
Abstract
Background
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most common chronic liver disease in the world. It is strongly linked to obesity, high blood pressure, type 2 diabetes and dyslipidaemia. Yoga, which includes asanas, pranayama, shat-karmas and meditation, may offer a holistic approach to improve the liver, metabolism and mental health.
Purpose
To evaluate the effectiveness of a 60-min yoga module in improving liver health and metabolic parameters in MASLD patients.
Methods
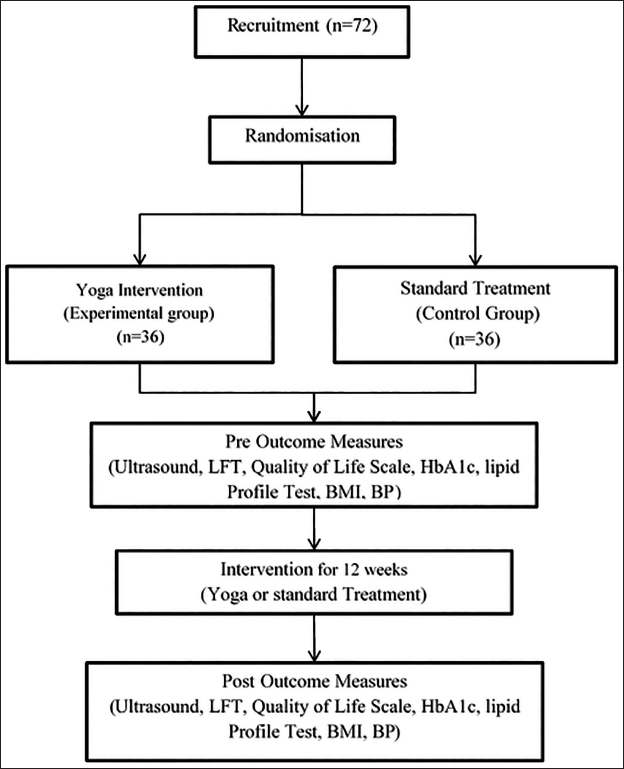
This open-label, two-arm, randomised controlled trial enrolled 72 adults aged 18–60 years diagnosed with MASLD, who received standard care at a hospital in Dehradun. Participants were randomised equally into a yoga group, which received a 60-min online yoga module 5 days per week for 3 months, or a control group receiving standard treatment alone. Key assessments include ultrasound measurement of liver fat, liver enzymes (serum glutamate pyruvate transaminase [SGPT], serum glutamic-oxaloacetic transaminase [SGOT]), HbA1c, lipid profile, body mass index, blood pressure, mental health and quality of life. Data collection occurred at baseline and 3 months post-intervention.
Results
The study is designed to assess improvements in hepatic steatosis and metabolic and psychosocial parameters following intervention.
Conclusion
This trial will provide evidence on the role of yoga as an adjunct therapy in MASLD management.
Keywords
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the updated term for non-alcoholic fatty liver disease (NAFLD).1, 2 It is a kind of chronic liver disease. The condition is defined as the build-up of fat in liver cells without much inflammation or liver damage. 3 Due to its strong link to metabolic syndrome, obesity and type 2 diabetes, MASLD is the most common ongoing liver disease in the world. 4 The increase in MASLD cases is primarily linked to lifestyle factors such as unhealthy diet, inactivity and stress, making it a significant contributor to the burden of chronic disease globally. 5 In total, 38% of adults and 7%–14% of children around the world are affected by MASLD, and the number of people with it is steadily rising. It is expected that MASLD will affect more than half of all adults by 2040. 6 It is a major cause of liver-related complications, including being the leading cause of liver transplant in women and patients with hepatocellular carcinoma (HCC) in the USA. 6 In India, the rates of MASLD, fibrosis and cirrhosis are 68.2%, 33.7% and 12.2%, respectively. 7 The North Zone has the highest rate of MASLD (73.3%), and Uttarakhand has the highest rate of all states at 80%. 7 However, it is important to note that the study of Mohan et al. 7 was based on clinic-based sampling from individuals attending diabetes and endocrine clinics, which may overestimate prevalence compared to the general population.
Yoga is a useful complement to lifestyle changes for fatty liver disease; it significantly decreases liver enzymes like alanine aminotransferase (ALT) by 20%–30% and aspartate aminotransferase (AST) by 15%–25% (p < .05), which means improvement in liver functions.8, 9 It improves the metabolic markers like blood sugar, cholesterol and triglycerides with significant decrease.8, 10 Imaging studies indicate reduced liver fat and stiffness, emphasising the reversal of fatty infiltration.8, 11 Yoga improves insulin sensitivity and decreases inflammation associated with stress.12, 13 Combined with dietary modifications, yoga shows synergistic improvement in liver function and fat metabolism, making it a valuable complementary therapy for managing fatty liver disease.8, 10–13
The current study aims to assess the effectiveness of yoga practices in reducing fatty liver in individuals diagnosed with MASLD. It also wants to investigate the effect of yoga on liver enzyme levels as a sign of liver health, as well as its impacts on obesity, blood pressure, lipid profile parameters and type 2 diabetes control. The study also looks at how yoga might help people with MASLD feel better mentally and emotionally. This helps to understand how yoga can help people with metabolic liver disease. Most importantly, this study protocol introduces the initial randomised controlled trial assessing a newly formulated, structured online yoga module specifically tailored for adults with MASLD. The novelty of this research lies in its customised implementation of traditional yogic elements—such as asanas, pranayama, shat-karmas and meditation—facilitated through an accessible online platform to enhance convenience and compliance. This study systematically evaluates this module, addressing a key gap in existing MASLD management tactics, which mainly focus on traditional lifestyle modifications while lacking standardised, evidence-based mind–body approaches.
Methods
Study Design
This study is an open-label, two-arm, randomised controlled superiority trial, as illustrated in Figure 1. The trial protocol follows the Consolidated Standards of Reporting Trials (CONSORT) 2025 guidelines to make sure clear and transparent reporting of randomised trials. 14 Participant enrolment, assessment time points and variables measured during the trial are scheduled as outlined in Table 1, following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines, which standardise protocol elements for clinical trials. 15 The SPIRIT 2013 checklist is provided in Supplementary Material S1.
Participants Enrolment, Intervention and Assessments as Per Standard Protocol Items: Recommendations for International Trials (SPIRIT).

Sampling
Patients diagnosed with MASLD from the Department of Gastroenterology of a tertiary care hospital in Uttarakhand were enrolled in the study. After obtaining informed consent and completing baseline assessments, eligible participants were randomly assigned in a 1:1 ratio to either Group A (yoga) or Group B (control).
Sample Size Calculation
The sample size was calculated using G*Power software (version 3.1.9.4) 16 for comparison between two independent means (two-tailed test). The effect size (Cohen’s d = 0.71) was derived from the between-group difference in mean change in globulin levels based on Sharma et al. 9 The mean change in globulin was 0.45 in the experimental group and 0.16 in the control group, yielding a between-group difference of 0.29. The pooled standard deviation (SD = 0.41) was calculated using the post-intervention SDs of both groups.
Based on these parameters, with a significance level (α) of 0.05 and statistical power (1−β) of 90%, the required sample size was estimated to be 33 participants per group (total n = 66). To account for an anticipated attrition rate of approximately 10%, the final sample size was increased to 72 participants, with 36 participants allocated to each group.
Participants
Inclusion Criteria
Individuals diagnosed with MASLD or NAFLD were selected based on the following clinical and diagnostic criteria: Adults aged 18–60 years. Participants with stable liver function and no signs of acute liver failure. Individuals with metabolic risk factors such as obesity, type II diabetes, dyslipidaemia or hypertension. Participants who are medically fit to perform yoga as assessed by a physician. Patients willing to provide informed consent and participate in the study. Individuals with stable mental health, without severe psychiatric disorders that could interfere with participation.
Exclusion Criteria
Patients with a history of excessive alcohol intake or alcohol-related liver disease.
Presence of other liver conditions such as hepatitis, cirrhosis or autoimmune liver diseases.
Patients with severe cardiovascular disease, end-stage renal disease, active cancer or any other life-threatening illness.
Pregnant or breastfeeding women.
Individuals with musculoskeletal disorders or neurological impairments that prevent safe participation in yoga exercises.
Individuals unwilling to adhere to the study protocol, attend regular sessions or complete follow-up assessments.
Patients who are already performing yoga, going to gym or have incorporated any other form of weight loss regimen or diet in their routine.
Randomisation
After baseline assessment, eligible participants were randomly allocated in a 1:1 ratio to either the yoga group (60 min of yoga) or the control group (standard care). The allocation sequence was generated using a computerised random number program in Microsoft Excel and concealed using sequentially numbered, opaque, sealed envelopes to ensure allocation concealment and minimise bias.
Treatments
Yoga Group
A validated yoga module with a content validity index (CVI) of 0.84 was developed, including sukshma vyayama (joint rotation exercises), scientifically designed asanas (postures), pranayama (breathing techniques), shat-karmas (cleansing techniques) and meditative practices. This module was practiced for 3 months, 5 days per week. Adherence to the intervention was monitored through attendance records, and participants attending at least 80% of the prescribed sessions were considered adherent and included in the per-protocol (PP) analysis. A brief description of the yoga module is provided in Table 2.
Components and Steps of Yoga Module.

Control Group
A standard treatment was prescribed by the gastroenterologist.
The Template for Intervention Description and Replication (TIDieR) checklist is provided in Table 3.
Description of Interventions Using the Template for Intervention Description and Replication (TIDieR) Checklist.

Outcomes
The primary outcome was the comparison of changes in liver fat content after 3 months of practicing the daily yoga module versus standard treatment alone in MASLD patients. Secondary outcomes included the comparison of changes in liver enzyme levels (serum glutamate pyruvate transaminase [SGPT], serum glutamic-oxaloacetic transaminase [SGOT]), glycaemic control assessed by HbA1c, lipid profile parameters, obesity measures, blood pressure and quality of life between the yoga group and the standard treatment-alone group.
Study Tools
Participants’ demographic information, including name, age, gender, lifestyle factors and medical history, was recorded.
Ultrasound (USG) was used to assess liver fat content using the Mindray DC-60 system.17, 18 Hepatic steatosis was graded based on standard ultrasonographic criteria into four categories: Grade 0 (normal liver echotexture), Grade I (mild steatosis with slight increase in hepatic echogenicity and normal visualisation of diaphragm and intrahepatic vessel borders), Grade II (moderate steatosis with impaired visualisation of intrahepatic vessels and diaphragm) and Grade III (severe steatosis with marked increase in echogenicity and poor or no visualisation of intrahepatic structures). In addition, liver stiffness (elasticity) was measured and expressed in kilopascals (kPa) as an indicator of hepatic fibrosis. All ultrasound assessments were performed by an experienced radiologist.
Liver function tests (LFTs), including SGPT/ALT and SGOT/AST, were measured using fully automated VITROS 5600/XT 7600 analysers (Ortho Clinical Diagnostics, USA). The VITROS dry-slide chemistry system was used for multilayer enzymatic or dye-binding reactions with reflectance spectrophotometry for quantitative analysis. ALT and AST were estimated through kinetic enzymatic methods. All measurements followed standardised calibration procedures and internal quality control protocols. 19
HbA1c was estimated from ethylenediaminetetraacetic acid (EDTA) whole blood using high-performance liquid chromatography (HPLC) on the Bio-Rad D-10 HbA1c analyser (Bio-Rad Laboratories, USA). This ion-exchange chromatography method separated glycated and non-glycated haemoglobin fractions and expressed HbA1c as a percentage of total haemoglobin. This technique is widely regarded as a gold standard for HbA1c measurement. 20
All lipid profile parameters (total cholesterol, triglycerides, high-density lipoprotein cholesterol [HDL-C], low-density lipoprotein cholesterol [LDL-C] and very-low-density lipoprotein cholesterol [VLDL-C]) were analysed using fully automated clinical chemistry analysers VITROS 5600 or VITROS XT 7600 (Ortho Clinical Diagnostics, USA), which use dry-slide, multilayer enzymatic colorimetric methods. Total cholesterol was estimated using VITROS CHOL Slides, based on the enzymatic method. Triglycerides were measured with VITROS TRIG Slides, adapted from the lipase–glycerol kinase–glycerophosphate oxidase method. HDL–cholesterol were quantified directly using VITROS HDL Slides, which employ a precipitation-free enzymatic technique with selective masking of non-HDL lipoproteins. LDL-C and VLDL-C were calculated using Friedewald’s formula. 21 All assays followed manufacturer-recommended calibration and internal quality-control procedures. 19
BMI was calculated as weight (kg) divided by height squared (m²). It assesses general obesity levels, which correlate closely with MASLD severity and outcomes. BMI serves as a simple and effective tool to monitor changes in obesity status resulting from interventions.
The standardised auscultatory sphygmomanometer method was used to measure blood pressure. The person sat comfortably after at least 5 min of rest, and their left upper arm was supported at heart level. A correctly sized cuff was chosen based on the size of the arm, and the systolic and diastolic pressures were found by listening for the sound of arteries (Korotkoff Phase I) and disappearance (Korotkoff Phase V). Two readings were taken 1–2 min apart, and the average was used as recommended. 22
To find out the quality of life of the participants, the Hindi version of the World Health Organization Quality of Life-BREF (WHOQOL-BREF) questionnaire was used. There are 26 items on this tool, which are divided into four areas: physical health, mental health, social health and the environment. The Hindi WHOQOL-BREF has shown great reliability with Cronbach’s alpha coefficients between 0.869 and 0.938 across all domains, which means that it has high internal consistency. 23 It has been shown to be valid and reliable in Hindi-speaking groups, so it is a strong tool for measuring quality of life in this study.
Blinding
Due to the nature of the intervention, participants and the yoga instructor could not be blinded to group allocation. However, to minimise bias, outcome assessment and data analysis were performed under blinded conditions. The radiologist conducting ultrasound assessments for liver fat content and the laboratory personnel analysing biochemical parameters (liver enzymes, HbA1c and lipid profile) were blinded to group allocation. In addition, the statistician responsible for data analysis was also blinded to group assignments. Group codes were concealed until the completion of the primary analysis.
Adverse Events
The Institutional Ethics Committee (IEC) was told about any unexpected or serious bad events within 48 h of them happening. If anything bad happens, participants would get medical help right away.
Analysis of Outcomes
The study conducted both intention-to-treat (ITT) and PP analyses to gain a thorough understanding of the effects of the intervention. The Shapiro–Wilk test was used to assess data normality. Continuous variables were presented as mean ± SD or median (interquartile range) if the data are not normally distributed, with comparisons made using an independent t-test or Mann–Whitney U test accordingly. Within-group comparisons of pre- and post-intervention data were conducted using paired t-tests or Wilcoxon signed-rank tests for non-normal data. Categorical data were expressed as frequencies and compared using the chi-squared test. The statisticians analysing the data were blinded to group allocations. All statistical analyses were performed using SPSS version 26.0.
Data Collection
Data were assessed at baseline and at the end of 3-month follow-up. The online yoga sessions were conducted by the first author, and participant compliance was monitored through weekly attendance records.
Discussion
This study protocol presents the first randomised controlled trial evaluating the effectiveness of a newly developed, structured online yoga module specifically designed for adults with MASLD. The novelty of this study resides in its customised integration of traditional yogic practices, encompassing asanas, pranayama, shat-karmas and meditation, presented in a feasible online format to improve accessibility and compliance. As the initial protocol for evaluating this specific module, it addresses a significant gap in present MASLD management strategies that predominantly emphasise lifestyle modification while failing to incorporate mind–body practices in a standardised, evidence-based framework.
Due to the increasing global burden of MASLD, particularly in areas such as North India, there is an urgent need for innovative interventions that provide comprehensive advantages. Yoga’s diverse effects on metabolic health, stress alleviation and psychological strength make it an optimal adjunct plan. Previous research indicates yoga’s potential advantages on liver enzymes, glycaemic management and lipid profile; but direct assessment of liver fat reduction via imaging is still limited. This trial aims to address the deficiency by using ultrasound-based quantification when combined with thorough metabolic and psychosocial assessments. The online delivery method is a strong point of this study because it overcomes the common problems like time limits and geographical limits. If it works, it could be used more widely. Strict methods like randomisation, blinded statistical analysis and both ITT and PP analyses improve the reliability and validity of the findings. Participants were advised to maintain their usual lifestyle habits throughout the study period; however, variations in diet and physical activity cannot be fully controlled. Additionally, participant adherence and external lifestyle influences may pose challenges, although compliance monitoring and objective outcome measures are expected to mitigate these concerns. Ultimately, this study wants to produce significant clinical evidence regarding the efficacy of a scientifically formulated yogic module in decreasing hepatic steatosis and enhancing cardiometabolic and psychosocial health in MASLD. Its results may facilitate incorporating yoga into standard MASLD care, impacting clinical practice, patient self-management strategies, guiding future integrative research and healthcare policy.
Conclusion
This study protocol outlines a rigorously designed randomized controlled trial to evaluate the efficacy of a structured, 60-minute online yoga intervention in individuals with metabolic dysfunction-associated steatotic liver disease (MASLD). By integrating traditional yogic practices with contemporary clinical assessment methods, the study aims to generate robust evidence on the impact of yoga on hepatic steatosis, metabolic parameters and psychosocial well-being. If proven effective, this intervention may offer a feasible, low-cost and scalable adjunct to standard care, contributing to improved clinical outcomes and holistic management of MASLD. The findings of this trial may also support the inclusion of evidence-based yoga interventions in clinical practice guidelines and inform future integrative healthcare research.
Footnotes
Acknowledgements
The authors gratefully acknowledge Shri Mahant Devendra Das Ji Maharaj, president of the Shri Guru Ram Rai University, for his invaluable guidance and support. The authors also thank Dr Lokesh Gambhir, Registrar of the University, and Dr Gaurav Raturi, Medical Superintendent of the hospital, for their support and assistance. The authors also acknowledge the use of OpenAI for assistance in improving the clarity and quality of the manuscript.
Authors’ Contributions
This study was conceptualised by GP, GS, SG and KJ. Study design was developed by GP, GS, KS and VU. Protocol implementation and strategy refinement were carried out by GP, KJ and VU. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patients and Public Involvements
Patients and/or the public are not engaged in the design, conduct, reporting or dissemination of this research.
Statement of Ethics
The Institutional Ethical Committee gave its ethical approval on 26 April 2025 with the reference number SGRR/IEC/14/25. The Clinical Trial Registry of India (CTRI/2025/05/087564) registered this trial on 23 May 2025.
Supplementary Material
Trial Registration Number
This trial is registered in the Clinical Trial Registry of India (registration number CTRI/2025/05/087564 (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.