
Abstract
Background
The simplest form of carbohydrate that the human body can utilize efficiently to fuel various functions in our body is glucose. The food that is consumed by us in any form is acted upon by pancreatic juices, bile, and several other digestive enzymes and is converted into its simplest form, which is absorbed by the small intestine and is diffused into the circulatory system; from there, it is transported to other organs via GLUT-2 and GLUT-4 transporters. This process is very important, and so are the hormones involved in it. One such major hormone responsible for glucose homeostasis in the body is insulin. Its malfunction or that of either of its signaling components leads to a metabolic disorder termed “diabetes.” Hyperglycemia is a grave condition associated with this complex disease and is of global concern. The impact of this disease can be life threatening if adequate precaution, medication, and therapy are overlooked. A plethora of synthetic drugs are available in the market, and the main goals of these antidiabetic medicines are to improve insulin sensitivity and/or production as well as to lower blood glucose levels. In all cases, frequent use of antidiabetic medication causes several after-effects.
Results
Numerous studies in this field demonstrate that antidiabetic phytomolecules are highly effective against diabetes patients and are almost completely without side effects. Almost all classes of phytomolecules have been thoroughly evaluated to develop the noble plant-based drug.
Conclusion
The current review discusses diabetes, its classification and management, worldwide occurrence, and the most crucial class of antidiabetic phytomolecules, for example, alkaloids, and terpenenoids as well as the parent molecule responsible for the bioactivity, subclasses, their mechanisms of action, plant sources and part, their superiority over synthetic drug, and new advances in this area.
Keywords
Introduction
Diabetes mellitus is a collection of metabolic illnesses that are depicted by chronic hyperglycemia resulting in deficiency in insulin action, insulin secretion, or both. The significance of insulin as a hormone required for anabolic processes is very crucial, and its malfunctioning leads to metabolic irregularities in lipids, proteins, and carbohydrates (Olokoba et al., 2012). Besides this, people suffering from this disease are more prone to cataracts, erectile dysfunction, non-alcoholic fatty liver disease, obesity, peripheral arterial disease, and heart disease (Olokoba et al., 2012). Keto-acidosis or a non-ketotic hyperosmolar condition, which can result in dehydration, coma, and death, in the absence of adequate and swift treatment, is the most serious concern (World Health Organization, 2019). An Egyptian Papyrus from 1,500 BC provides the initial description of diabetes, referring to “too large emptying of the urine” (Leutholtz & Ripoll, 2011). As ants were found near the urine of a diabetic person, an Indian physician later documented the illness and labeled it as honey urine (Poretsky, 2010). Due to the sweet taste of diabetic patients’ urine, Thomas Willis introduced the name “Mellitus” or “from honey” in the late seventeenth century (Poretsky, 2010). The Greek Apollonius of Memphis used the phrase “diabetes” or “to pass through” in approximately 250 BC (Poretsky, 2010), but there lies a discrepancy among people with regard to the origin of this term. The Indian doctors Sushruta and Charaka initially identified two different types of diabetes, namely, type 1 and type 2, around 400–500 BC, correlating type 1 diabetes with adolescents and type 2 diabetes with obesity (Poretsky, 2010). Aretaeus of Cappadocia, an ancient Greek physician, provided the first comprehensive clinical description of diabetes in the first century AD, but in some literature, Aulus Cornelius Celsus is credited for this. Aretaeus of Cappadocia identified excessive urination as a characteristic sign of diabetes (Trikkalinou et al., 2017).
Types of Diabetes and Management
Type 1 Diabetes
It was earlier also known as juvenile diabetes or insulin-dependent diabetes mellitus; basically, in this ß-cells of the pancreas are attacked by the patient’s immune cells, which results in loss of function of the pancreas to produce enough insulin, and glucose metabolism is affected. Although both men and women are equally impacted (Maahs et al., 2010) and even though type 1 diabetes (T1DM) frequently affects children, it can also develop in adults, and 84% of T1DM patients are adults (Patterson et al., 2009). Some people may have a rapid rate of β-cell destruction, whereas others have a slow rate.
Type 2 Diabetes
Type 2 diabetes is commonly known as adolescent diabetes or non-insulin-dependent diabetes mellitus; in this the body cells of an individual do not respond properly to insulin hormones, possibly due to defective insulin receptors, and slowly, the level of hormone also reduces. It is observed that type 2 diabetes (T2DM) is most prevalent in adults, but nowadays it is affecting a large number of children and adolescents as well (World Health Organization, 2016). It is a widespread and serious global health issue that has arisen because of quick changes in lifestyle, culture, economy, society, population ageing, unplanned urbanization, and dietary changes such as an increase in the consumption of highly processed foods and sugar-sweetened beverages.
Gestational Diabetes
Gestational diabetes is recorded in the fetus during pregnancy and resembles type 2 diabetes in many ways. There is a higher risk of adverse outcomes for the mother and for the fetus due to gestational diabetes. The possibility of acquiring diabetes later in life is higher for newborns whose moms have gestational diabetes and even for the mothers. The escalated likelihood of macrosomia (birth weight 4.5 kg), preeclampsia, preterm birth, etc. results in cesarean delivery due to hyperglycemia in pregnancy (Metzger et al., 2009)
Monogenic Diabetes
Monogenic diabetes is caused by a genetic defect in one gene in pancreatic β-cells, which impairs β-cell function or reduces the number of β-cells. Monogenic diabetes is typically divided into two categories based on when it first manifests: neonatal diabetes at a very early age of six months or maturity-onset diabetes of the young (MODY) at 25 years of age. However, certain hereditary abnormalities turn up as MODY, adult-onset diabetes, or neonatal diabetes (Canivell & Gomis, 2014).
Management of Diabetes
Type 1 Diabetes
To effectively manage the disease, people with T1DM need daily insulin administration, routine blood glucose testing, and a healthy lifestyle. Insulin shots must be taken by every individual diagnosed with type 1 diabetes to maintain blood glucose control. Depending on how quickly insulin shots start to function when they peak, and how long they last, numerous varieties of insulin exist. A syringe, insulin pen, or insulin pump is frequently used to administer insulin.
Type 2 Diabetes
With around 90% of all occurrences of diabetes being type 2, it can be declared as the universal kind of diabetes. Insulin resistance, which occurs when the body does not fully respond to insulin, is typically a key characteristic. Blood glucose levels continue to rise as a result of insulin’s inability to function effectively, releasing more insulin. For certain patients with T2DM, this may eventually exhaust the pancreas, causing the body to produce less and less insulin and raising blood sugar levels even further (hyperglycemia). Similar to T1DM, T2DM symptoms include excessive thirst, dry mouth, frequent urination, fatigue, insufficient energy, exhaustion, wounds that heal slowly, persistent skin infections, vision blur, and tingling or numbness in the hands and feet. People with T2DM may go undiagnosed for several years before they are finally found to have the disease since these symptoms can be minimal or non-existent (World Health Organization, 2019).
Worldwide Status of Diabetes
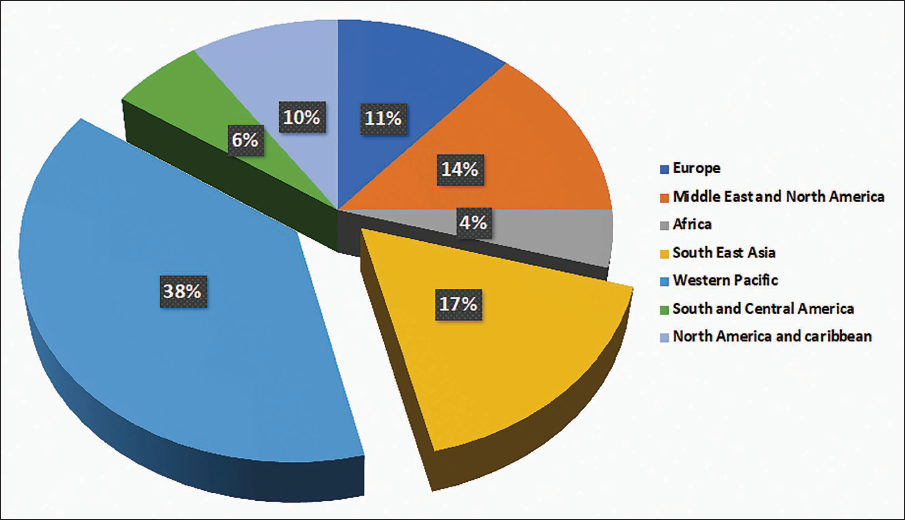
There are 537 million adults worldwide who have diabetes as of the latest data from the International Diabetes Federation (IDF. This represents an increase of 16% (74 million) from the IDF’s earlier forecasts for 2019. If this is the speed, then it is estimated that there will be 643 million diabetics worldwide in 2030, and 783 million by 2045. This would be a 46% increase from the present scenario, which is greater than the projected population growth for the same period (20%). The occurrence of diabetes has risen to 10.5% globally, according to the most current IDF Diabetes Atlas, with more than half (44.7%) of adults still undiagnosed. Over three-quarters of adults with diabetes live in low- and middle-income nations. Type 2 diabetes affects more than 90% of diabetics globally. Due to a complex combination of social, demographic, environmental, and genetic factors, type 2 diabetes is becoming increasingly common. 81% of these people live in countries with low and moderate incomes. The IDF 2019 report also presented the list of countries in which the top three containing the maximum number of individuals having diabetes are China (116.4 million), India (77.0 million), and the USA (31.0 million) (Ogle et al., 2022). In a gap of two years, the latest report of the IDF database, 2021, shows an almost similar trend with slight modification; again, the Western Pacific represents the maximum number of diseased individuals (206 million), and then comes the Southeast Asian region (90 million), whereas the Middle East and North America (73 million) came at the third place, pushing Europe (61 million) to the fourth place, while North America and the Caribbean (51 million) and South and Central America (32 million) followed a similar trend as of 2019 report (IDF, 2021) (Figure 1).
Type 2 Diabetes Mellitus Patient Status in 2021.
Antidiabetic Drugs and Their After-effects
The major groups of oral diabetes drugs are metformin, biguanides, sulfonylureas, meglitinide, thiazolidinedione (TZD), dipeptidyl peptidase 4 (DPP-4) inhibitors, sodium-glucose cotransporter (SGLT2) inhibitors, and α-glucosidase inhibitors. Blood sugar levels are lowered with oral sulfonylureas such as glimepiride and glyburide, mostly via increase in the islet of Langerhans insulin secretion (Salehi et al., 2019). For the treatment of T2DM in all age groups, metformin is the main first-line medicine of choice. By exhibiting complex effects on the mitochondrial enzymes, metformin causes the liver’s adenosine monophosphate–activated protein kinase to become active, causing hepatic uptake of glucose and inhibiting gluconeogenesis (Viollet et al., 2012). Nonetheless, the various metformin modes of functioning are yet to be understood, but gluconeogenesis, glycolysis, and glycogen production in the liver are said to be regulated by it. Metformin is absorbed by organic cation transporters after ingestion, where it is broadly dispersed in many tissues such as the colon, liver, and kidneys without being digested by the body. The kidney is the main organ of excretion. Although metformin has a very good safety profile, roughly 30% of people may experience gastrointestinal problems such as diarrhea, nausea, and dyspepsia when treatment begins.
Sulfonylureas increases insulin release in the pancreas by inhibiting KATP channels, which lowers blood glucose levels. This restrict liver gluconeogenesis as well. Sulfonylureas lessen the liver’s ability to clear insulin and decrease the breakdown of lipids into fatty acids (Proks et al., 2002). Sulfonylureas are currently recommended as supplemental or second-line treatments for T2DM. The most common adverse reaction to sulfonylureas is hypoglycemia; however, other less serious symptoms include headache, nausea, dizziness, and weight gain.
Alternate Source of Antidiabetic Agents: Medicinal Plants
Several herbal antidiabetic medications are employed in various traditional systems of medicine worldwide. Numerous and diverse plants are copious sources of bioactive components with specific pharmacological characteristics and almost no adverse side effects (Salehi et al., 2019). Communities in lower-middle income countries have high confidence in these medicinal herbs, and they are using low-cost medicinal plants to treat diabetes rather than synthetic ones (Arumugam et al., 2013). High-income countries are currently more likely to adopt traditional systems of medicine due to their zero side effects and wonderful results. Many phytoconstituents in medicinal plants, such as alkaloids, flavonoids, terpenoids, saponins, carotenoids, and glycosides, have antidiabetic properties (Tajner-Czopek et al., 2020). As of now, six general antidiabetic drug mechanisms can be identified based on the literature reviews (Chan et al., 2012).
Hypolipidemic Effect
Effects Like Insulin
Antioxidant Effect
This includes prevention of oxidative damage, which can cause cell impairment by scavenging free radicals (Kaneto et al., 2005), reducing H2O2 formation, inhibiting ROS production, modulating enzymes (cyclooxygenase, microsomal monooxygenase, NADH oxidase, xanthine oxidase, lipoxygenase, succinoxidase), and regulating the balance between antioxidants and oxidants inside the cells (Crespy & Williamson, 2004).
This review describes some important antidiabetic medicinal plants and their secondary metabolites with antidiabetic effects that include alkaloids, flavonoids, and terpenoids in general and their mode of action.
Medicinal Plants Containing Antidiabetic Properties
Alkaloids
The major classes of structurally diverse chemicals known as alkaloids, which are generated from amino acids, contain a heterocyclic ring with a nitrogen atom in it (Kaur & Arora, 2015). Alkaloids are further divided into various categories depending on their biosynthetic precursor and heterocyclic ring system, including indole, tropane, piperidine, purine, imidazole, quinolizidine, isoquinoline, pyrrolizidine, and pyrrolidine alkaloids.
Indole Alkaloid
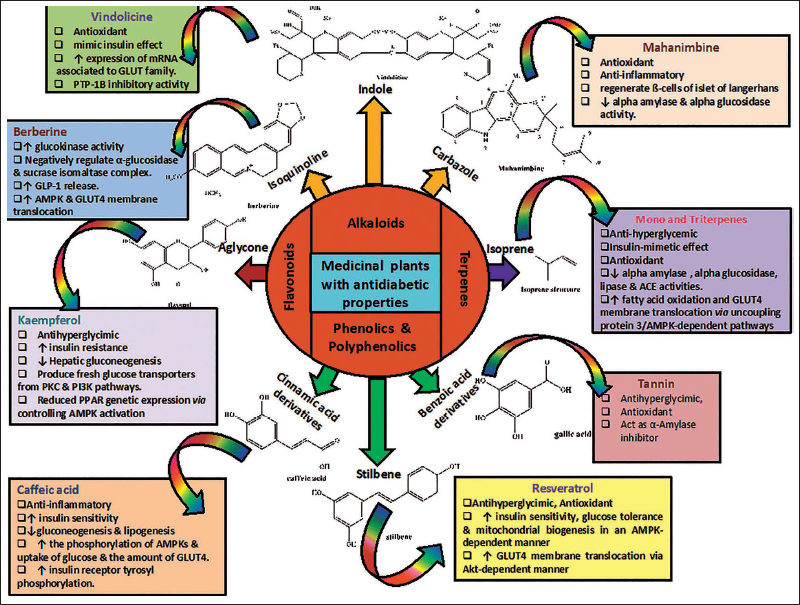
In this class of alkaloids, there are around 2,000 different chemicals, with vincamine, vincristine, vinblastine, strychnine, ajmalicine, and ajmaline molecules being more studied and researched. A pyrrole ring is fused to a benzene nucleus to form the weakly basic molecule known as indole (C8H7N), where 10 ύ electrons move around the structure (Omar et al., 2021). Plants from the Apocynaceae, Loganiaceae, Rubiaceae, and Nyssaceae families include a variety of indole alkaloids. Reserpine, an antihypertensive medicine from Rauvolfia serpentina, as well as the potent anticancer medications vinblastine and vincristine from Catharanthus roseus, are significant indole alkaloids that are extracted from their respective plants. More than 130 alkaloids have been reported from root and leaf tissues that are valuable economically. Apart from vinblastine and vincristine, an alkaloid vindolicine is suggested to exhibit an antidiabetic effect (Prasad et al., 2010). It has been noted that the fresh leaf juice of C. roseus lowers blood glucose levels in diabetic rabbits. The use of Catharanthus leaves and other parts as an antidote for the cure of diabetes has been approved by the pharmaceutical industry. In C. roseus, the mode of action still needs to be explored, but it has been hypothesized that the glucose transport GLUT family may be involved in glucose uptake (Figure 2). Overall, the action of insulin secretagogues may be due to amelioration in the genes GLUT-2 and GLUT-4, which are responsible for glucose transport and its direct action on protein transportation and fat metabolism.
Parent Phytomolecules and Their representatives with Respective Modes of Action Against Diabetes.
Vindolicine and Its Mode of Action
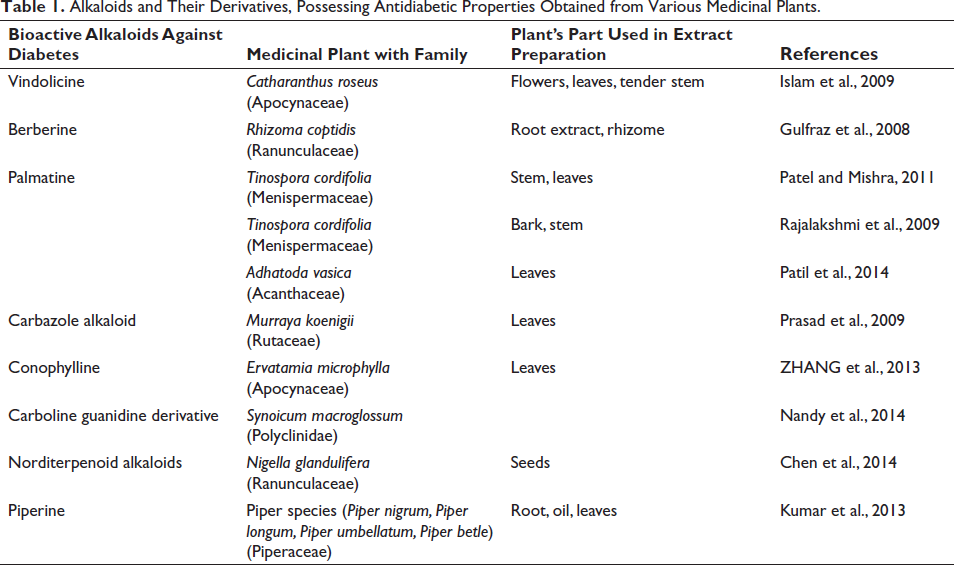
Vindolicine is derived from C. roseus and is used for the development of antidiabetic therapeutics. This study can be correlated to Prasad et al.’s (2009) study, which used an aqueous extract of leaves of three plants, Catharanthus roseus, Murraya koenigii, and Psidium guajava, to analyze antidiabetic properties (Table 1). Alpha-amylase and alpha-glucosidase inhibitory activities were also checked in aqueous and ethanolic extracts, respectively, of the flower and leaves of Catharanthus, and both the aerial extracts exhibit strong alpha-amylase inhibitory action, that is, 63% (in leaf) and 15% (in flower), compared to commercial drugs. In albino rats, plant leaf crude extract treatment resulted in the normal level of glucose concentration. The same extract also reduced the increased measures in cholesterol, low-density lipids (LDL), VLDL, triglycerides, and high-density lipids (HDL) in the diabetic group, compared to commercial drugs, which have a direct impact on the heart.
Alkaloids and Their Derivatives, Possessing Antidiabetic Properties Obtained from Various Medicinal Plants.
Important alkaloids present in Catharanthus are vinblastine, vincristine, vinorelbine, vindesine, ajmalicine, serpentine, and vindolicine. However, vindolicine, a drug used to treat diabetes, is the focus molecule in this article (Table 1
Isoquinoline Alkaloid
The structural isomer of quinoline alkaloids is called isoquinoline alkaloids. Based on the presence of different functional groups, they are classified into several subclasses, including simple isoquinolines, benzylisoquinolines, morphine alkaloids, phthalide isoquinolines, protoberberines, and ipecac alkaloids (Kaur & Arora, 2015). Plants from the families Papaveraceae, Berberidaceae, Fumariaceae, Menispermaceae, Ranunculaceae, Rutaceae, and Annonaceae are abundant sources of isoquinoline alkaloids (in the dehydro forms) (Table 1). These alkaloids are also abundant in a few plant species that are members of the Magnoliaceae and Convolvulaceae family (Kukula-Koch & Widelski, 2017). Many well-known medicinal plants, including Coptidis chinensis Franch or Rhizoma coptidis (family Ranunculaceae), Phellodendron chinense Schneid (family Rutaceae), and Mahonia bealei (Fort.) Carr., contain the principal component berberine (family Berberidaceae). R. coptidis belongs to the family Ranunculaceae and is widely used against many diseases, including type 2 diabetes (Wu et al., 2016).
Berberine and Its Mode of Action
Alkaloid berberine, which is a natural isoquinoline, is found in different families belonging to the same order Ranunculales, for example, Berberidaceae, Ranunculaceae, Menispermaceae, and Papaveraceae, and one family of the order Sapindales, that is, Rutaceae. Typical berberine-containing plants are R. coptidis (Ranunculaceae) and Phellodendron amurense (Rutaceae), Berberis species (Berberidaceae), Tinospora cordifolia (Menispermaceae), and Eschscholzia californica (Papaveraceae) (Table 1). The majority of alkaloids are typically alkaline and colorless, while berberine is an acidic compound distinguished by its bright yellow color (Jagetia, 2021).
The compounds RC (R. coptidis), jatrorrhizine, palmatine, epiberberine, berberine, and coptisine have potent inhibitory α-glucosidase properties (Jagetia, 2021). The sucrase isomaltase complex’s mRNA expression and the activity of disaccharidases in the protein kinase A-dependent pathway were both dramatically decreased by berberine when it was examined by several researchers in diabetic and non-diabetic rats (Liu et al., 2010). On the other side, in numerous human cell lines, the insulin receptor’s mRNA and protein expressions were elevated by berberine (Zhang et al., 2010). Furthermore, it boosted the expression of GLUT-4 mRNA in skeletal muscles and improved the expression of the insulin receptor substrate 1 (InsR), GLUT-1, and GLUT-3 in the brain (Sandeep & Nandini, 2017). When cells are in a low energy charge state, AMP-activated protein kinase (AMPK) is turned on to encourage the uptake and utilization of glucose as its major role is to manage glucose homeostasis in an organism. Berberine bi-directionally regulates the expression of AMPK in liver hepatocellular carcinoma hepatocytes (HepG2) and C2C12 myotubes cell lines, promoting glucose utilization by enhancing glycolysis, a consequence that may be unrelated to AMPK activation (Xiao et al., 2018).
Palmatine and Its Mode of Action
A protoberberine alkaloid identified in many dicot plant species such as Tinospora cordifolia (Kumar et al., 2017), Tinospora sagittata (Rong et al., 2016), R. coptidis, Phellodendron amurense (Sun et al., 2016), etc., T. cardifolia belongs to the family Menispermaceae, commonly known as Guduchi, which is a shrub and is useful in the treatment of several diseases such as diabetes, jaundice, skin disease, anemia, allergic conditions, urine disorder, and rheumatism. It also helps in immunity enhancement and subside infections, etc. The chemical constituents of T. cardifolia are diterpenene lactones, glycosides, steroids, sesquiterpenenes, phenolics, aliphatic compounds, essential oils, a mixture of fatty acids, and polysaccharides, which occur in various plant organs such as root, stem, as well as in whole plant. T. cordifolia contains numerous alkaloids and shares some of the alkaloid profiles of R. coptidis. The range of alkaloids present in tinospora are tetrahydropalmatine, palmatine, magnoflorine, tinosporin, tembetarine, berberine, isocolumbin, and choline.
In Table 1, hydroalcoholic and ether extraction of T. cardifolia shows antidiabetic properties, and it is attributed to alkaloids such as palmatine and berberine; the latter is already briefly discussed in the previous section. Through several research studies, it has been observed that palmatine presence in most of the antidiabetic plants advocates its anticipation to possess antidiabetic properties (Patil et al., 2010). The biological activity of palmatine and the influence of T. cordifolia on the aspects of expression of molecular markers of diabetes and the route were not fully examined, and very few research reports on palmatine activity are available to date (Patil et al., 2010). The drug is used against inflammation, bacteria-related gastrointestinal infections, urinary tract infections, respiratory tract infections, etc. in China (Zhang et al., 2018). Its antidiabetic activity is correlated with anti-sucrase and anti-maltase activities (Patil et al., 2010).
Carbazole Alkaloid and Its Mode of Action
Leaves of Murraya koenigii species are used in conventional medicine against diabetes and the responsible bioactive molecule here is an alkaloid carbazole, as the plant is the richest source of this alkaloid. The plant family under which it is placed is Rutaceae, commonly known as curry leaf, or kari patta. For centuries, M. koenigii has been used as a spice in cookery and has great medicinal value. Raw leaves are used for digestion-related diseases such as dysentery and diarrhea and to stop regurgitation.
It is documented that during chronic disease, oxidative stress increases in the body, resulting in the formation of free radicals that cause tissue damage. M. koenigii leaf extract either stimulates and/or regenerates ß-cells of the islet of Langerhans present in the pancreas, which functions by alleviating the oxidative stress in the body (Figure 2). This could be due to the free radical–clearing phenomenon of carbazole alkaloids present in the leaves (Tachibana et al., 2003). The possible mode of action by which carbazole and its derivative decrease blood sugar levels may be either by elevating peripheral glucose uptake or by enhancing insulin secretion from beta cells (Arulselvan & Subramanian, 2007).
Terpenoids
Terpenes are a class of naturally occurring chemicals that are primarily found in plants; however, some are also isolated from various other sources (Breitmaier, 2006). They represent a large family of natural hydrocarbons, a class of secondary metabolites formed from basic isoprene units containing five carbons. They are volatile compounds that give flowers and plants their aroma (Breitmaier, 2006). Terpenes and terpenoids (compounds that resemble terpenes) are classified according to the number of isoprene units, which range from one to many, found in the parent nucleus. According to the number of isoprene units (n) in the molecule, terpenes can be classified into the following classes: hemiterpenes (C5H8), monoterpenes (C10H16), sesquiterpenes (C15H24), diterpenes (C20H32), triterpenes (C30H48), tetraterpenes (C40H64), and polyterpenes (C5H8) n.
Monoterpenes
These molecules are made up of two isoprene units, represented by the general molecular formula (C5H8)2, and frequently have one double bond in their structure (Habtemariam, 2017). Terpenoids are commonly referred to as secondary metabolites formed via two separate biosynthetic routes either through the cytosolic mevalonic acid route (MVA) or through the plastidial non-mevalonate route, also known as 2-C-methyl-D-erythritol 4-phosphate (MEP) route (Rehman et al., 2016). The terpenoid family of natural products, which includes monoterpenes, is a principal class of secondary metabolites exhibiting a diverse range of functions at cell and molecular levels that support it as a favorable therapeutic index. Additionally, their accessibility, low level of negative consequences, and improved safety account make them a propitious source for developing novel, efficient treatments for diabetes mellitus (Al Kury et al., 2021). More than 30 known skeletons contain monoterpenes, which are divided into three subgroups (Brahmkshatriya & Brahmkshatriya, 2013).
The main compounds of acyclic monoterpene are linalool, citral, geraniol, citronellol, and linalyl acetate.
Linalool
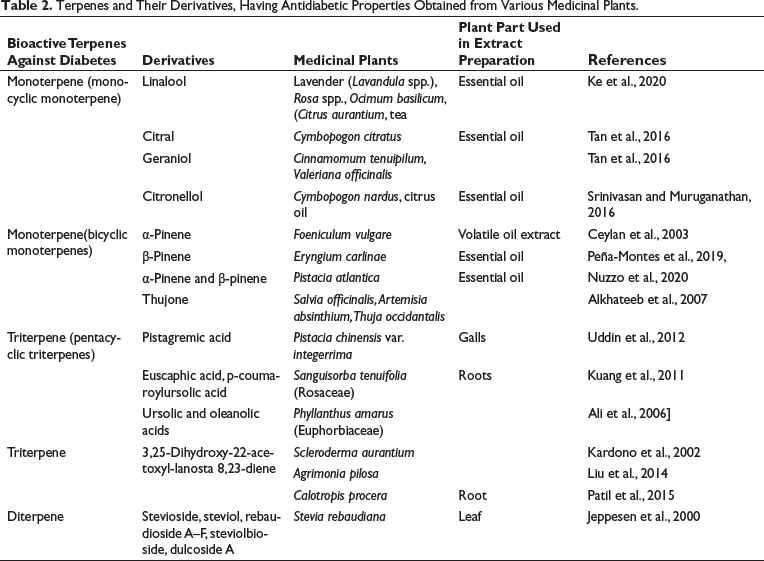
Linalool (3,7-dimethyl-1,6-octadiene-3-ol) is one of the primary acyclic monoterpenes that exist in essential oils of various herbs, including lavender (Lavandula spp.), rose (Rosa spp.), basil (Ocimum basilicum), and neroli oil (Citrus aurantium) and is present in different varieties of tea (Table 2). Various types of research support that linalool exhibits a beneficial impact on glucose metabolism (More et al., 2014). Garba et al. (2020) explored the antidiabetic effects of lemongrass tea and reported that its consumption decreases blood sugar levels by 60.3%.
Terpenes and Their Derivatives, Having Antidiabetic Properties Obtained from Various Medicinal Plants.
Citral
Citral (3,7-dimethylocta-2,6-dienal) is a compound that consists of the cis and trans isomers geranial and neral, respectively. It is found in all kinds of citrus fruits as well as in lemon grass (Cymbopogon citratus) (Shah et al., 2011). In earlier research, citral was found to lessen hyperglycemia and diabetes-related problems (Najafian et al., 2011). On α-amylase, citral has a 45.7% inhibitory effect.
Monocyclic Monoterpene
The main compounds of monocyclic monoterpene are limonene, carveol, terpineol, thymol, p-cymene, and menthol.
Limonene
Limonene [1-methyl-4-(1-methylethenyl)-cyclohexene] is found in citrus oil obtained from orange, lemon, and grapefruit. Previously, researchers (More et al., 2014) had documented that limonene subsided hyperglycemic and diabetes-related complications. It is well accepted that preventing protein glycation reduces secondary complications in diabetes, and a publication by Bacanlı and the group in 2017 primarily focused on the same aspect such as how the protective impact of D-limonene acts to subside diabetes and its further effects on glucose metabolism.
Thymol
Thymol (2-isopropyl-5-methylphenol), a naturally occurring phenolic monoterpenoid that is mostly found in the Thymus species (Trachyspermum ammi L. Sprague), also known as ajwain (Capetti et al., 2020), is used as a herbal medicine to treat several conditions, including diabetes, respiratory problems, etc. (Bouyahya et al., 2020). A potent antioxidant, thymol also acts as an effective hydroxyl radical and superoxide anion scavenger (Abbasi et al., 2018). Along with this, it also possesses antibacterial (Miladi et al., 2017), anti-inflammatory (Veras et al., 2013), and anticancer properties (Kang et al., 2016). It was found that thymol treatment reduces overall weight and visceral fat pad weight. In addition, a general decrease in lipid profile was also seen. Apart from that, the function of a few metabolic enzymes such as aspartate aminotransferase, lactate dehydrogenase, and alanine aminotransferase were also decreased. Overall, thymol reduces serum lipid peroxidation, lowers glucose and leptin amounts, and enhances antioxidant levels (Haque et al., 2014).
Bicyclic Monoterpenes
The main compounds are α- and β-pinene, thujone, myrtenal, genipin, geniposide, and catalpol.
α-Pinene and β-Pinene
α-Pinene [(1S,5S)-2,6,6-trimethylbicyclo[3.1.1] hept-2-ene ((-)-α-pinene)] is a key ingredient in the herb Foeniculum vulgare’s volatile oil extract (fennel) (Table 2). Fennel has been shown to have anti-inflammatory, hypoglycemic, and hepatoprotective properties (Ceylan et al., 2003). After 24 hours of treatment with α-pinene, hypoglycemia was observed in those mice that possess alloxan-induced diabetes.
Genipin and Geniposide
Iridoids have a cyclopentane-[C]-pyran ring joined to six-membered heterocyclic oxygenates as their primary structural skeleton (Nathia-Neves et al., 2018). The iridoids genipin [methyl-1-hydroxy-7-(hydrozymethyl)-1,4a,5,7 tetrahydrocyclopenta[c]pyran-4-carboxylate] and geniposide [methyl (1S,4aS,7aS)-7-(hydroxymethyl)-1-[(2S, 3R,4S,5S,6R)-3,4,5-trihydroxy-6-(hydroxymethyl)oxan-2-yl] oxy-1,4a,5,7a tetra hydro cyclopenta [c] pyran-4-carboxylate] act as a secondary metabolite and are detected in many plants. Raw fruit of Genipa americana L. (genipa) possess genipin, whereas Gardenia jasminoides J. (gardenia, Rubiaceae family) fruits contain geniposide, a substance with choleretic and hepatoprotective properties, which is harnessed as an herbal medicine in China. The intestinal microflora enzymes convert geniposide to genipin, indicating that blood contains mainly genipin and is responsible for various bioactivity (Wang et al., 2008). It has been demonstrated that genipin exhibits anticancer, anti-inflammatory, hepatoprotective, and anti-oxidative activities (Shanmugam et al., 2018). Almost similar biological activities have also been reported in the case of geniposide, such as anti-inflammatory (Koo et al., 2006), anti-oxidative stress (Wang et al., 2015), and anti-apoptotic effects (Jiang et al., 2016).
Triterpene
Triterpenoids are organic molecules with a six-isoprene unit carbon skeleton that are derived biochemically from the acyclic C30 hydrocarbon squalene. Triterpenoids have pentacyclic or tetracyclic structures, and the pentacyclic triterpenes can be further divided into lupanes (betulin, lupeol, and betulinic acid), oleananes (oleanolic and maslinic acids), and ursanes (asiatic, ursolic, and corosolic acids) (Putta et al., 2016). The most extensively studied antidiabetic substances are pentacyclic triterpenes and their derivatives and the chief triterpenes that exhibit antidiabetic activities include oleanolic acid, ursolic acid betulinic acid, and maslinic acid (Sangeetha & Rajamani, 2019).
Oleanolic Acid
Oleanolic acid (3-hydroxy-olean-12-en-28-oic acid) is a naturally occurring oleanane group product that can be found in many different plants as a free acid or in the form of triterpenoid saponin (Castellano et al., 2013). Oleanolic acid’s effectiveness in preventing chemically induced acute liver damage, fibrosis, and cirrhosis brought on by chronic liver diseases has proved its hepatoprotective properties. Oleanolic acid is an interesting antidiabetic drug since it is not adipogenic and is considered superior to synthetic antidiabetic drugs (Ayeleso et al., 2017).
Ursolic Acid
Ursolic acid is isolated from several plant species, including rosemary and lavender, apple fruit peel, organum, thyme, berries, and flowers (Table 2). Ursolic acid is considered to be the most promising triterpene because of its various biological activities. Commercially, this substance is extensively used in health-related items due to its demonstrated anti-cancer, antidiabetic, hepatoprotective, anti-inflammatory, anti-obesity, cardioprotective, antioxidant, and anti-apoptotic activities (Yu et al., 2015).
Terpene’s Antidiabetic Mechanism
There are various methods for treating type II diabetes, but here the mode of action of some terpene molecules and their derivatives against diabetes has been discussed briefly (Figure 2).
Terpene: Insulin-mimetic Effect
Diterpenes such as stevioside and steviol, extracted from the foliar region of the herb Stevia rebaudiana, exhibited elevated insulin secretion in normal mouse’s islet ß-cells and the INS1 cell line. In both cases, elevated insulin production may be associated with enhanced glycolysis and reduced gluconeogenesis either by stimulating the genes of this pathway or by blocking phosphorylation of ATP and oxidase activity of NADH (Jeppesen et al., 2000). In type II diabetes in Gotokakizaki rats, a diterpene stevioside treatment resulted in anti-hyperglycemic, insulinotropic, blood pressure lowering, and glucagonostatic effect. The anti-hyperglycemic activity of Cleome droserifolia was also attributed to its insulin-like effects in peripheral tissues (Motaal et al., 2011). The Costus speciosus increases the capacity of muscle and adipose tissue to absorb glucose that affects peripheral tissues, a mechanism that is more or less similar to that of insulin hormone. Interestingly, it encourages the regeneration of any surviving cells as well (Eliza et al., 2009).
Conclusion
There are several synthetic drugs based on sulfonylurea, biguanides (metformin), thiazolidinediones, etc., as principal molecules are available that are very effective in treating the symptoms but cannot cure the disease. Since the sick individuals must take these medications regularly for an extended period, several drug-related ailments have emerged as side effects. That is the reason why researchers worldwide are rigorously fetching the conventional system of medicine against diabetes to develop a completely safe plant-based drug. However, due to procedural shortcomings in the research, it has been impossible to make conclusions about the effectiveness of these treatments; also, there is not enough data to support the recommendation. Nevertheless, people in lower-middle income countries still have an opinion that ayurvedic medicine with a balanced diet, adequate sleep, and regular yoga can even cure diabetes. In the twenty-first century, when the human race is highly equipped with modern technology and internet revolution, people are more aware of the treatment and the side effects associated with the drugs administered, resulting in the development of a totally new branch of science known as “pharmacogenomics,” a study that can provide a tailor-made medication based on how genes affect an individual’s response against drugs. Furthermore, the world’s scientific community’s joint efforts resulting in developing whole genome data of several medicinal plants will certainly help researchers to get better insights into phytomolecules and their synthesis and will lead to the development of plant-based drugs against diabetes with zero side effects. In accordance, this review will help the readers to understand the actual and diverse group of phytomolecules, their respective plant sources, and the underlying mechanism against diabetes.
Abbreviations
GLUT-2: Glucose transporter 2; GLUT-4: Glucose transporter 4; T1DM Type 1 diabetes; T2DM: Type 2 diabetes; MODY: Maturity-onset diabetes; IDF: International Diabetes Federation; TZD: thiazolidinedione; DPP-4: Dipeptidyl peptidase 4; SGLT2: Sodium-glucose cotransporter; RC: Rhizome coptidis; INSR: Insulin receptor substrate 1; AMPK: Amp-activated protein kinase; Hepg2: Hepatocellular carcinoma hepatocytes; MVA: Mevalonic acid route; MEP: 2-C-methyl-D-erythritol 4-phosphate
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethical Approval and Informed Consent
Not applicable.