greater perceived severity of threat. 12
Uncertain situations are characterized by a lack of information which is an essential aspect of the decision-making process. This absence of information can induce fear as it leads to a perception of uncertain situation as dangerous and imminent. 9 This emotional state of fear usually impairs decision-making. 13 Psychologist Sudeep Bhatia talks about an irrational balancing of risk and reward during decision-making. 14 A decision is indicative of a potential mistake which is why under uncertainty, the risk level of an error is not evaluated by the brain.
DeSteno explains the psychology of coronavirus fear as a “mix of mis calibrated emotion and limited knowledge.” 15 Therefore, the interaction between fear, uncertainty, and decision-making relates very well with the COVID-19 pandemic. The impact of COVID-19 hampers cognitive development in children. 16 Fiorenzato et al, 17 in their study, reported the cognitive consequences of social restriction during the pandemic. The participants reported cognitive challenges such as attention, executive functioning, and temporal orientation. These challenges were majorly seen in the younger people. 17 Therefore, we argue that the critical psychological ingredients of COVID-19, namely fear and uncertainty, can have an undesirable effect on the developing cognitive skills of adolescents. This period is a “time of increased pressure for problem-solving and personal decision.” 18 By the age of 15, adolescents develop cognitive competency requited to make sound decisions, 19 however, with the ulterior motive to gain new experiences and try out new things, adolescents tend to engage in rather thrill-seeking. 20
The literature available on the psychological challenges during COVID-19 does not address the cognitive consequences in adolescents. Therefore, based on the literature reviewed from the international databases and upcoming areas to be explored (impact of COVID-19 adolescents’ cognition), this research aimed to examine the interaction of fear, uncertainty, and decision-making during the COVID-19 pandemic.
Hypotheses
H1: There would be a significant positive relationship between intolerance of uncertainty and fear of COVID-19 among Indian adolescents.
H2: High level of fear of COVID-19 would have a significant positive relationship with maladaptive decision-making patterns among Indian adolescents.
H3: Adolescents reporting a high level of intolerance of uncertainty would show maladaptive decision-making patterns among Indian adolescents.
H4: Intolerance of uncertainty would mediate the association between fear of COVID-19 and maladaptive decision-making patterns among Indian adolescents.
H5: Fear of COVID-19 would mediate the relationship between intolerance of uncertainty and maladaptive decision-making patterns among Indian adolescents.
Methodology
Participants
This study used a cross-sectional online survey and the nonprobability sampling technique called snowball sampling. The recruitment window lasted from January 25, 2021, to February 10, 2021. The sample comprised 136 Indian Adolescents aged 15 to 19 years. Because of the restrictions imposed by the lockdown and pandemic, the data were collected through Qualtrics, and the participants were contacted personally or through Facebook, WhatsApp, and Instagram. The design of the survey confined one device to one response only. The survey questionnaire was in English. Most of the responses were received from Delhi, Sirsa (Haryana), and Chandigarh. The data gathered were descriptive. Adolescents who met inclusion criteria voluntarily participated by clicking the study link. The participants could complete the survey using their personal computers/laptops, tablets, or smartphones.
Inclusion, Exclusion Criteria, and Ethical Considerations
Individuals belonging to the adolescent age group (15–19 years) (the age group criteria as defined by the World Health Organization). 21 This age group was considered for participation because adolescence is a milestone stage in the development of cognitive competencies.
Adolescents from all types of gender identities. No adolescents were excluded on the grounds of education, social-economic status, and geographical location.
Adolescents who reported mental health difficulties were excluded from the study. To assess this, participants were asked to self-report if they are currently seeking treatment or therapy from a mental health practitioner. Also, the participants who did not complete the survey were excluded.
The study was conducted per the ethical guidelines mandated by the American Psychological Association (APA) and as detailed in Helsinki’s declaration. Before collecting the data, written informed consent was taken from the participants.
Participants were also assured about the confidentiality of their responses.
Parental consent was not sought as the literature shows that by the age of 15, adolescents develop the cognitive competency required to make sound decisions, 19 the risk-taking behavior is only demonstrated in potentially harmful situations in order to gain new experiences and try out new things. 20 To that regard, this study did not involve any potential research harm. 22 Accordingly, the APA resolution waives parental consent in research with adolescents (that poses no potential harm). 23
The study was conducted as per the approved research protocol. The study has been approved by the institutional ethics committee of vide letter no. AIPS/ERC/RB2021/01.
Measures
Fear of Coronavirus Scale (FCV-19S) 24
FCV-19S is a 7-item, 5-point Likert scale developed by Ahorsu et al 24 to measure the severity of fear of COVID-19. The high overall scores on the scale are indicative of a more severe fear of COVID-19. The 7 items of the measure have satisfactory item-total correlation (0.47 to 0.56) and firm factor loadings (0.66 to 0.74). The scale also shows acceptable reliability values, namely internal consistency (α = 0.82) and test-retest reliability (ICC = 0.72). There is a positive correlation of the scale with perceived vulnerability, hospital anxiety, and depression. The scale has been successfully administered to the Indian population. The Tamil version of the scale reports a good internal consistency, making the tool valid and reliable for the Tamil-speaking population. 25 The English version of the scale has also been used to assess the fear of COVID-19 in the pan-India population. 26 The scale has been used with adolescent population across various nations and studies have concluded that the scale is fully invariant across gender and age.27–29
Intolerance for Uncertainty Scale (IUS-12) 30
IUS-12 was developed and validated by Carleton et al. 30 It assesses an individual’s propensity to find uncertain situations unpleasant. The items are rated on a 5-point Likert scale. The original scale consists of 27 items. There was a high correlation (r = 0.96) between the total score of the 12-item scale and the total score of the 27-item scale. Carleton et al found that the total score of IUS-12 maintained excellent internal consistency (α = 0.91). The scale has been used with adolescents to study risk-taking behavior. 31
Adolescent Decision-Making Questionnaire-Revised (ADMQ-R)
The ADMQ is a modification of the Flinders’ decision-making questionnaire by Mann (“Decision-making questionnaires I and II,” unpublished questionnaires, 1982). It is a 4-point rating scale. The 5 subscales of the questionnaire, namely, self-confidence, vigilance, panic, evasiveness, and complacency, are classified into “adaptive decision-making pattern” and “maladaptive decision-making pattern.” Each subscale has 6 items. The self-confidence and vigilance subscales represent an adaptive pattern of decision-making, while the other 3 subscales represent a maladaptive pattern of decision-making. The test-retest validity for the Hebrew version of the scale is 0.64. The internal consistency for the subscales is self-confidence (α = 0.76), vigilance (α = 0.70), panic (α = 0.70), evasiveness (α = 0.80), and complacency (α = 0.67).
Statistical Analyses
The statistical analyses of the study were done using IBM SPSS Statistics version 26 (IBM Corp., Armonk, N.Y., USA). Descriptive statistics were conducted for the variables of the study and the demographic characteristics of the sample. Pearson’s bivariate correlational analysis was conducted to examine the associations between the main study variables. To establish direct and significant cause and effect relationships between the variables, regression analyses were also run. Lastly, mediation analysis was conducted using PROCESS macro (version 3.5.3) for SPSS developed by Hayes to examine: (a) the mediating role of IU in the relationship between fear of COVID-19 and maladaptive decision-making and (b) the mediating role of fear of COVID-19 in the relationship between IU and maladaptive decision-making. The statistical significance of the mediating variable was investigated using 5000 bootstrapping samples.
Results
Demographic Profile
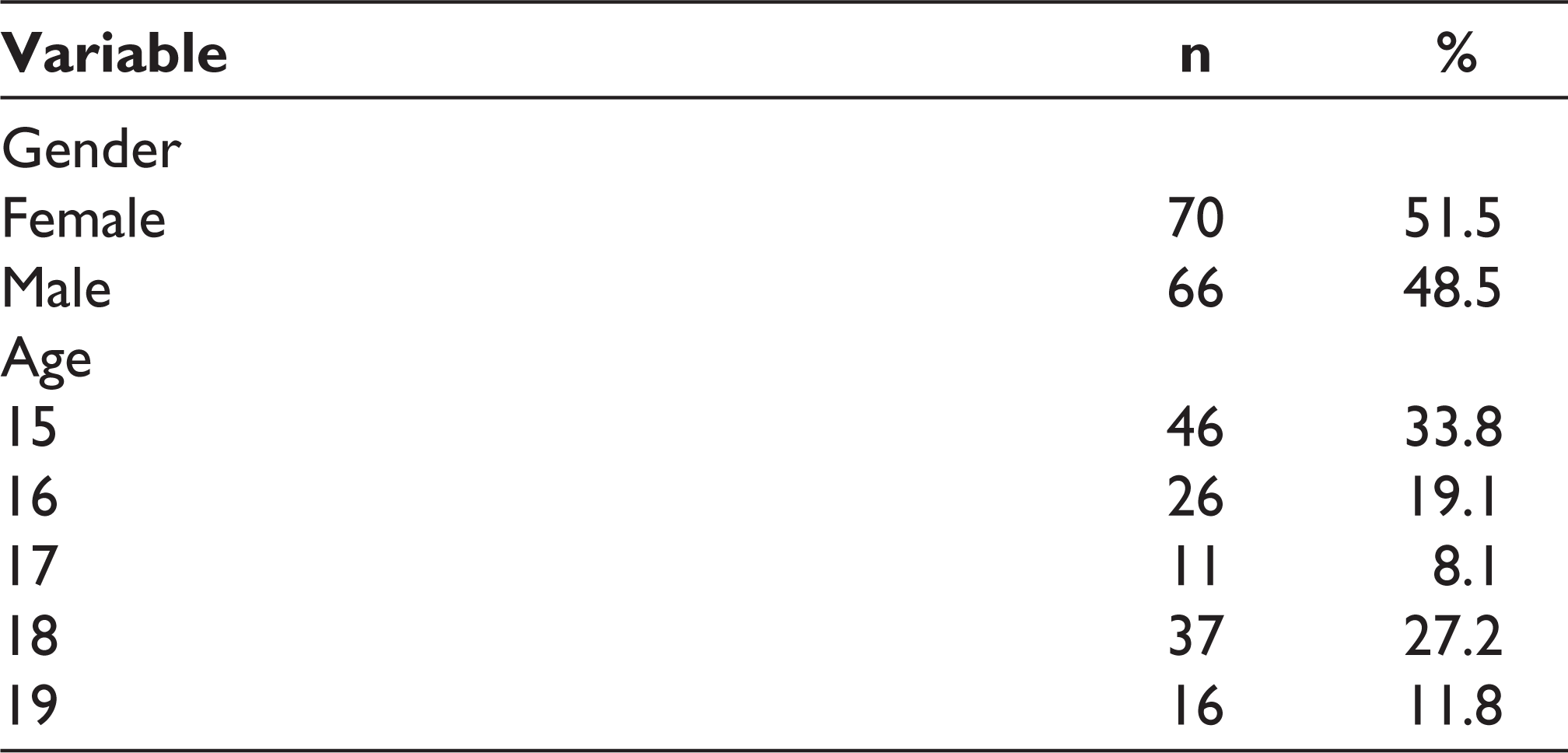
Of the 147 participants of the survey, 136 responses were included and 12 responses were excluded. The final sample characteristics (n = 136) are collated in Table 1. The mean age of the participants was 16.64 (SD = 1.47). Although the responses reviewed were from various Indian regions, the distributions were majorly concentrated in Sirsa (Haryana), Delhi, and Chandigarh.
Sample Characteristics (n = 136)
The descriptive statistics for the main study variables are displayed in Table 2. The mean scores of fear of COVID-19 and IU were 17.44 (SD = 6.31) and 32.57 (SD = 9.47), respectively. For decision-making, only the scores of maladaptive decision-making patterns were considered for this study. The mean score for maladaptive decision-making patterns was 39.60 (SD = 9.16).
Descriptive Statistics Among the Study Variables (N = 136)
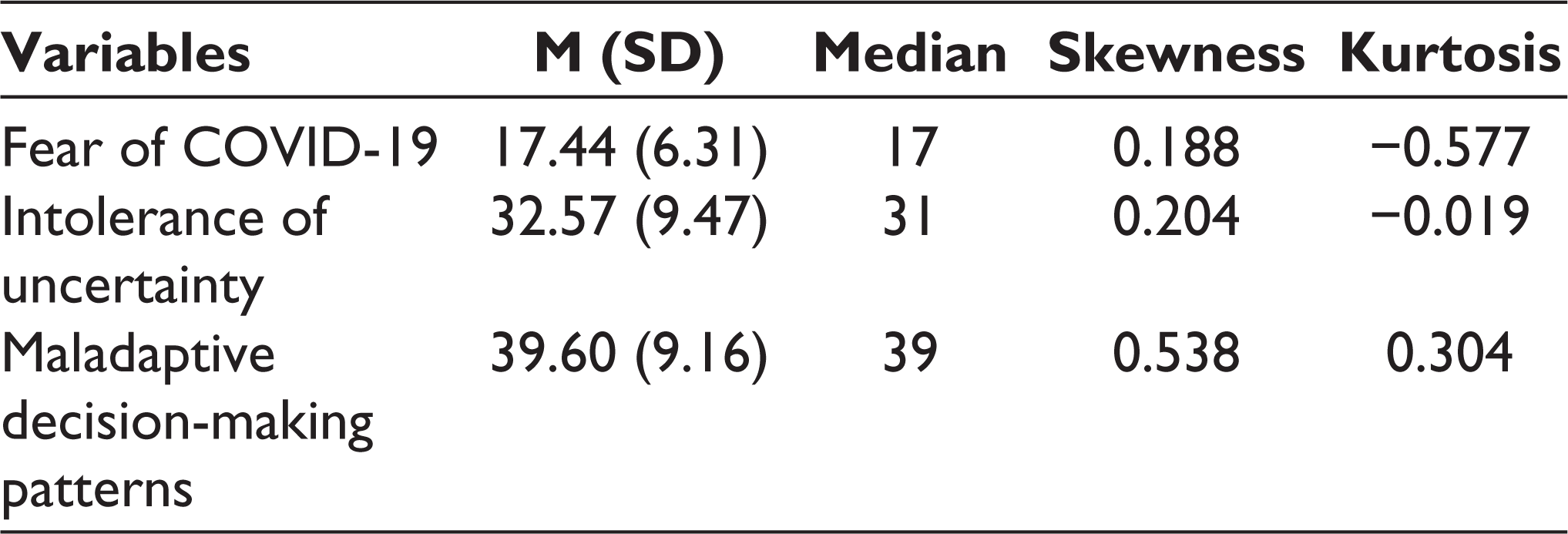
The normality of the data was considered through skewness and kurtosis statistics. The results indicated that the skewness of the data ranged from 0.19 to 0.54, and kurtosis ranged from −0.02 to 0.30. The skewness of the data shows an approximately symmetric distribution of variables. However, the kurtosis of the data shows a mixed result as scores of fear of COVID-19 and intolerance of uncertainty indicate an excessively flat distribution. In contrast, the scores of maladaptive decision-making patterns are nearly somewhat peaked. All in all, it can be concluded that the current data deviate from a normal distribution.
Association Between the Variables
Table 3 shows significant positive relationships between all the study variables. Confirming hypothesis 1, there was a significant positive relationship between intolerance of uncertainty and fear of COVID-19. Hypothesis 2 was confirmed as fear of COVID-19 and maladaptive decision-making patterns were significantly and positively related. A significant positive relationship was found between intolerance of uncertainty and maladaptive decision-making patterns, thus confirming hypothesis 3.
Pearson’s Correlations Between the Main Study Variables (N = 136)
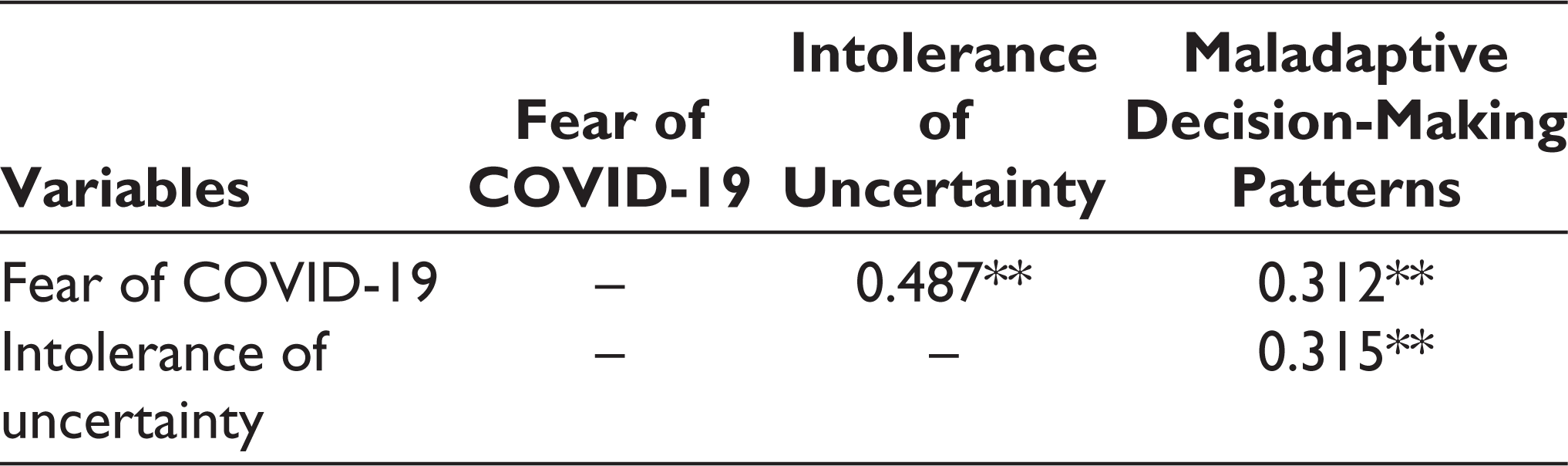
Table 4 presents the findings from the simple regression analyses on fear of COVID-19 as a dependent variable and IU as the independent variable. Findings revealed that IU was a significant predictor of fear of COVID-19 with an R 2 value of 0.237. This indicated that with a significant regression on fear of COVID-19 (F (1, 134) = 41.710, P < .001), IU influenced 23.7% of the scores of fear of COVID-19. It can thus be concluded that as IU increased, fear of COVID-19 also increased significantly.
Linear Regression with Fear of COVID-19 as the Dependent Variable

Table 5 presents the findings from the simple regression analyses on IU as a dependent variable and fear of COVID-19 as the independent variable. Findings revealed that fear of COVID-19 was a significant predictor of IU with an R 2 value of 0.237. This indicated that with a significant regression on IU (F (1, 134) = 41.710, P < .001), fear of COVID-19 influenced 23.7% of the scores of fear of COVID-19. It can thus be concluded that as the fear of COVID-19 increased, IU also increased significantly. Based on the findings in Tables 4 and 5, fear of COVID-19 and IU share a bi-directional relationship and exert an equal amount of influence on one another.
Linear Regression with Intolerance of Uncertainty as to the Dependent Variable

Regression of maladaptive decision-making patterns as dependent variable and intolerance of uncertainty and fear of COVID-19 as independent variables is presented in Table 6. IU was a significant predictor of maladaptive decision-making patterns (F (1, 134) = 14.717, P < .001). However, it explained only 9.9% of the variance in the scores of maladaptive decision-making patterns. Similarly, as a significant predictor of maladaptive decision-making, fear of COVID-19 (F (1, 134) = 14.717, P < .001) influenced 9.7% of the scores of maladaptive decision-making patterns.
Linear Regressions with Maladaptive Decision-Making Pattern as a Dependent Variable
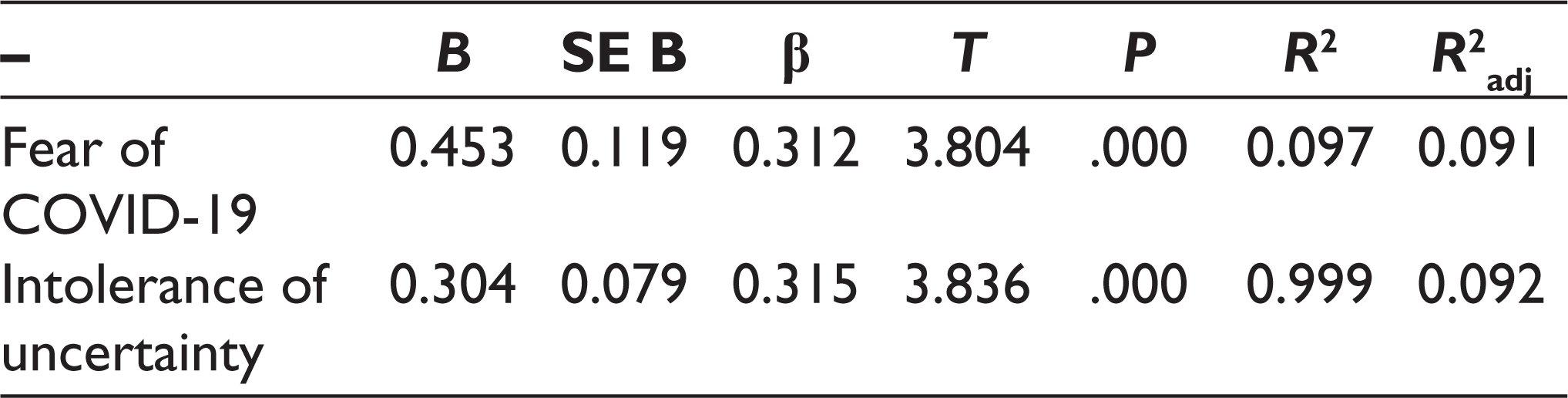
Figure 1 demonstrates the mediational analyses model that examined the influence of IU on maladaptive decision-making patterns, as mediated by the fear of COVID-19. The model shows significant mediation by fear of COVID-19 on IU’s influence on maladaptive decision-making [b = 0.098, 95% BCa CI [0.010, 0.206]. The Preacher and Kelly’s Kappa Squared was 9.3% (k 2 = .093), indicating a low effect size. The significant partial and complete standardized indirect effect of IU on maladaptive decision-making patterns via FCV were found to be b = 0.010, 95% BCa CI [0.001, 0.021] and b = 0.101, 95% BCa CI [0.010, 0.206], respectively.
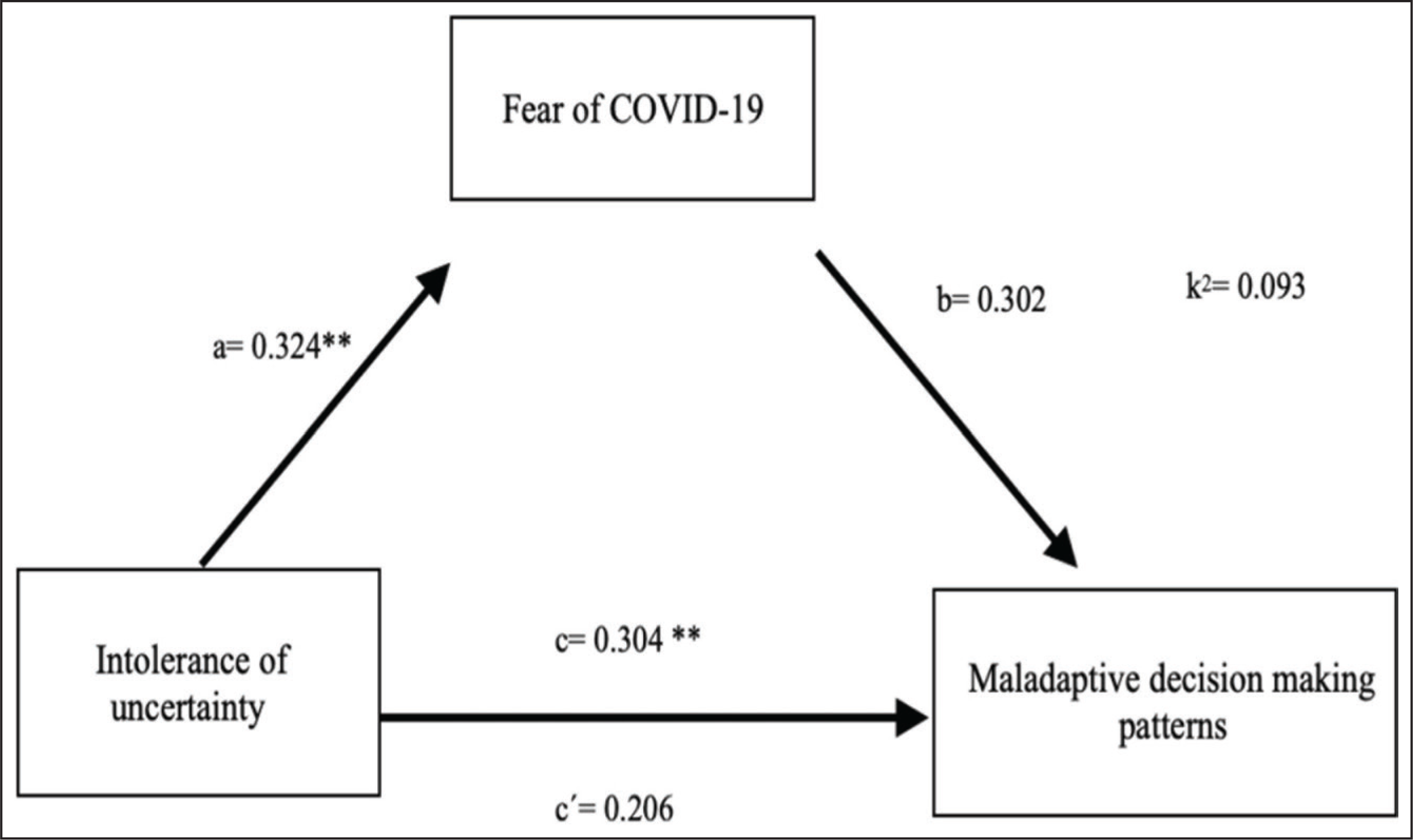
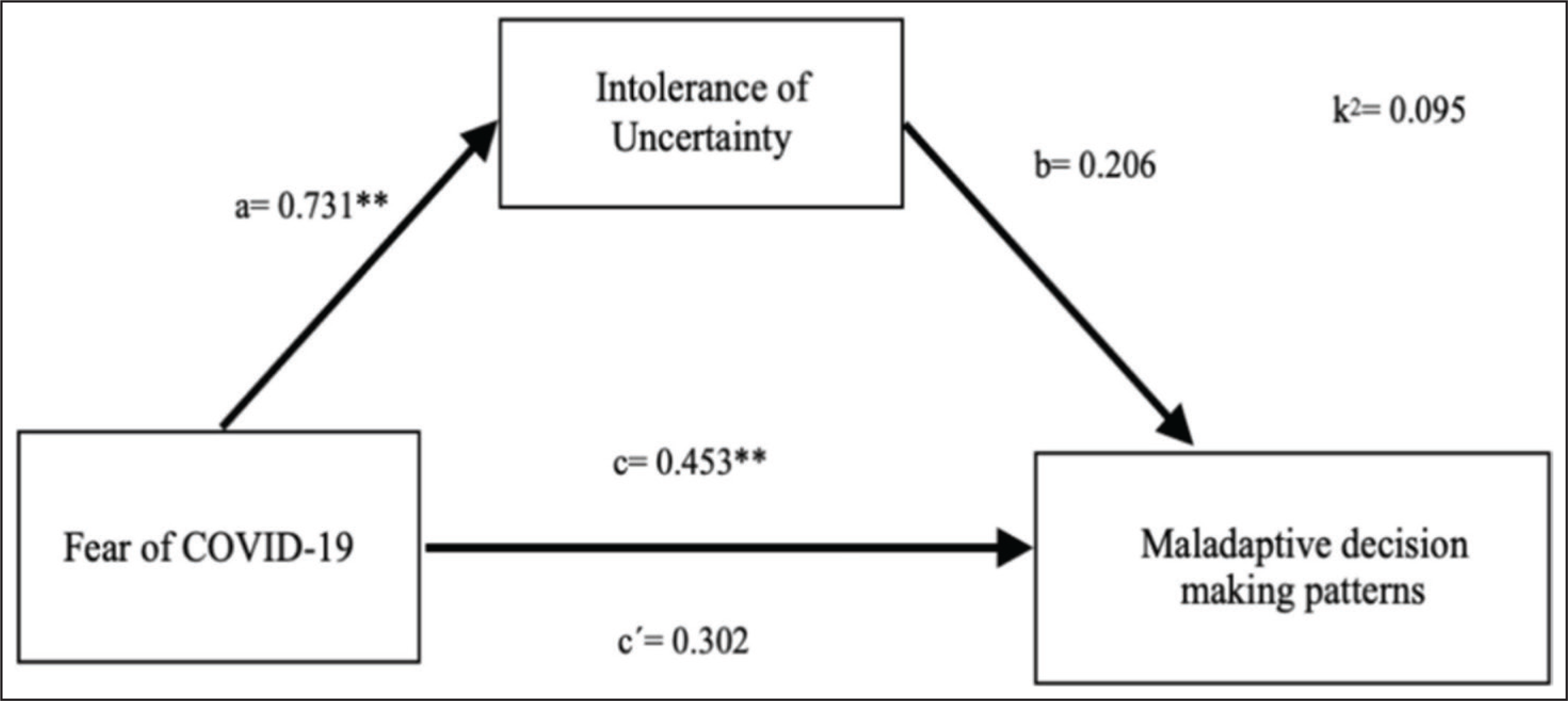
Figure 2 represents the influence of fear of COVID-19 on maladaptive decision-making patterns, as mediated by IU. It was found that IU significantly mediates the effect of FCV on maladaptive decision-making patterns, b = 0.150, 95% BCa CI [0.004, 0.316]. The Preacher and Kelly’s Kappa Squared was 9.5% (k2 = .095), indicating a low effect size. The significant partial and complete standardized indirect effect of FCV on maladaptive decision-making patterns via IU were found to be b = 0.016, 95% BCa CI [0.0005, 0.033] and b = 0.103, 95% BCa CI [0.002, 0.215], respectively.
In sum, it can be concluded that the fear of COVID-19 and IU mediate each other’s indirect influence on maladaptive decision-making patterns.
Discussion
Adolescence is characterized by increased sensitivity to social and psychological changes. The literature reveals an elevation in the prevalence of anxiety and depression in adolescents during the COVID-19 pandemic. Furthermore, studies have highlighted the negative impact of the pandemic on cognitive development in children. 16 Additionally, comparative studies have reported cognitive worsening in younger age groups as opposed to the older, during the pandemic. 17
Studies have also linked cognitive difficulties to increased psychological symptoms such as depression and anxiety.32, 33 The influential role of IU in anxiety has also been established.34, 35 Based on these findings, this study explored if fear and IU (characteristics of anxiety) can influence decision-making. Our results concluded that emotion, ie, fear of COVID-19, and cognitive constructs, ie, maladaptive decision-making patterns and intolerance of uncertainty, share a significant positive relationship.
The bi-directional relationship between fear of COVID-19 and IU is supported by the existing literature. For instance, IU mediates the relation between fear of COVID-19 and positivity, 36 and fear of COVID-19 mediates IU’s relationship with mental well-being 10 and depression. 37 The underlying mechanism of this relationship is the over-activation of alerting network of attention brought about by the IU.
Furthermore, the study also found more maladaptive decision-making patterns in those who reported high fear of COVID-19. While there is a paucity of research regarding this relationship, evidence exists for the influence of fear on the risk assessment. This has been mainly explained by the extension of Kahneman’s Thinking, fast and slow (2011) dual-process decision-making models that examine the impact of fear on one’s assessment of risk within this dual-process model. As fear takes over individuals, it regulates the perceived sense of control and self-esteem. This contributes to one’s perception about regulating the cause and effect or action and result. Thus, fear affects decision-making by inundating one’s sense of agency and sense of identity. 38 Highly intolerant adolescents (toward uncertainty) displayed maladaptive decision-making patterns, ie, panic, evasiveness, and complacency. IU is associated with the tendency to select the immediately available but less valuable and less probable rewards and sensitivity to outcomes. 39 It has been linked to several anxiety disorders, and anxiety felt in the face of uncertainty may result in maladaptive behaviors such as impulsive decision-making. 40 The association between intolerance to uncertainty and self-reported maladaptive behavior can be explained by uncertainty paralysis, which refers to one’s tendency to freeze during uncertainty. 41 Future research can examine the role of such uncertainty paralysis as an underlying mechanism that regulates the relationship between uncertainty intolerance and adolescents’ maladaptive decision-making patterns.
Fear makes us cognizant of the precautions and meticulous details before reaching a final decision. But the same fear can diverge us from rational thoughts when we are presented with uncertain situations. This argument provides the fundamental mechanism for accepted mediation models of this study, which indicate that: (a) fear of COVID-19 mediates the relationship between IU and maladaptive decision-making and (b) IU mediates the relationship between fear of COVID-19 and maladaptive. Falling in line with these results, Hunt et al 42 found that anxiety sensitivity and intolerance of uncertainty facilitate the relationship between maladaptive avoidance decisions and fear. Studies have also shown that fear guides decision-making during uncertain situations, as demonstrated in a study of traumatic brain injury (TBI) patients, which concluded that impaired decision-making and risk behavior after TBI could be preceded by deficits in the processing of fear. 43
The findings of the study call for the development of interventions that mitigate the risk factors associated with the interaction of emotions (fear of COVID-19) and cognitive constructs (intolerance of uncertainty and decision-making). By risk factors, we refer to cognitive challenges (such as indecisiveness, lower self-efficacy, etc) later in life, which can be manifested in job insecurity, unemployment, unhealthy relationships, impaired immunity, and psychiatric symptoms.
Limitations and Implications of Future Research
Although the available literature has corroborated findings, there remains a lack of literature that examines the exact relationship between variables in adolescents. Therefore, this exploratory research addressed this knowledge gap. Nevertheless, the study displays certain limitations which can be addressed in future research. First, the study design can be studied on a larger sample to create a possibility of larger effect sizes. Second, the study did not examine a potentially associated factor of exposure risk, ie, differences in results of those residing in the high-risk zone compared to those residing in low-risk zone. Third, this study did not address the temporal aspect of the variable; thus, advising more longitudinal research. Fourth, the study was correlational and used self-report measures. Moreover, the applicability of all the chosen measures in the Indian adolescent population is not yet established. Future research can administer behavioral assessment tools to investigate the concerned associations.
Future research on similar grounds can consider gender differences in the level of intolerance of uncertainty and fear. Moreover, the analysis can be conducted on adults to generalize the findings to a larger population and pave the way for refined emotion–cognition theories. Given that the autonomic responses precede decision-making, this study’s design can be modified to an experimental task-based paradigm to explore the underlying physiological mechanism. The study also recommends a longitudinal approach to examine the temporal effects of these variables. Furthermore, a psychoeducational component can also be extracted to upskill children and adolescents about the relationship between their emotions and cognitive constructs.
Footnotes
Acknowledgements
We would like to express our gratitude to all those who have helped us put together this research work. We wish to thank, first and foremost, Dr Ranjana Bhatia, Head of the Institution, Amity Institute of Psychology and Allied Sciences, Amity University, for her support in the accomplishment of this study. We are highly indebted to her for giving us intellectual freedom in our work. We would also like to extend our gratitude to Dr Neelam Pandey, who has always been a source of inspiration. Her continuous encouragement and guiding force behind this work made it possible for us to undertake this research. Our heartfelt gratitude also extends to all those who took out time to participate in this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.