
Abstract
Background:
Obesity is a growing health problem across the globe. Obesity and psychological well-being have been explored in the Indian adolescent and adult population. However, their association has not been explored in Indian obese school children.
Aims:
The primary objective of this study is, therefore, to analyze body image dissatisfaction (BID), depression, and health-related quality of life (HRQOL) in obese and normal-weight children and to compare these factors between the 2 groups.
Methods:
In this cross-sectional study, 100 obese and 100 normal-weight children from Mumbai, between 10 and 12 years of age were recruited by simple random technique. The BID was assessed using Stunkard’s Silhouette Figure Rating Scale. Depressive symptoms were evaluated with the Mood and Feelings Questionnaire: Short Version and HRQOL was examined using the Pediatric Quality of Life Inventory. The statistical analysis was carried out using SPSS statistical software version 24 (SPSS Inc. Chicago, IL USA).
Results:
The mean body mass index of the normal-weight children was 15.76 ± 1.4 kg/m 2 and 26.62 ± 3.1 kg/m 2 for obese. All obese children demonstrated BID, 54% were depressed and only 33% demonstrated a very good HRQOL. Intergroup analysis revealed a statistically significant difference in the obese group for BID, depression, and HRQOL, where P < .05.
Conclusion:
Obese school children are more prone to BID, higher depressive symptoms, and poor HRQOL than normal-weight school children. Thus, it demands a multimodal approach in preventing chronic psychological related problems in obese children.
Introduction
Obesity does not only act as a precursor for noncommunicable diseases but also affects psychological well-being. It is becoming a growing health problem across the globe. 1 According to the World Health Organization (WHO), majority of the overweight and obese children are housed in developing countries. Obesity Collaborators revealed that India has the second-highest number of obese children (14.4 million) in the world. Its prevalence varies from 5% to 19.3%.2–4
Apart from the identified contributing factors such as poor dietary habits and a sedentary lifestyle, family factors such as types of food available at home and the food preferences of family members are also found to increase the risk for developing childhood obesity. 5 Consequences of childhood obesity are found to manifest into psychosocial problems including distorted peer relationships, poor self-esteem, body image dissatisfaction (BID), and depressive symptoms which eventually affect the quality of life.6–8 A study by Arumuganathan et al in 2021 identified that psychiatric illness and body shape dissatisfaction are very common among adolescent obese children in India. 9
The National Eating Disorders Collaboration defined body image as a person’s perception of their physical self and the thoughts and feelings–positive, negative, or both–which result from that perception. 10 It includes how a person sees themselves, as compared to the normal weight that has been set by society. Sánchez et al 11 and Deshmukh and Kulkarni 12 among others have found an association between the BID and body mass index (BMI) in their research investigations.11, 12 Deshmukh and Kulkarni 12 further stated that Indian adolescents with higher body mass index and underweight were dissatisfied and unhappy about their body shape. Multiple studies across various regions have reported that psychological abnormalities such as eating disorders, poor self-esteem, and depression are closely associated with obese children with BID.13–15 The WHO states that childhood obesity and depression related to it may become a serious health condition leading to poor functioning of the child at work, school, and the family. 16 Likewise, childhood obesity profoundly affects health-related quality of life (HRQOL) either directly or inversely.5, 8, 17, 18 Sarwer and Polonsky in their study have identified the depth of the psychological burden on individuals with obesity. They found that BID is directly related to the excess weight gained by an individual affecting the quality of life and leading to depression. 19 Numerous other studies have also determined that obesity and BID associated with it negatively influence the HRQOL.20–22
Yazdani et al in their study also showed that obesity causes negative body image perceptions which in turn affects psychological well-being. They emphasize that clinicians must include mental health treatment strategies as well while addressing such patients. 23 Similarly, Weinberger et al 24 also concluded that interventions used to manage BID can be beneficial to achieving psychological well-being as well as weight management. 24 Moving further, Luppino et al with their meta-analysis confirmed the presence of a direct relationship between obesity and the risk of depression. 25
Global evidence suggests that there is a relationship between BID, depressive symptoms, and HRQOL. India houses many obese children but studies till date have explored only the adolescent and adult obese population. There is a paucity of literature linking psychological comorbidities and childhood obesity in India. Although many concerns are raised with respect to childhood obesity, the relationship between these factors has not been firmly established. Thus, our study is an attempt to answer the research question–Is there an association between BID, depression, and HRQOL among obese children? The primary objective of this study is, therefore, to analyze BID, depression, and HRQOL in obese and normal-weight children and to compare these factors between the 2 groups.
Methods
It is a school-based cross-sectional study, carried out from September 2019 to January 2020. All the English medium schools in the city of Mumbai were enlisted. Based on the convenience sampling technique, 2 schools were selected from the eastern suburbs of Mumbai suburban district, the Konkan division of Maharashtra. The research approach was explained before the data collection and permission was taken from the concerned school authorities, physical education teachers, and the class teachers. The Institutional research review committee approved this study. Normal-weighted and obese school children between 10 and 12 years of age of both genders were included. Children with listening difficulty, acute medical conditions, recent hospitalization in the past 6 months, physical disabilities, and prediagnosed psychiatric problems were excluded from this study.
The sample size was calculated by using OpenEpi online software, version 3.01. Considering 67% of prevalence of BID in obese children, 26 at 95% CI (1−α), power as 80%, ratio of controls to cases as 1, the proportion of controls with exposure as 45, and proportion of cases with exposure as 67, the total required sample was 176. Considering a 10% dropout rate, the sample size was rounded off to 100 each in the obese group and the control group (normal weight).
Out of 2041 students, who enrolled in fifth, sixth, and seventh grade in the 2019 to 2020 academic year, 284 overweight students, based on their school physical record, were screened. The age of the participants was confirmed from the school records. All the participants were informed about the purpose, methodology, and benefits of the study. The participant information sheet and the informed consent form for parents/guardians were circulated to all the participants 2 weeks before the data collection. Informed consent from parents and the participants was obtained.
Out of 136 obese children, who fulfilled the inclusion and exclusion criteria, 100 were recruited based on a simple random sampling technique by computer-generated random number (graphpad.com) and assigned to the obese group. Similarly, 100 normal-weighted children selected to the control group for comparison. Anthropometric measures were taken in the same education center during the physical education period with the assistance of a physical education teacher. With the help of the class teacher, a maximum of 20 students were allowed to fill up the questionnaire in their respective classrooms. Students were under constant supervision of the investigator. Help was sought from schoolteachers to minimize the scope for discussion amongst them. All the participants were briefed and instructed in English to answer each item. The participants’ doubts were clarified by the investigator.
Measures
An anthropometric evaluation was carried out with standardized equipment and the guidelines of the National Health and Nutrition Examination Survey. 27 Height was measured by using a stadiometer and body weight by using a calibrated digital weighing scale. The participants were asked to remove their shoes, empty their pockets, and advised to wear single-layer clothing during the measurement day. BMI was calculated by dividing body mass by the square of the body height and expressed in kg/m 2 . Children were classified as obese and normal-weight according to revised growth charts by the Indian Academy of Pediatrics (IAP). 28 For boys, a BMI between the 5th to 71st percentile is considered normal, 71st to 90th percentile is overweight, and more than 90th percentile is obese. However, for girls, the range between fifth to 75th percentile is normal, 75th to 95th percentile is overweight, and more than 95th percentile is obese.
Participants’ BID was analyzed by Stunkard’s Silhouettes Figure Rating Scale and found to be reliable (r = 0.79) and valid. 29 It shows a series of 9 figure drawings for men and women, ordered from very thin to very obese. It involves 3 measurements: current image, desired image, and the discrepancy. For the first measurement, participants were asked to choose one image that is closest to their body image. For the second measurement, participants were asked to choose another diagram that will resemble their ideal or desired figure to be. The discrepancy is calculated by the difference between desired and perceived body image (ie, discrepancy = desired − current body image). When the discrepancy is equal to 0, a participant is satisfied with his/her body image; a positive discrepancy value indicates a desire to be bigger and a negative discrepancy for thinner. The discrepancy value used for the analysis was interpreted as the level of dissatisfaction with the body image.
For the analysis of depression, the “Mood and Feelings Questionnaire” Short Version (SMFQ) was adopted. It is a child self-report that is reliable and valid for children and adolescents. 30 Internal reliability is high (Cronbach’s α = 0.85), with 60% sensitivity and 85% specificity with a cut-off score of 8 or more. It consists of 13 questions with 3-point Likert scale: “not true” (0), “sometimes” (1), and “true” (2). All the participants were asked to mark their answers to each question. Each response summed to form a total score out of a maximum possible score of 26. A higher score indicates more depressive symptomatology. An established clinical cut-off of 8 indicated the likely presence of depression.
The quality of life was assessed by the Pediatric Quality of Life Inventory (PedsQL) 4.0. It is reliable for the total scale score (α = 0.89 child; 0.92 parent report) and validated for measuring HRQOL in children and adolescents and is applicable in clinical trials, research, clinical practice, school health settings, and community populations. 31 It consists of a total of 23 questions on physical function, emotional function, social function, and school function. The participant’s responses were recorded on a 5-point Likert scale from 0 (never), 1 (almost never), 2 (sometimes), 3 (often), and 4 (almost always). For scoring, items scored reversely and linearly transformed to a 0 to 100 scale as follows: 0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0. Total scores were obtained by the sum of all the items over the number of items answered on all the scales and transformed on a scale from 0 to 100. The mean score was estimated for each domain by dividing the sum of the items over the number of items answered only for that particular domain. Higher scores indicated better HRQL.
Statistical Analysis
The statistical analysis was carried out using SPSS statistical software version 24 (SPSS Inc. Chicago, IL, USA). The demographic characteristics, anthropometric values, SMFQ score, and PedsQL 4.0 scores were summarized using means and standard deviations. The normality of the data were checked using the Shapiro–Wilk test. As data were freely distributed, a Wilcoxon signed-rank test was performed for obese children’s gender influence on BMI, BID, SMFQ, and PedsQL. However, a Mann–Whitney U-test was performed to compare normal-weight and obese school children. Statistical significance was set at P ˂ .05.
Results
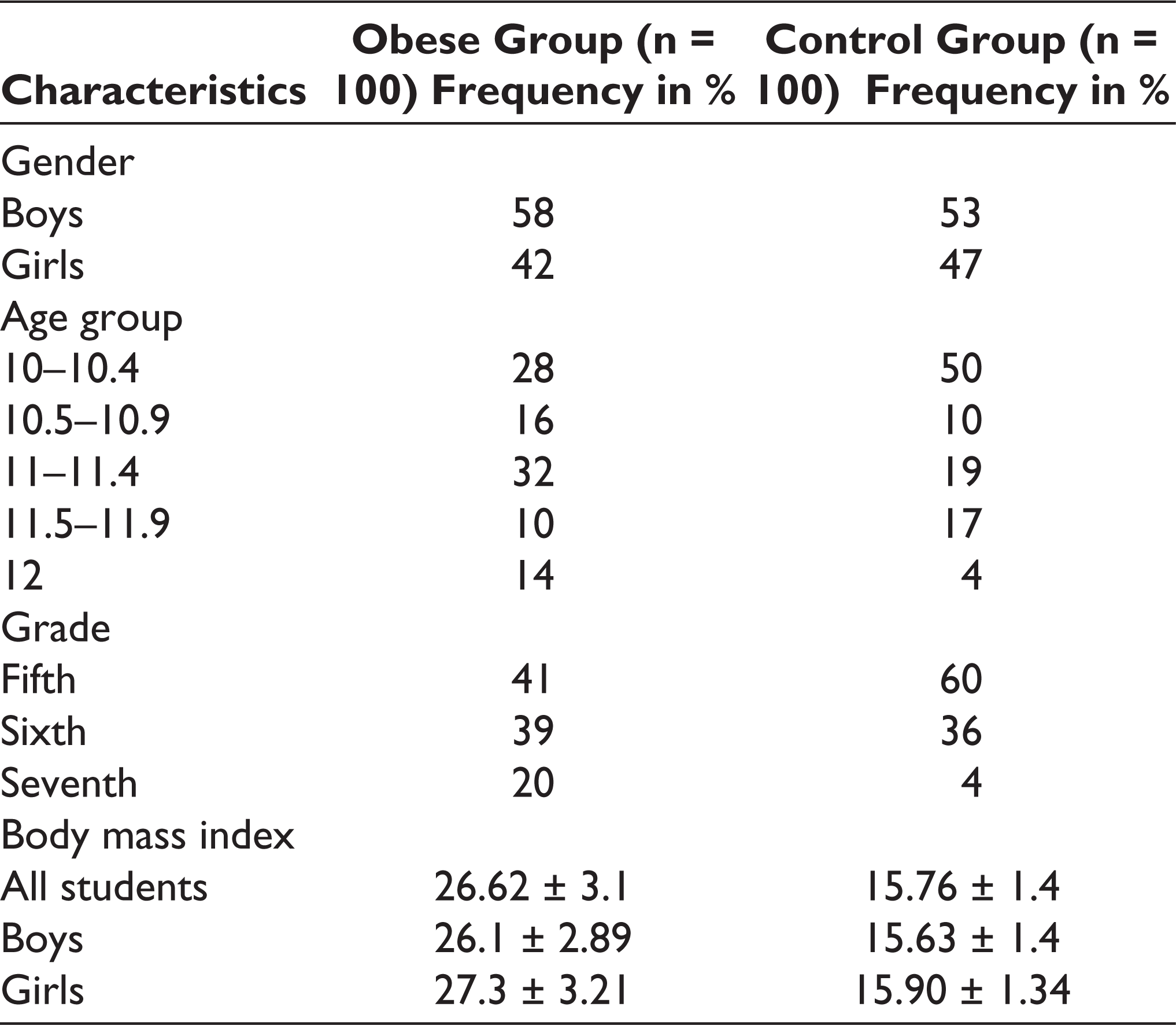
Overall, data of 100 normal-weight children and 100 obese school children were analyzed in this study. The participant recruitment strategy is depicted in the flow diagram shown in Figure 1. The mean age of the control group was 10.58 ± 0.6 years and that of the obese group was 10.8 ± 0.7 years. Their calculated mean BMI was 15.76 ± 1.4 kg/m 2 and 26.62 ± 3.1 kg/m 2 , respectively. The other demographic details of the participants are shown in Table 1.
Demographic Characteristics of Obese and Control Groups
Flowchart Depicting Participant Recruitment Strategy
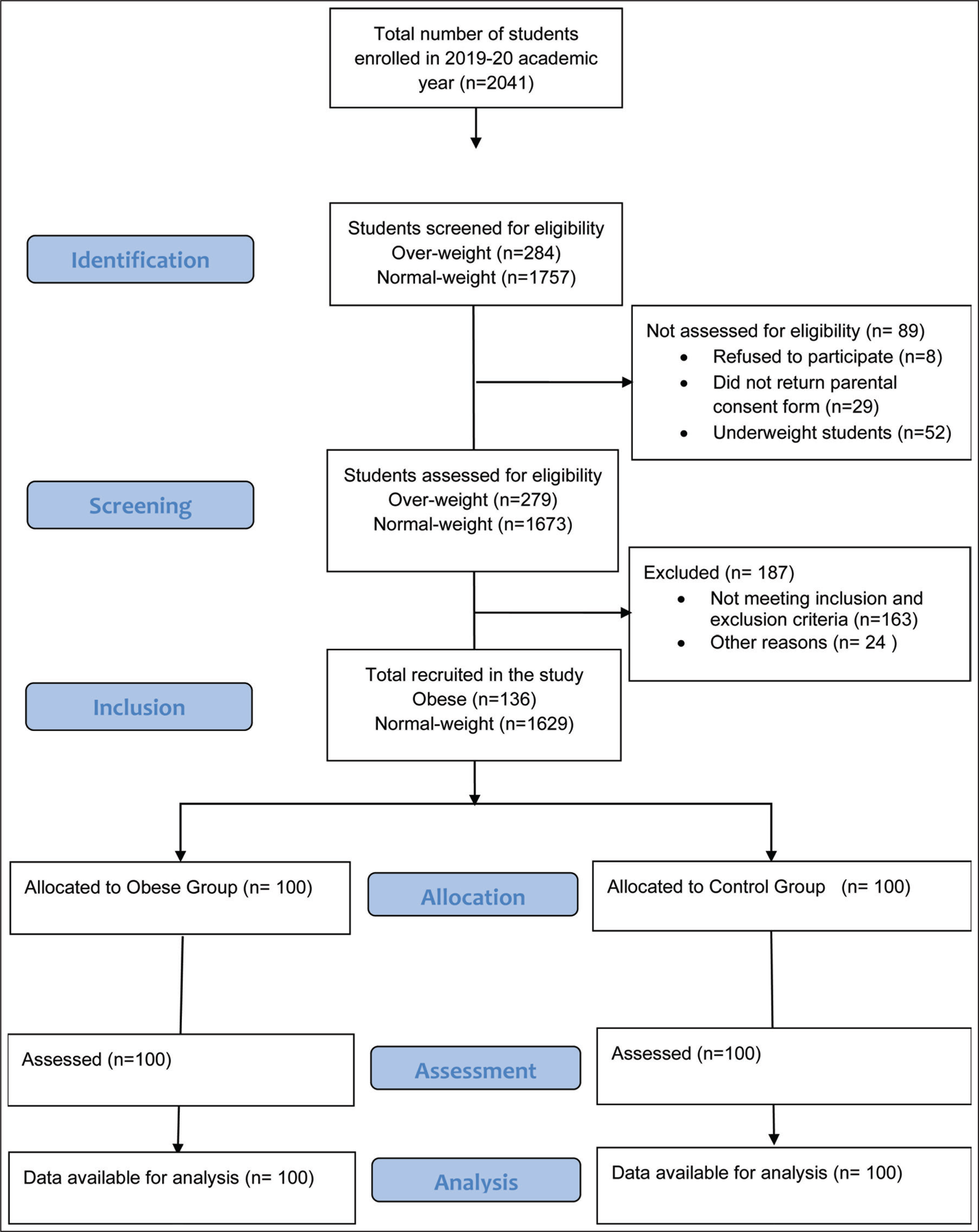
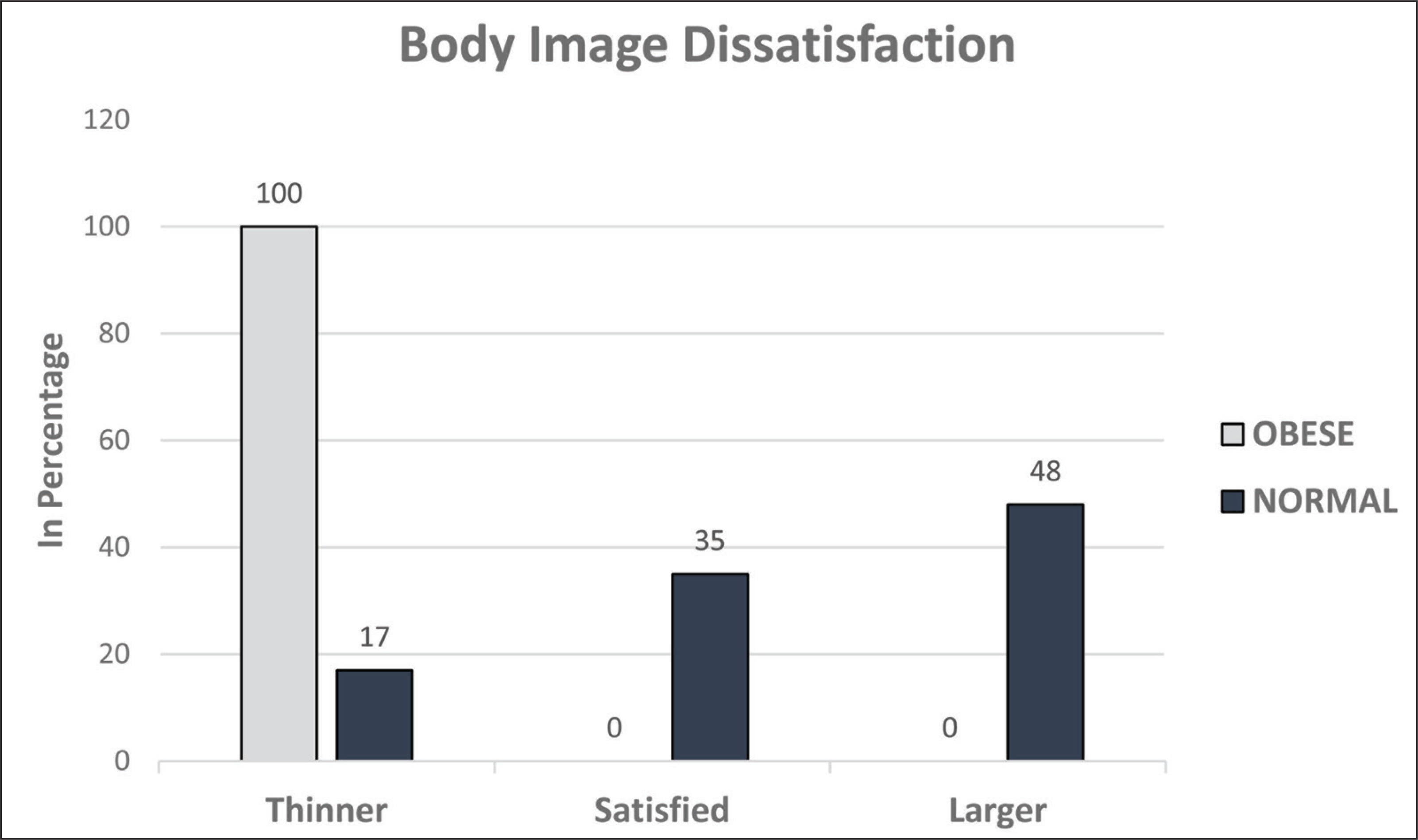
Figure 2 shows the discrepancy details of the BID among obese and normal-weight school children. All obese children were dissatisfied with their body image and preferred to be thinner. However, only 35% of normal-weight children were satisfied with their body image and 48% wanted to become larger.
Distribution of Body Image Dissatisfaction in Obese and Normal-Weight School Children
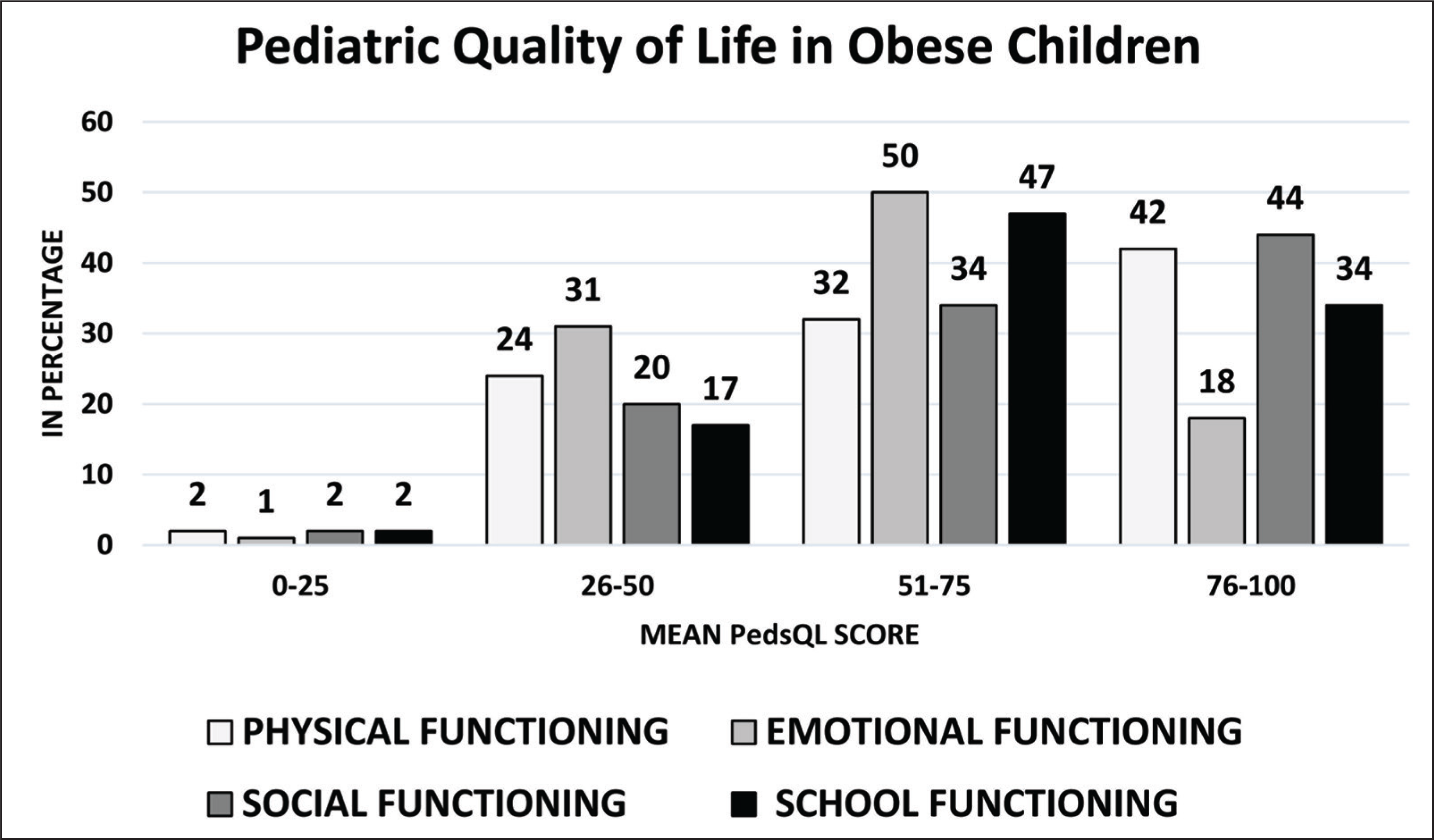
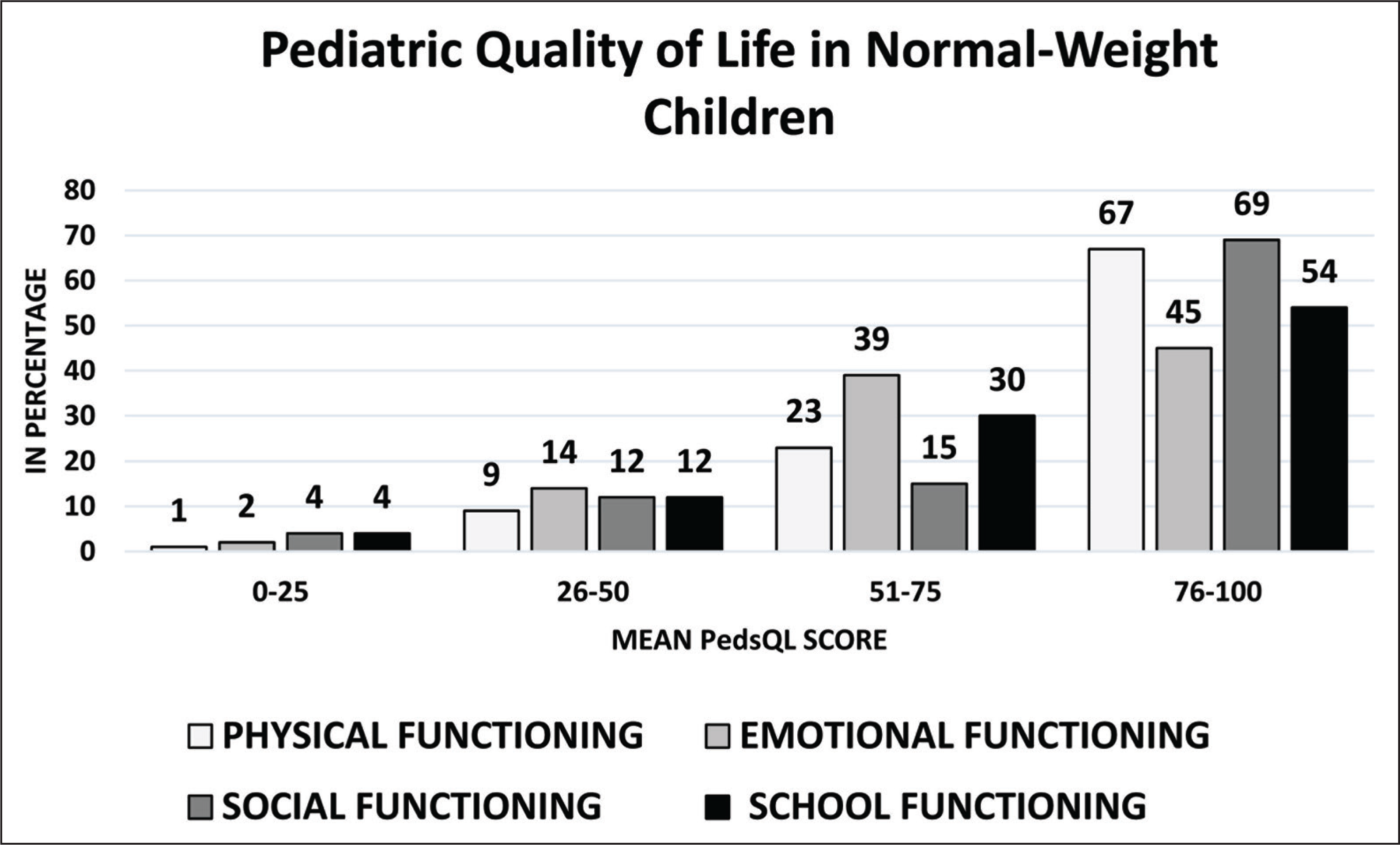
Figures 3 and 4 show the distribution of PedsQL for the obese group and control group, respectively. The analysis of depression in SMFQ disclosed that 54% of obese school children were depressed with a mean score of 7.76 ± 3.82. Simultaneously, 33% of normal-weight children were found to be depressed with a mean score of 6.65 ± 3.56. The mean score for total HRQOL in the obese group was 67.18 ± 16.02. Among these participants, 33% of them scored ≥ 75 (very good quality of life), 49% between the score of 51 to 75, 18% in 26 to 50 score, and none in the 0 to 25 score range. The control group, however, secured a mean score of 77.11 ± 16.72, among these participants 67% secured ≥75, 24% were in the score range of 51 to 75, 7% were in the 26 to 50 range score range, and 2% were placed in 0 to 25 score range.
Distribution of PedsQL Scores in Obese School Children
Distribution of PedsQL Scores in Normal-Weight School Children
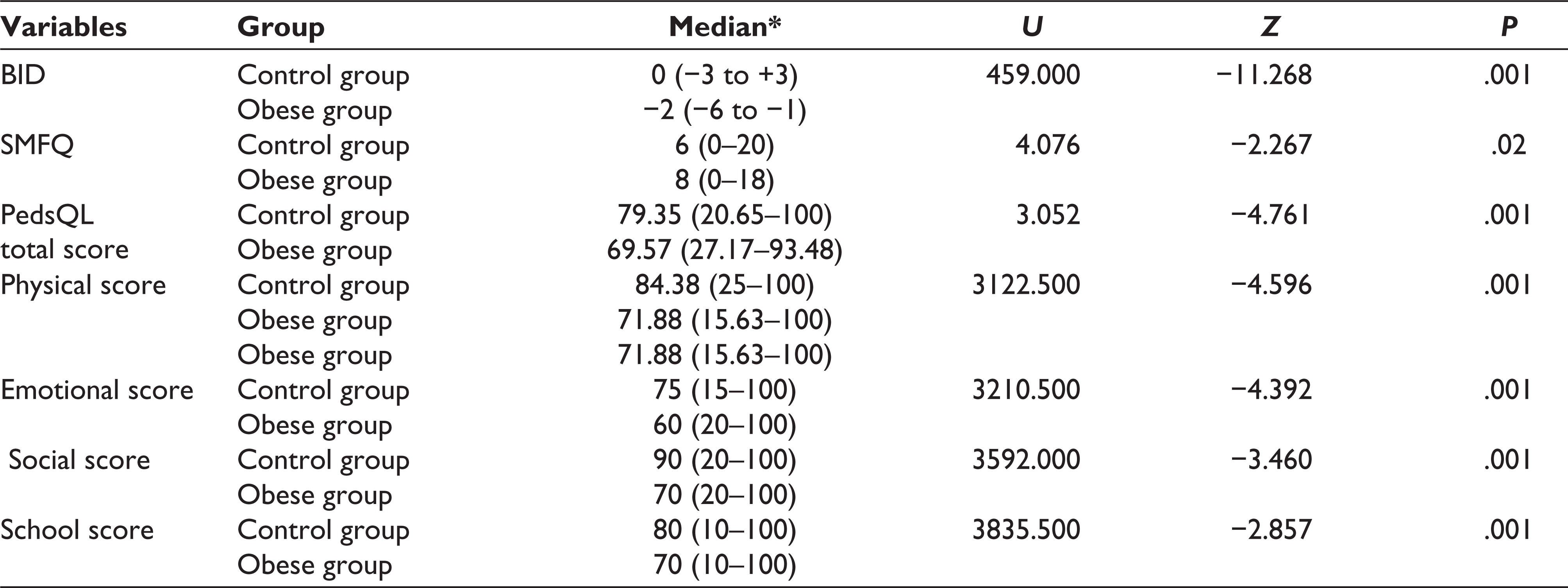
A Mann–Whitney U-test was used to perform an intergroup analysis between the control and the obese group. This test revealed a significant difference in BID in obese group (Md = −2, n = 100) and control group (Md = 0, n = 100), U = 459, z = −11.268, and P < .001. The other study variables also revealed a significant difference among the obese group, which is, shown in Table 2.
Intergroup Analysis Between Obese and Normal-Weight School Children
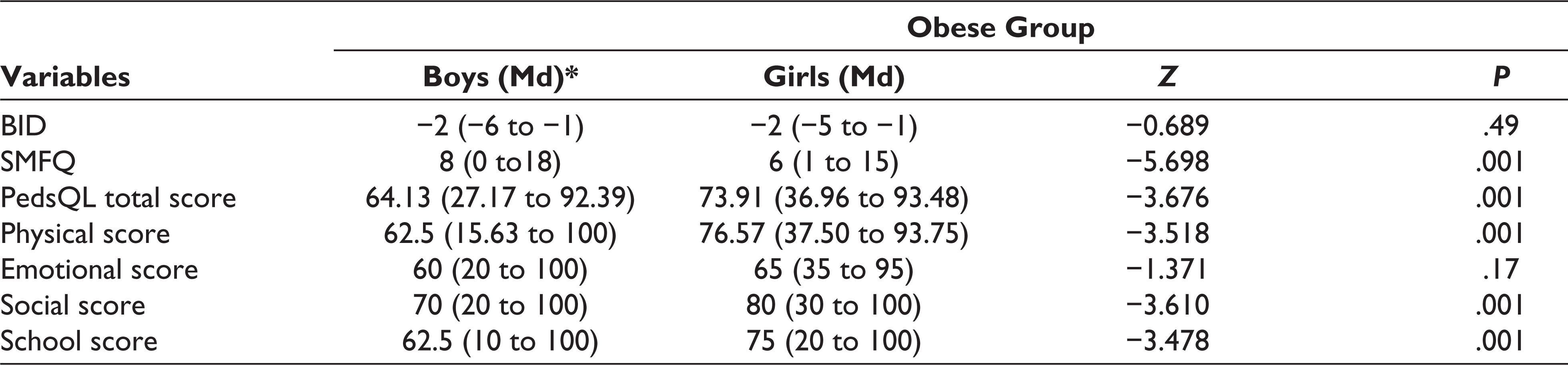
A Wilcoxon signed-rank test was performed to analyze obese children’s gender influence on BID, SMFQ, and HRQOL. It revealed a statistically significant increase in depressive symptoms among boys from the obese group, z = −5.698, P < .001. The median score on the SMFQ Scale for obese boys is Md = 8 to obese girls Md = 6. However, gender influence on BID and emotional score on the PedsQL showed no statistical difference and the details are shown in Table 3.
Comparison of the Gender Effect in Obese School Children
Discussion
This study analyzed BID, depression, and HRQOL among 100 obese and 100 normal-weight school children. The result of BID in this study confirmed that all obese children perceived equal BID. Simultaneously, 65% of normal-weight school children were also dissatisfied because of either desire to get thinner or bigger.
Multiple studies had disclosed a widespread association of BID not only with obese children but in adolescents as well.11, 17, 26 Similarly, this study demonstrated that obese children were more dissatisfied as compared with their normal-weight counterparts. Up till now, multiple factors have been identified to influence BID among obese children. It includes but is not limited to BMI, family, peers, society, media, culture, self-esteem, psychopathology, gender, age, education level, physical activity, weight control behavior, religiosity, and spirituality. 32 The majority of obese participants, during their meeting with the school counselor, disclosed that peer pressure influenced their BID, thus accepting or rejecting one’s body image. Mostly, peers share their ideas about what is normal or beautiful, and also express their desires about body appearance. 26 Thus, social comparisons among school-aged children, siblings, and peers, and sometimes bullying on their body size attributed to a higher rate of body dissatisfaction among our obese participants. Hence, all of them desired to get thinner. Because the BID has a detrimental effect on psychological well-being, it is mandatory to explore its correlates and address its appropriate management strategy.
Literature has found that depression and decreased quality of life are the few reported consequences of BID. Evaluation of depression using SMFQ in our study identified that 54% of obese and 33% of normal-weight children demonstrated depressive symptoms. Multiple studies revealed that weight-related teasing was closely related to low body satisfaction, low self-esteem, and high depressive symptoms.8, 33, 34 In our study, obese girls demonstrated lower depressive symptom scores as compared to boys. Primarily it may be because of their adequate coping strategy, also parental support to address the peer pressure, as observed by the investigators during the course of the study. Studies have suggested that children who have family support, good coping strategies, and emotional security are likely to have a positive body image and greater resilience thus decreasing depressive symptoms.35, 36 Moreover, we observed that few of our obese participants with depressive symptoms had developed unhealthy eating habits. “Limited eating” was reported among a few female obese children, that is, they used to share the majority of their lunch with their school friends. However, a few male obese children reported that they overeat (binge) to become stronger to fight out the bullies. Literature demonstrated that childhood depression may carry forward in adolescence and adulthood. Gaffrey et al 37 reported homotypic continuity of preschool depression into adolescence and the onset of puberty. They also suggested that preschool depression follows the path of the severity of depression which is elevated as compared with their peers, it continues from preschool through adolescence. 37 Wallin et al 38 in their cohort study reported an interrelation between poor academic performance and depression in early adulthood. 38 Therefore, early identification and prevention of depression in childhood is a need of the hour to protect psychosocial well-being.
Multiple studies revealed obese children are more prone to developmental symptoms and tend to have a poor quality of life as compared to their nonobese counterparts.34, 39 Pooled analysis of systemic review by Tsiros et al found a strong inverse negative correlation between BMI and specifically physical functioning of HRQOL. 18 In this study, among obese school children, observation of a specific domain of HRQOL reveals that emotional function was the most affected (62.40 ± 15.85), physical (67.31 ± 20.3) and school functioning (67.75 ± 18.86) were equally affected, while social functioning (71.20 ± 21.00) remains the least affected. However, in normal-weight children, emotional functioning (72.85 ± 19.52) was more affected and social functioning (80.25 ± 21.57) was the least affected. Nevertheless, the obese school children demonstrated decreased HRQOL as compared to nonobese. The literature identified that reduced physical performance/activity and social pressure lead to decreased emotional functioning in obese children. In this study, the possibility for poor emotional functioning maybe because of self-reported weight-related teasing. The observed better physical functioning in our participants could be because of motivated physical training teachers, initiation, and conduction of various sports activities, and schools’ support to “Fit India” health promotion. These factors effectively helped obese children to cope with their physical demands. Therefore, school’s motivation plays a vital role in building up confidence among obese children to improve their physical performance. Kolotkin et al in 2002 reported females scored less HRQOL score than males. 40 However, this study found obese boys scored fewer HRQOL scores than obese girls.
This study attempts to understand the obese school children’s perceptions about their body image, resulting in depression and quality of life impediments experienced by Indian school students. Obesity tends to affect our sense of body image which defines our thoughts, feelings, behavior, and also physical appearances, especially in young children. Indian society also culturally promotes a thinner body idyllic making it further challenging for young individuals to accept their body shapes and structures. The thin lines between real and ideal body image are blurred causing anxiety and dissatisfaction leaving an individual psychologically vulnerable.41, 42 During the data collection, obese children with higher depressive symptoms, were relatively detached because of the lack of normal body shape, while few others were extremely agitated because of body shaming by their classmates. In both cases, this behavior needs to be addressed and resolved as it may progress into unwanted manifestations and affect children’s psychological well-being. 33 It is essential to counsel normal-weight children along with obese ones in terms of body shaming which may include educational programs to halt the weight-related teasing in the school.
The obese persona is often perceived as lazy, inapp-ropriate, and incompetent and is often subjected to constant comparison of body weight, which influences a child’s thought process leaving a deep impact. 43 Such negative triggers must be challenged and the rising trend of the “Size 0 Figure” must be taken seriously, discouraged, and addressed in schools regularly. Education and health promotion programs must be initiated to provide awareness and knowledge about healthy diets and appropriate nutritional practices. The importance of intellectual prowess and academic achievements over body appearance needs to be highlighted. The cognitive-behavioral therapy (CBT) sessions by Das et al 44 proved to be efficacious in reducing depression in students with raised depressive symptoms. Parental and social support is very important to achieve the desired changes. 44 Children whose parents get involved positively with their child are at lower risk of depression in adulthood, especially in school age of 5 to 7 years which is a very crucial period; parental support prevents the early onset of depression more than at any other time point. 35 Hill et al 45 conducted an RCT demonstrating that their Confident Body, Confident Child (CBCC) program, which included 18 months of health promotion regarding healthy eating patterns and body image in parents of preschool children, had greater body satisfaction in children. 45
This study has a few potential limitations. It involved only a narrow age group of school children and not all the age groups in that category were considered. Normal-weight children in this study also demonstrated depressive symptoms and reduced emotional functioning in HRQOL. However, their causative factors were not identified, which is beyond the scope of this study. Moreover, all the confounding factors for depression in obese school children were not explored. We adopted a screening tool to assess the participant’s depression and thus lacked diagnostic assessment for their depression. Because obese school children are prone to demonstrate altered physical performance, in the future, their psychological well-being can be correlated to their level of physical activity.
Children are the budding future of our country. Their innocence needs to be valued and cherished. To change the sociocultural perceptions and norms, attempts need to be made to understand students’ mind. School is the place where a child spends maximum time making it simpler to mold them in every possible way. Open conversations among children, parents, and teachers about each one’s opinion about their body image, body ideals, and individual understanding of beauty, addressing the media’s wrong attitudes about slimness as a gold standard for beauty, healthy eating not dieting, improving physical activity not to lose weight but to be fitter, and the role of parental support must be encouraged. A multimodal approach is required to control obesity in early childhood. 46 Furthermore, parental, societal, and health education at preschool might help reduce bullying, provide encouragement and support, and eventually improve the quality of life.
Conclusion
To our knowledge, this is the only study that made an attempt to explore psychological well-being, especially among obese school children. In summary, all the obese school children in our study were dissatisfied with their body image and desired to get thinner. In addition, they also demonstrated higher depressive symptoms and lower quality of life as compared to normal-weight children. Gender influence among these obese school children correspondingly had also demonstrated that boys had higher depressive symptoms and decreased HRQOL as compared to girls. Because childhood obesity not only affects their physical performance but also psychosocial well-being, it is important to consider the mental health of obese children. Thus, it warrants a multimodal approach in catering to their needs for the positive development of one’s image.
Footnotes
Acknowledgements
We like to express our sincere gratitude to all the study participants and their parents who actively participated and/or were allowed to participate in this study without whom this would not be possible. We would also like to acknowledge the school authorities for permitting us to conduct this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.