
Abstract
Background
Trauma has a profound impact on both psychological and physiological functioning, with sleep disturbances—particularly nightmares—emerging as one of the most commonly reported symptoms. These sleep disruptions often co-occur with cognitive difficulties, affecting memory and attention.
Purpose
The present study aimed to explore the relationship between trauma history, nightmare frequency and their effects on cognitive functions such as memory and concentration among young adults aged 18–30.
Methods
A sample of 22 participants was surveyed using a structured questionnaire designed to assess trauma exposure, sleep quality, nightmare frequency and self-reported cognitive performance. Data were analysed to identify associations between trauma experiences, sleep disturbances and cognitive outcomes.
Results
Individuals with a history of trauma reported more frequent nightmares and poorer sleep quality. A notable association was observed between frequent nightmares and cognitive difficulties, particularly memory lapses and problems with concentration. Participants experiencing regular nightmares also reported higher levels of daytime impairment, indicating a link between nocturnal distress and reduced cognitive efficiency.
Conclusion
The findings highlight the significance of recognising nightmares not only as a symptom of trauma but also as a contributing factor to cognitive challenges. Integrating sleep-focused interventions into trauma-informed care may enhance cognitive well-being and overall functioning among affected individuals. This study adds to the growing evidence underscoring the interconnectedness of trauma, sleep and cognitive health.
Keywords
Introduction
Nightmares have consistently emerged as a significant symptom of post-traumatic stress, 1 through polysomnographic recordings and interviews with adults diagnosed with post-traumatic stress disorder (PTSD), identified a clear link between trauma exposure and disturbances in rapid eye movement (REM) sleep, along with frequent nightmares. Supporting this, Ohayon and Shapiro, 2 in a large-scale epidemiological study involving 13,000 adults, reported that 2%–6% of the population experience chronic nightmares, with notably higher prevalence among trauma-exposed individuals. Similarly, Marquis et al. 3 observed in a longitudinal survey of undergraduate students that those with a trauma history had elevated nightmare frequency, which later predicted issues with anxiety and attention.
Further, Lara-Carrasco et al. 4 using dream diaries from adolescents, found that trauma-related nightmares commonly featured themes of hyperarousal and helplessness, reinforcing the content-specific nature of post-traumatic dreams. They extended this understanding by highlighting gender differences through a meta-analysis, noting that women with PTSD are more likely to experience nightmares and emotional dysregulation compared to men. 5
Nightmares and Cognitive Functioning
Nightmares appear to impact cognitive performance, particularly in populations under stress or trauma. Swanson et al. 6 using cognitive testing among 204 college students, found that frequent nightmares were negatively associated with working memory capacity. A similar connection was established by Zadra and Donderi, 7 who showed that university students experiencing regular nightmares reported elevated emotional distress and reduced concentration.
Additionally, Salas et al. 8 demonstrated that trauma-exposed young adults with poor sleep quality performed worse on executive functioning and memory tasks, reinforcing the cognitive cost of disturbed sleep. From a neurobiological perspective, the impact of trauma on cognition and sleep is mediated by changes in neurotransmitter systems and brain structure. The overactivation of the hypothalamic–pituitary–adrenal (HPA) axis results in sustained cortisol release, which can damage hippocampal neurons and impair memory consolidation. Additionally, trauma affects the balance of neurotransmitters such as serotonin, norepinephrine and dopamine, all of which play critical roles in mood regulation, arousal and cognitive functioning. Functional MRI studies have shown altered connectivity between the amygdala and prefrontal cortex in trauma survivors, indicating a disruption in the brain’s ability to regulate emotional responses. These alterations are associated with increased emotional reactivity, intrusive thoughts and difficulties in concentrating, hallmarks of both PTSD and brain fog. 9
Interventions and Therapeutic Outcomes
Evidence also supports that targeting nightmares can improve psychological and cognitive functioning. Pigeon et al. 9 conducted a randomised controlled trial with veterans and found that therapeutic interventions significantly reduced nightmare frequency and enhanced cognitive performance. Krakow and Zadra 10 similarly demonstrated that imagery rehearsal therapy (IRT), a structured method to alter distressing dreams, led to improved sleep quality and decreased daytime PTSD symptoms in trauma patients. A narrative literature review proposes that nightmares act as a bridge between trauma and insomnia, making them an ideal clinical target for intervention. 11 Their findings emphasise the dual benefit of treating nightmares not only for better sleep but also for reducing trauma-related distress.
Methods
This study employed a quantitative, cross-sectional research design to examine the relationship between trauma exposure, nightmare frequency and cognitive functioning among young adults. The study relied on standardised psychological assessment tools and statistical analyses to investigate associations between trauma history, sleep disturbances and self-reported cognitive difficulties.
The research focused on identifying correlations and predictive relationships between these variables using descriptive statistics, correlation analysis, regression models and analysis of variance (ANOVA). This quantitative approach allowed for systematic measurement of trauma exposure, sleep quality, nightmare frequency and cognitive functioning within the study sample.
Participants
A total of 22 participants (N = 22) were recruited for this study using purposive sampling. All participants fall within the age range of 18–30 years, aligning with developmental research indicating heightened vulnerability to trauma and cognitive plasticity during this life stage.
Inclusion Criteria
Self-reported history of trauma (as determined by the Life Events Checklist-5).
Age between 18 and 30 years.
Speaking English and being able to give informed consent.
Having at least one nightmare a week for the previous month.
Criteria for Exclusion
Current use of sedatives or antipsychotics; neurological illnesses (such as epilepsy or brain injury); active substance abuse; and sleep disorders other than nightmare disorder (such as sleep apnoea).
Data Collection
Flyers, student health services and online university platforms were used to recruit participants. Each participant receives a small compensation for taking part using the following standardised tools, and quantitative data were gathered:
The purpose of the Life Events Checklist-5 (LEC-5) is to evaluate exposure to potentially traumatic situations. The Clinical-Administered PTSD Scale (CAPS-5) is a structured diagnostic interview used to assess the severity of PTSD. Pittsburgh Sleep Quality Index (PSQI): to evaluate sleep disruptions and quality. The NFQ is a self-report tool used to gauge the frequency and severity of nightmares. The short cognitive screening test known as the Montreal Cognitive Assessment (MoCA) evaluates executive function, memory, attention and processing speed. Forward and backward digit span: Used to evaluate working memory. To account for mood as a confounding variable, use the Beck Anxiety Inventory (BAI) and the Beck Depression Inventory-II (BDI-II).
Results
Demographic Details
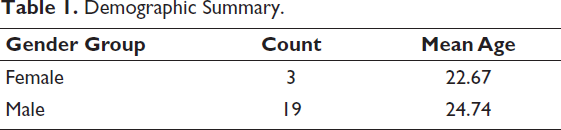
The study involved young adults between the ages of 18 and 30. The demographic distribution of participants based on gender and age is summarised below in Table 1.
Demographic Summary.
Descriptive Statistics
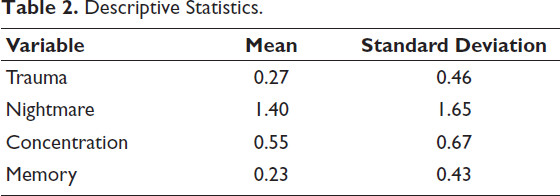
Descriptive statistics were computed to assess the levels of trauma, nightmare frequency and cognitive impact among young adults in Table 2.
Descriptive Statistics.
Correlation Analysis
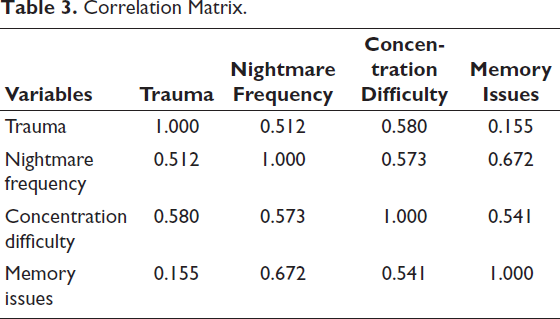
The correlation matrix below illustrates the relationships between trauma, nightmares and cognitive impact variables. A moderate to strong positive correlation was found between trauma history and nightmare frequency (r = 0.51), as well as between trauma and concentration difficulties (r = 0.58). Nightmare frequency showed strong associations with both memory issues (r = 0.67) and concentration difficulties (r = 0.57), suggesting cognitive disruption in individuals experiencing frequent nightmares.
Pearson correlation was conducted to examine the relationships between trauma, nightmare frequency and cognitive impairment indicators. The result is shown in Table 3.
Correlation Matrix.
Regression Analysis
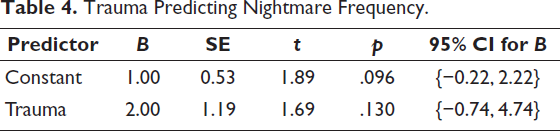
To further explore the impact of trauma and nightmares on cognitive impairment, regression analysis was conducted and is shown in Table 4.
Trauma Predicting Nightmare Frequency.
Model Summary
R² = 0.262, Adjusted R² = 0.170, F(1, 8) = 2.84, p = .130 and it is shown in Tables 5 and 6.
Model 2: Nightmare Frequency Predicting Concentration Difficulty.
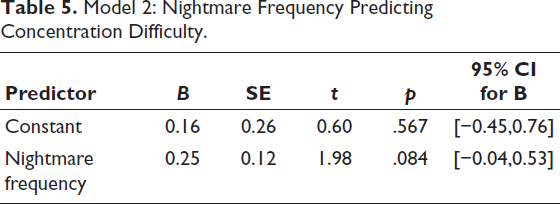
Model Summary
R² = 0.328, Adjusted R² = 0.244, F(1, 8) = 3.90, p = .084.
Trauma and Nightmare Frequency Predicting Concentration Difficulty.
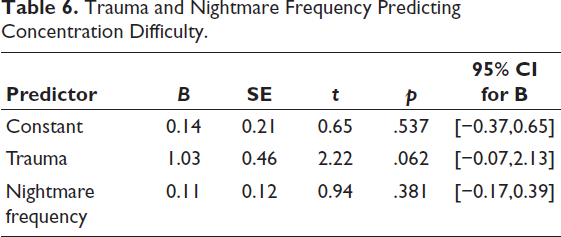
Model Summary
R² = 0.605, Adjusted R² = 0.492, F(2, 7) = 5.36, p = .039.
These findings may tentatively suggest that trauma and nightmare frequency together contribute to concentration difficulties. However, given that some predictors did not reach conventional levels of statistical significance, these relationships should be interpreted as preliminary trends rather than definitive effects.
ANOVA Analysis
To determine whether there is a significant difference in memory problems between participants with and without a trauma history, a one-way ANOVA was conducted. This test assesses whether trauma status has a statistically significant effect on reported memory issues, and it is shown in Table 7.
One-way Analysis of Variance (ANOVA)—Trauma and Memory Issues.
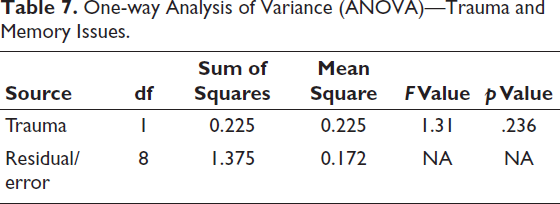
The ANOVA results indicated that the effect of trauma on memory issues was not statistically significant, F(1, 8) = 1.31, p = .286. This suggests that there was no meaningful difference in memory problems between individuals with a trauma history and those without in this sample. While memory impairment was observed across the sample, trauma did not appear to be a significant differentiating factor in this specific aspect of cognitive functioning.
ANOVA: Impact of Trauma on Memory
To evaluate whether a history of trauma significantly influences memory issues among young adults, a one-way ANOVA was conducted and is shown in Table 8.
Analysis of Variance (ANOVA) Summary—Trauma and Memory Issues.
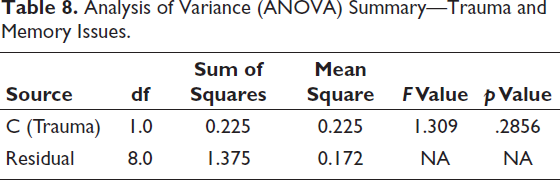
The ANOVA results indicate that there was no statistically significant effect of trauma history on memory issues (F(1, 8) = 1.31, p = .2856). This suggests that while there may be differences in memory problems among individuals with and without trauma, these differences were not statistically significant.
Discussion
The present study examined the relationships between trauma exposure, nightmare frequency and cognitive functioning among young adults aged 18–30 years. Specifically, the study aimed to investigate whether individuals with a history of trauma and frequent nightmares experience greater cognitive difficulties, particularly in the domains of memory and concentration. Using quantitative statistical analyses, including descriptive statistics, correlation analysis, regression models and ANOVA, the study explored potential associations between trauma-related experiences and cognitive functioning. Overall, the findings provide preliminary evidence suggesting that trauma exposure and sleep disturbances—particularly nightmares—may be associated with perceived cognitive difficulties among young adults.
The correlation analysis revealed moderate associations between trauma exposure and nightmare frequency, as well as between trauma exposure and concentration difficulties. Participants who reported a history of trauma tended to report more frequent nightmares and greater challenges maintaining concentration during daily activities. These findings are consistent with existing literature demonstrating that trauma exposure is frequently associated with disturbances in sleep patterns, particularly disruptions in REM sleep, which is closely linked to dream activity and emotional memory processing.12, 13 Disturbances in REM sleep are often observed among individuals exposed to traumatic experiences and have been associated with the occurrence of recurrent nightmares and emotional dysregulation.14, 15
In addition to the relationship between trauma and nightmares, the results indicated that nightmare frequency was moderately associated with both concentration difficulties and self-reported memory problems. Participants who experienced more frequent nightmares also reported greater cognitive challenges, particularly with sustaining attention and recalling information. Although these findings cannot establish causal relationships, they are consistent with previous studies suggesting that sleep disturbances may negatively influence cognitive functioning. Sleep plays a crucial role in memory consolidation and attentional regulation, and disruptions in sleep continuity can impair executive functioning and cognitive efficiency.16, 17 Frequent nightmares may interrupt sleep cycles, leading to fragmented sleep and daytime fatigue, which can in turn reduce cognitive performance.
The regression analyses provided further insight into the relationships between trauma exposure, nightmares and cognitive difficulties. The first regression model examined whether trauma exposure predicted nightmare frequency. Although the analysis revealed a positive relationship between trauma history and the frequency of nightmares, the effect did not reach conventional levels of statistical significance. This result should therefore be interpreted cautiously. The absence of statistical significance may be attributable to the limited sample size of the study, which reduces statistical power and the ability to detect small to moderate effects. Nevertheless, the direction of the relationship is consistent with prior research demonstrating that individuals with trauma histories are more likely to experience persistent nightmares and sleep disturbances.1, 2
The second regression model examined whether nightmare frequency predicted concentration difficulties. The findings suggested a potential association between more frequent nightmares and increased concentration problems; however, this effect approached but did not reach statistical significance. Although the results cannot be interpreted as conclusive, they may indicate a trend that warrants further investigation. Previous research has shown that disrupted sleep and recurring nightmares can negatively affect attentional processes and cognitive performance, particularly among individuals exposed to psychological stress or trauma.6, 8 Frequent nocturnal awakenings and emotional distress associated with nightmares may reduce the restorative quality of sleep, leading to impaired daytime cognitive functioning.
The third regression model examined the combined effects of trauma exposure and nightmare frequency on concentration difficulties. This model was statistically significant overall, suggesting that trauma and nightmares together may explain a portion of the variance in concentration problems reported by participants. Within this model, trauma exposure demonstrated a stronger association with concentration difficulties than nightmare frequency alone. This finding may indicate that trauma-related psychological processes—such as heightened physiological arousal, intrusive memories and emotional dysregulation—may influence cognitive functioning independently of sleep disturbances.18, 19 Trauma exposure has been associated with dysregulation of the HPA axis and prolonged cortisol release, which may impair hippocampal functioning and affect cognitive processes such as memory consolidation and attentional control. 19
The analysis examining memory problems produced somewhat different results. The one-way ANOVA conducted to assess whether trauma exposure was associated with memory difficulties did not reveal a statistically significant difference between participants with and without trauma histories. This finding suggests that trauma exposure may not have been a strong differentiating factor for self-reported memory difficulties within this sample. Several explanations may account for this outcome. First, memory functioning is influenced by a wide range of psychological and physiological factors, including stress levels, emotional regulation and sleep quality. 20 Second, the measurement of memory difficulties relied partly on self-reported perceptions rather than comprehensive objective neuropsychological testing. Self-reported cognitive complaints may not always correspond directly with measurable cognitive impairment.
The descriptive findings also provide additional context for interpreting the results. The sample consisted predominantly of male participants, with only a small proportion of female participants. Participants reported experiencing nightmares approximately once or twice per week on average, indicating that sleep disturbances were relatively common within the sample. Additionally, concentration difficulties were reported more frequently than memory problems. This pattern may reflect the immediate cognitive effects of sleep disruption, which often manifest as reduced attentional capacity, mental fatigue and decreased alertness rather than clear memory deficits.16, 21
Several limitations should be considered when interpreting the findings of this study. First, the relatively small sample size (N = 22) limits statistical power and restricts the generalisability of the results. Small samples increase the likelihood that potentially meaningful relationships may not reach statistical significance. Second, the gender distribution of participants was uneven, with a predominance of male participants. This imbalance limits the ability to examine potential gender differences in trauma exposure, nightmare frequency and cognitive functioning. Previous research suggests that women may experience trauma-related sleep disturbances at different rates than men, highlighting the importance of gender-balanced samples in future studies. 5 Third, some measures of cognitive functioning relied on self-reported experiences rather than comprehensive objective cognitive assessments.
Despite these limitations, the study contributes to the growing body of research examining the interconnections between trauma, sleep disturbances and cognitive functioning. The findings highlight the potential role of nightmares as a factor associated with cognitive difficulties among young adults. Sleep disturbances are frequently overlooked in trauma-focused clinical assessments, yet they may represent an important pathway through which trauma-related stress affects cognitive performance and daily functioning. 11
Future research should expand upon these findings by employing larger and more diverse samples, incorporating objective sleep measures such as actigraphy or polysomnography and utilising comprehensive neuropsychological tests to assess cognitive functioning more accurately. Longitudinal studies would also be valuable in clarifying the temporal relationships between trauma exposure, sleep disturbances and cognitive outcomes. Such research could help determine whether interventions targeting nightmares and sleep quality may improve cognitive functioning among trauma-exposed individuals.
In conclusion, the present study provides preliminary evidence suggesting that trauma exposure and nightmare frequency may be associated with cognitive difficulties—particularly in the domain of concentration—among young adults. Although several findings did not reach statistical significance, the observed patterns highlight the potential importance of sleep disturbances in understanding trauma-related cognitive challenges. Addressing nightmares and sleep quality may therefore represent an important component of comprehensive trauma-informed care aimed at improving cognitive well-being and daily functioning.
Conclusion
This study explored the complex relationships between trauma history, sleep disturbances—specifically nightmares—and cognitive difficulties such as memory loss and concentration problems in young adults aged 18–30. Using quantitative methods, including correlation, regression and ANOVA, the study aimed to uncover how past traumatic experiences and poor sleep quality contribute to cognitive functioning.
The findings suggest that trauma and nightmares are significantly related to cognitive impairment. Trauma was moderately associated with increased nightmare frequency and difficulty concentrating, while frequent nightmares were strongly associated with both memory and concentration problems. Although not all regression models reached statistical significance, patterns in the data consistently pointed toward a meaningful relationship between these psychological and cognitive variables.
The final regression model, which included both trauma and nightmares predicting concentration difficulty, was statistically significant, highlighting how trauma may indirectly affect cognitive performance through sleep disturbances. While the one-way ANOVA examining trauma’s impact on memory did not show a significant effect, this may be due to the small sample size or variability in individual memory resilience.
In conclusion, the results support the notion that unresolved trauma and frequent nightmares can significantly interfere with cognitive functioning in young adults. These findings underscore the need for psychological interventions that not only address trauma directly but also incorporate sleep-focused treatments. Improving sleep quality—particularly by addressing nightmares—may serve as a vital pathway for enhancing cognitive health and daily functioning in trauma-affected individuals.
Implications of the Study
The study has important clinical relevance, especially for mental health professionals working with trauma survivors. First, it emphasises the importance of screening for nightmares and sleep disturbances as part of trauma assessments. Frequently, therapeutic focus remains centred on emotional symptoms (e.g., anxiety, depression), while cognitive impacts such as forgetfulness, attention difficulties and mental fatigue are overlooked.
Integrating sleep-focused interventions, such as IRT or cognitive behavioural therapy for insomnia (CBT-I), may reduce nightmare frequency and improve both psychological and cognitive functioning. These approaches can help reframe distressing dream content, regulate sleep cycles and restore memory and attentional control.
Additionally, including cognitive rehabilitation strategies in therapy for trauma survivors—such as working memory training or mindfulness-based attention retraining—could support cognitive recovery alongside emotional healing.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the small sample size (N = 22) reduces statistical power and limits the generalisability of the results. Some analyses approached statistical significance but did not meet conventional thresholds, which may partly reflect insufficient statistical power.
Second, the gender distribution was highly imbalanced, with the majority of participants being male (19 males and 3 females). This imbalance restricts the ability to examine potential gender differences in trauma exposure, nightmare frequency and cognitive functioning.
Third, cognitive functioning was assessed partly through self-reported measures, which may be influenced by subjective perception and mood states.
Finally, although the study incorporated qualitative data through interviews and sleep diaries, these data were used primarily to contextualise the quantitative findings and were not analysed through a formal qualitative framework. Future studies employing larger samples and comprehensive mixed-method analyses would provide a more robust understanding of the relationship between trauma, nightmares and cognitive functioning.
Footnotes
Authors’ Contribution
Saranya TS—Conceptualisation, study design, data analysis, manuscript writing and overall supervision of the study.
Sera Mary Soloman—Data collection, questionnaire administration and preliminary data interpretation.
Sandeep Kumar Gupta—Methodological guidance, statistical validation and critical revision of the manuscript for intellectual content.
Sebnem Yucel—Theoretical framing, literature review support and review of cross-cultural aspects related to trauma and sleep.
Recep Yucel—Data interpretation, technical review and final proofreading of the manuscript prior to submission.
All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was collected from all the participants after ensuring confidentiality.
Statement of Ethics
The study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. Ethical approval for this research was obtained from the Institutional Ethics Committee of the host institution. All participants were informed about the purpose and procedures of the study and provided written informed consent prior to participation. Confidentiality and anonymity of participants were strictly maintained throughout the research process. No potential harm or discomfort was inflicted upon participants, and they were free to withdraw from the study at any point without penalty.