
Abstract
Background
Neuropsychological functioning, metacognitive awareness and mindfulness are central to self-regulatory processes operating across cognitive and affective domains. Although global research on these constructs has increased, integrated evidence from non-Western contexts, particularly India, remains limited.
Purpose
The purpose of this study was to assess and compare neuropsychological functioning, metacognitive awareness and mindfulness in adult Indian men diagnosed with opioid dependence (OD) and healthy male controls. The study also examined the relationships among these constructs within the OD group.
Methods
A total of 200 adult men aged 25–45 years (mean age = 35 years, SD = 5) participated in the study. The sample included 100 participants diagnosed with OD according to International Classification of Diseases-11 (ICD-11) criteria and 100 healthy controls without a history of substance use disorders. Standardised instruments were used to assess neuropsychological functioning, metacognition and mindfulness. Group differences were analysed using multivariate analysis of variance (MANOVA) with Bonferroni-corrected univariate analyses. Correlation and multiple regression analyses were conducted within the OD group while controlling for demographic variables.
Results
Men with OD demonstrated significantly poorer neuropsychological functioning, lower metacognitive awareness and reduced mindfulness compared to controls (all p < .05). Within the OD group, both mindfulness and metacognitive awareness showed positive correlations with neuropsychological functioning. After adjusting for demographic factors, metacognitive awareness exhibited a stronger association with neuropsychological functioning than mindfulness.
Conclusion
The findings indicate pronounced self-regulatory deficits in individuals with OD. The results support the inclusion of metacognitive and mindfulness-based components in assessment and rehabilitation programmes, particularly within South Asian cultural contexts.
Neuropsychological Functioning
The delayed-recall and visual-memory scores of methadone or buprenorphine users were lower than those of healthy subjects, and thus may be attributed to abnormalities in white matter tracts across frontal-temporal regions and dopamine-driven working memory (WM) circuits. 1 Research from India found that male subjects using opioids, whether alone or concurrently with cannabis, demonstrated increased error rates on verbal 2-back and visual 1-back tasks, suggesting early visual WM dysfunction. 2 These cognitive deficits, which include attention, memory and executive function, are stable throughout long periods of abstinence, and are likely to continue even during periods of active buprenorphine–naloxone treatment.3, 4 Similarly, a recent systematic review noted that chronic or high-dose opioid use was significantly related to impairments in verbal episodic and visuospatial memory. 5 Based on this body of literature, it appears essential to develop culturally appropriate neurocognitive assessments to assess opioid-dependent Indian populations.
Metacognition
A metacognitive skill is a more advanced cognitive skill in that individuals assess the quality of their own thinking, are able to monitor the amount of mental effort required to complete a task, and are able to modify their approach to a task based on prior experience. 6 There are two related components of metacognition: metacognitive knowledge, which is the knowledge an individual’s cognitive strengths and weaknesses, as well as knowledge of problem-solving strategies and methods; and metacognitive regulation, which is the ability to formulate plans, monitor progress and evaluate the outcomes of the thinking and behaviour involved in completing a task.7, 8
Individuals who suffer from substance dependence (SU) have consistently been found to possess metacognitive impairments that contribute to reduced self-awareness, increased impulsiveness and less effective decision-making.9, 10 These metacognitive deficits can serve to exacerbate drug-seeking behaviours by reducing an individual’s ability to predict the negative consequences of engaging in drug-seeking, to employ alternative, adaptive coping strategies to manage cravings and to substitute maladaptive thought patterns with adaptive ones. 11 Metacognitive therapy (MCT) has emerged as a treatment for the metacognitive deficits that develop in response to these deficits. The focus of MCT is to help individuals to be able to identify and change their maladaptive beliefs about their abilities to think and manage their own cognitive processes.12, 13
To date, however, the majority of metacognition in addiction research has been performed in Western populations and as a result, there is limited understanding of the impact of the cultural environment on cognitive dysfunctions.
Mindfulness
Mindfulness, as defined by Kabat-Zinn,14, 15 requires the active practice of being focused on the current moment while maintaining an openness and curiosity regarding what is happening at the moment, including a non-judgemental acceptance of one’s experience in the present moment. Individuals can cultivate this ability by practising observing their thoughts, physical feelings and emotions as they occur; it does not require suppressing these experiences or avoiding them, nor becoming overly preoccupied with them. MCT ultimately promotes greater emotional stability and enhances cognitive flexibility, thus enabling individuals to maintain their attention and respond to life events more effectively.16–19
According to a cognitive science view of mindfulness, it facilitates a meta-cognitive mode of awareness where individuals perceive mental events as transitory rather than permanent.20, 21 This transformation reduces ruminative tendencies, promotes emotional balance and interrupts the habitual behavioural responses typical of addiction. Mindfulness-based interventions have demonstrated effectiveness in reducing relapse risk, decreasing reactivity to cravings and improving general well-being among opioid dependence (OD) populations.22–24 Although mindfulness has origins in South Asian traditions, there is a paucity of research investigating its application within clinical contexts in India, therefore the extent to which cultural familiarity influences the use of mindfulness in this population is unknown.
Interaction of Mindfulness and Metacognition
In addition to problems with sustained attention, WM, impulse control and planning/organisation of behaviour, individuals diagnosed with OD have been shown to experience metacognitive deficits, primarily the inability to monitor and evaluate their own thinking.25, 26 As described above, when an individual is unable to monitor their own thinking, they may be unaware of maladaptive thought patterns, utilise fewer coping mechanisms, and be at greater risk of relapse.10, 27
Evidence continues to emerge indicating that cognition and metacognition are highly interdependent and do not occur independently of one another. While learning to maintain attention on one’s thoughts in a consistent and deliberate manner may allow individuals to become more cognisant of how their thoughts arise, this will foster more thoughtful monitoring and regulation of mental processes.28, 29 However, deficits in either of these domains can further strengthen maladaptive cognitive/emotional cycles that encourage continued substance use.20, 21 Therefore, integrated approaches (such as combining mindfulness-based relapse prevention [MBRP] with MCT) that target both domains have been promising in improving emotional regulation, cognitive control and relapse prevention.30, 50 However, despite increasing interest in these areas, virtually nothing is known about how mindfulness, metacognition and cognitive abilities interact within non-Western cultural environments.
Cultural Context and Research Gap
Recent studies in a sample of Indians who suffer from OD revealed that there were significant problems with sustaining attention and performing on WM for those men, thus indicating that the social and cultural context (and the expectation of men in their families) could contribute as much as biological and neurological factors to the problems men experience with cognitive processing. 31 Most of the literature that is currently available on mindfulness, metacognition and cognition in populations that use substances has been done in Western countries, typically included both genders, was with adolescent participants, or was based on a treatment-seeking population. The limitations of using such a narrow demographic when drawing conclusions about populations from different cultures cannot be overstated.
Verbal and visual memory do not develop independently of one another; they are developed in relation to the cultural environment in which people live. Strong family bonds, marital obligations and the pressures associated with masculinity in South Asian societies create many constraints on the individual’s ability to maintain emotional balance, and consequently, impact mindfulness and metacognitive development.32, 33
Men with OD in India have been shown to have marked deficits in verbal and visual memory, as indicated by impaired performance on N-back tasks and episodic recall. 2 Furthermore, longitudinal data have demonstrated slow or no recovery of memory functioning despite abstinence.3, 4 Comparable deficits in memory functioning have been reported in several other countries, with individuals suffering from OD demonstrating impairments in delayed verbal recall and visuospatial memory. 1 However, the majority of this evidence has come from health systems and cultural contexts which are vastly different from the Indian culture. To date, no studies have investigated the relationship between mindfulness, metacognition and verbal/visual memory functioning in adult Indian men with OD, despite the fact that cultural expectations, family structures, stigma and gender-related pressures all play significant roles in the cognitive functioning of men with OD.
Unique Contribution of the Present Study
Although mindfulness and metacognition both involve awareness and regulation of internal experience, their interaction in OD has rarely been examined. 34 Most existing evidence comes from Western settings with samples that vary widely in gender, marital status, socio-economic background and culture. Such findings cannot be assumed to generalise to other populations, as cognitive functioning, recovery processes and treatment engagement are closely shaped by the sociocultural context. 36 There is also growing recognition that verbal and visual memory performance varies across cultures, and recent studies suggest that opioid-related memory deficits may present differently across societies.1, 2
In South Asian contexts, including India, culturally defined expectations around masculinity, financial responsibility and family stability place substantial emotional demands on men. These pressures may increase psychological vulnerability and have been linked to lower mindfulness and weaker metacognitive control in individuals with OD.32, 33 Indian studies further show that men with OD exhibit marked impairments in both verbal and visual WM, reflected in higher error rates on verbal 2-back and visual 1-back tasks, with many deficits persisting even after abstinence or treatment completion.3, 4 Together, these observations point to the importance of studying memory alongside higher-order cognitive capacities such as mindfulness and metacognition within the Indian cultural context.
Most prior research has examined mindfulness, metacognition or memory in isolation. Assessing these constructs simultaneously allows for a more integrated understanding of cognitive functioning in Indian men with opioid use disorder (OUD) and how attentional regulation, self-monitoring and memory performance may co-occur. Adult Indian men are frequently represented in treatment settings yet remain underrepresented in empirical research, limiting culturally informed interpretation of cognitive vulnerability. Examining this group provides insight into how cultural norms, family structure, stigma and gender expectations relate to cognitive and metacognitive functioning.
Finally, the use of cross-culturally validated measures such as the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R), Metacognitive Awareness Inventory (MAI) and standardised memory tasks enable comparison with international findings and supports a culturally grounded investigation of cognitive vulnerability in OD.
Rationale of the Study
OD is associated with substantial cognitive difficulties, including reduced mindfulness, lower metacognitive awareness and impairments in both verbal and visual memory. Mindfulness and memory are core cognitive functions that support emotional regulation, learning, decision-making and behavioural flexibility.36, 37 When an individual’s metacognitive and mindfulness capabilities are impacted by substance use, they will be unable to recognise maladaptive thought processes, successfully manage their cravings for substances, and become actively engaged in their treatment plan. The metacognitive process refers to an individual’s self-awareness as well as their ability to evaluate, regulate and direct their thoughts. Mindfulness is an attentiveness to the present that is non-judgemental; when either capacity is compromised, an individual has difficulty in identifying maladaptive thought processes and coping with the drive to consume drugs.
Individuals with OD also show marked impairments in verbal and visual memory compared to healthy controls, including poorer delayed recall and higher error rates on N-back tasks. Such memory deficits may further compromise metacognitive monitoring and reduce the cognitive resources needed to engage effectively in mindfulness-related processes.
The present research examines the correlation among mindfulness, metacognition and memory functioning in adult men with OD in comparison with healthy controls, with the aim of clarifying how these cognitive processes interact and contribute to the overall cognitive profile of this population.
Methods
Objectives of the Study
To compare verbal and visual WM, metacognition and mindfulness between men with opioid dependence and healthy controls.
To examine associations among WM, metacognition and mindfulness within the opioid-dependence group.
To determine whether metacognition and mindfulness predict WM performance after controlling for demographic variables.
Design of Research
The study employed a cross-sectional comparative design in which men with OD were compared with healthy controls. Although the groups were broadly age-matched, differences in education, occupation, family income and family structure were observed and were therefore treated as potential confounders in subsequent analyses.
Sampling Technique: Purposive
Sample Size
The sample comprised 200 adult men, including 100 individuals diagnosed with OD according to International Classification of Diseases-11 (ICD-11) criteria, and 100 healthy controls with no history of SU. Participants in both groups were aged 21–45 years, able to communicate in Hindi or English, and provided informed consent. Individuals with co-occurring mental disorders or serious medical conditions were excluded from both groups.
Tools to be Used
Four standardised assessment tools were employed in the study to measure emotional distress, mindfulness, metacognitive functioning and WM. The General Health Questionnaire (GHQ-28) is a 28-item screening tool designed to evaluate emotional distress and risk for psychiatric disorders. 38 The CAMS-R was used to assess mindfulness. 39 MAI was used to assess Metacognitive Awareness, which evaluates both cognitive knowledge and regulation of cognition, including planning, monitoring, evaluating, debugging and managing information. 7 Verbal and visual WM were examined using the N-back test, 41 with scoring based on the number of hits and errors, where omissions and commissions constitute total errors. The test duration was 12 min.
Procedure
Participants progressed through this study as depicted in Figure 1. A total of 215 individuals were assessed for eligibility. After applying inclusion and exclusion criteria, 200 participants were enrolled, including 100 men with OD and 100 healthy controls. Missing data were minimal (<5%), and cases with incomplete responses were excluded from final analyses.
Participant Recruitment, Exclusion and Inclusion in the Final Analysis.
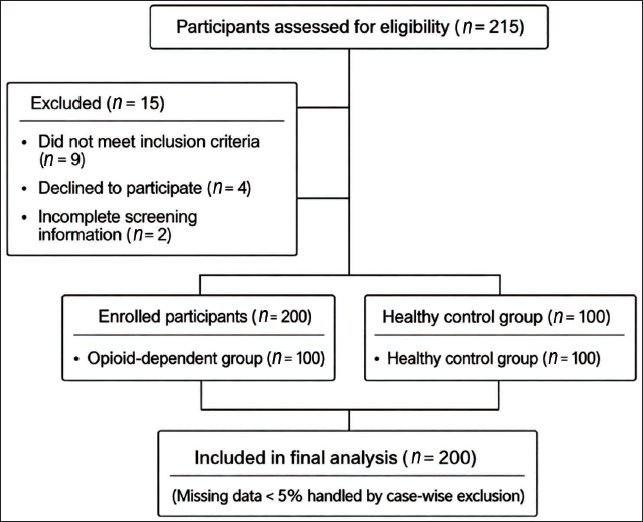
Ethical approval for the study was granted by the institutional research and ethics committee. A total of 200 adult men participated, including 100 individuals diagnosed with OUD (ICD-11) and 100 age-matched healthy controls with no substance use history. After applying the inclusion and exclusion criteria, written informed consent was obtained. Socio-demographic and clinical information were collected through a semi-structured proforma, and the GHQ-28 (cut-off: 23) was used to screen for psychiatric morbidity. Participants who met the criteria completed standardised measures: the MAI for metacognition, the CAMS-R for mindfulness, and verbal (2-back) and visual (1-back) N-back tasks to assess WM accuracy and errors. These tasks provided sensitive indicators of verbal and visuospatial memory functioning.
Data from the study were analysed using Statistical Package for the Social Sciences (SPSS) version 23. Descriptive statistics were applied to summarise the characteristics of the participants. Independent t-tests along with appropriate multivariate statistical techniques were utilised to examine differences between the OD and healthy control groups for measures of mindfulness, metacognition and neurocognitive function. Statistical analysis of correlations and regression was used to examine the relationship between mindfulness, metacognition and neurocognitive function among the OD group. To address group differences in socio-demographic characteristics, age, education, occupation, family income and locality were entered as covariates in hierarchical regression models. These variables were included in the first step, after that, mindfulness and metacognition in the second step to examine their unique contribution to neuropsychological functioning after controlling for potential confounders. This approach was adopted to minimise the influence of socio-demographic confounding and to strengthen the interpretability of cognitive predictors.
Missing Data Handling
Participants who failed to complete their responses for the primary assessment scales were excluded from the final data analysis. The number of such cases was small, accounting for fewer than 5% of the total sample.
Results
Table 1 displays demographic information for both OD and healthy control subjects. The OD group was found to be significantly younger than the control group, t = −3.18, p < .001. All participants in both groups were male and married. Significant group differences were observed in education (χ2(5) = 46.12, p < .001), occupation (χ2(1) = 51.61, p < .001), family income (χ2(2) = 32.87, p < .001), religion (χ2(3) = 29.44, p < .001) and family structure (χ2(2) = 79.86, p < .001). In contrast, locality distribution did not have a significant difference between the groups (χ2(1) = 0.14, p = .71).
Comparison of Socio-demographic Characteristics Between Individuals with Opioid Dependence and Healthy Controls (N = 200).

This study is one of the first to examine mindfulness and metacognition together in individuals with OD, and the first, based on current literature, to do so among adult men in India.
Table 2 compares metacognitive awareness between participants with OD and healthy controls across all MAI domains. The OD group scored significantly lower than controls on declarative, procedural and conditional knowledge, as well as on all metacognitive regulation and its components (all p < .001). The magnitude of these differences was large across domains, with Cohen’s d values indicating very strong effects. Overall metacognitive awareness (MAI total score) was substantially reduced in the opioid-dependence group compared to healthy controls, reflecting pronounced impairments in both of cognition knowledge and cognitive regulation processes among OD individuals.
Metacognitive Awareness in Opioid Dependence Versus Healthy Control Group (N = 200).

Table 3 shows that participants with OD made significantly more errors than healthy controls on both verbal and visual N-back tasks (p < .001), indicating poorer WM performance. The group differences were large in magnitude, as reflected by Cohen’s d, and fall within statistically plausible and clinically interpretable ranges.
Comparison of Verbal and Visual N-back Performance Between Opioid Dependence and Healthy Control Groups (N = 200).

Table 4 shows positive associations among WM performance, metacognitive awareness and mindfulness in the healthy control group. Both verbal and visual N-back performance were moderately correlated with metacognition and mindfulness, indicating better WM accuracy with higher cognitive self-awareness. A strong correlation was observed between metacognition and mindfulness, reflecting related but distinct aspects of cognitive self-regulation. All correlations are unadjusted bivariate estimates.
Pearson Correlations Between Neuropsychological Functioning, Metacognition and Mindfulness Among Males Without Substance Use (N = 100).

Given the high correlation between mindfulness and metacognition, multicollinearity was examined prior to regression analyses. The tolerance values obtained were all well within the acceptable range, as were the variance inflation factors (VIFs), which ranged from 0.00 to 0.51 (all <1.0), thus ruling out multicollinearity as an issue in our model.
As shown in Table 5, hierarchical regression was employed to assess if there existed relationships between metacognitive and mindful processes and verbal WM performance in individuals with OD, when controlling for demographic variables. In Step 1, demographic factors accounted for a small proportion of variance in verbal N-back error scores (R2 = 0.014).
Hierarchical Multiple Regression Predicting Verbal Working-memory Performance (Verbal N-back Error Scores) in the Opioid-dependence Group (n = 100).

The addition of metacognition and mindfulness in Step 2 resulted in a substantial and statistically significant increase in explained variance (R2 = 0.499; ∇R2 = 0.485; F change = 44.06, p < .001). In the final model, metacognitive awareness (MAI total score) was significantly associated with verbal WM performance (B = 0.199, p < .001). Mindfulness (CAMS-R) also showed a significant independent association (B = 0.031, p = .032).
Table 6 shows that demographic factors (age, education, income, occupation, locality) did not predict visual N-back performance, indicating that visual WM deficits in individuals with OD are not shaped by basic socio-demographic differences. Metacognition emerged as a powerful predictor of visual WM performance (B = 0.196, p < .001), underscoring the value of skills such as planning, monitoring and evaluating strategies when completing visual memory tasks. Mindfulness (CAMS-R) also significantly predicted visual WM performance (B = 0.028, p = .032). This aligns with evidence that mindfulness promotes attentional stability, reduces cognitive interference and enhances present-moment awareness, all of which contribute to improved WM outcomes.
Multiple Regression Analysis Predicting Visual N-back Performance in the Opioid Dependence Group.

Discussion
Despite being highly represented in treatment services across South Asia, this population remains underrepresented in global addiction research.32, 33, 35 In the present study, men with OD showed substantially lower levels of metacognitive awareness and mindfulness compared to healthy controls, with large effect sizes indicating pronounced deficits across these domains. The very strong association observed between mindfulness and metacognition (r = 0.923) suggests that these constructs are closely linked and may operate together in supporting cognitive and emotional regulation.28, 29
Better WM performance was consistently associated with higher levels of both metacognitive awareness and mindfulness. Similar patterns were observed for verbal and visual WM, indicating that effective self-monitoring of thoughts and regulation of attention are closely related to performance on cognitively demanding tasks.42, 44 These findings align with existing evidence that WM efficiency depends heavily on executive processes such as attentional control, flexible allocation of cognitive resources and monitoring of ongoing performance.37, 43, 74 Previous studies have identified correlations between mindfulness and improved sustained focus (i.e., less distractions from cognitive interference), and both factors may be associated with WM performance.45, 46
The strong relationship between mindfulness and metacognition further supports theoretical models that conceptualise mindfulness as a form of metacognitive awareness, characterised by clear observation of internal experiences with reduced reactivity.28, 29 Previous studies have similarly linked mindfulness with enhanced cognitive monitoring, planning and reflective awareness, all of which are central components of metacognitive functioning.20, 21 Together, these processes have been associated with adaptive self-regulation and executive functioning in both clinical and non-clinical populations.23, 47
Regression analyses indicated that demographic and socio-economic variables accounted for minimal variance in verbal and visual WM performance, a pattern consistent with earlier findings suggesting that opioid-related cognitive impairments are relatively independent of age and socio-economic status.48, 49 In contrast, the combination of metacognitive awareness and mindfulness accounted for a significant amount of variance in WM performance. This pattern is consistent with prior work highlighting the importance of executive and self-regulatory processes, particularly metacognitive monitoring, in supporting efficient WM functioning.8, 50 Consistent with previous findings, participants reporting using planning, monitoring and evaluation strategies to control their learning processes performed better than those who did not report using such strategies, as evidenced by increased accuracy and speed when performing N-back tasks; both are indicative of successful metacognitive regulation during high-cognitive-load tasks. 50
Metacognition proved to be an important factor in predicting both WM (verbal and visual) performance; this suggests that the ability to monitor one’s own thought process has significant implications for WM (i.e., attention and memory updating). These findings are supported by other researchers who have demonstrated that many individuals with substance dependency experience impairments in metacognitive regulatory abilities; therefore, these individuals often exhibit deficits in their executive functioning capabilities and their ability to cognitively adapt.10, 11 Mindfulness has also been shown to demonstrate separate correlations with WM performance and thus support the idea that improved attentional stability and decreased cognitive interference lead to improved cognitive function.37, 51, 52
Similar results were found in the sample of healthy controls. In the sample of healthy controls, metacognitive abilities, as well as other cognitive-related variables (e.g., age, education level), showed significant associations with WM performance. No significant association was found with demographic-related variables (e.g., gender, ethnicity). Metacognitive abilities and other cognitive-related variables have also been shown in previous studies to be positively related to both executive functioning and the updating of information in memory.54–56 Separate positive correlations were found between mindfulness and visual WM performance. Neurocognitive studies, which show that mindfulness is positively related to increased activation in both attentional and executive neural networks involved in visuospatial processing, provide a basis for understanding why this correlation exists.37, 57
When taken collectively, the results suggest that mindfulness and metacognition show consistent associations with WM performance in both clinical and non-clinical populations. Although these two processes are closely related, they appear to make separate contributions to cognitive-related functioning, including executive functioning.28, 29 Importantly, given the cross-sectional design, these relationships should be interpreted as associative rather than causal. The observed patterns highlight the value of examining mindfulness and metacognition in future longitudinal and intervention-based research aimed at understanding cognitive functioning in OD.
Integration with Existing Literature
The various cognitive and self-regulatory deficits found for declarative, procedural and conditional knowledge, planning, evaluation and monitoring of comprehension related to opioid use are consistent with previous studies demonstrating that opioid use is associated with extensive and generalised executive function deficits.25, 48, 49 The chronic use of opioids is related to changes to the structure and function in several critical brain regions (i.e., the prefrontal cortex, anterior cingulate cortex and insula) that are involved in cognitive oversight, attentional regulation and error detection.11, 58, 59
Numerous studies have demonstrated that WM is significantly impaired in those who are having dependence on opioids. WM refers to the ability to hold information in mind over short periods of time and to manipulate this information using the ‘phonological loop’ (verbal WM) or the visuospatial sketchpad. Studies have found that prolonged use of opioids can disrupt both the phonological loop and the visuospatial sketchpad processes, leading to decreased N-back performance, lower levels of updating efficiency and decreased executive control.60, 61 For example, Rapeli 62 explained that participants with OD performed significantly lower level of performance than healthy controls on both verbal and visual N-back tests, indicating that they had less WM capacity and fewer abilities related to attention. Similarly, Darke et al. 63 documented impairments in attention, learning and memory among heroin users, which suggests that the cognitive problems experienced by heroin users are widespread and similar to those found in the present study.
Research using techniques of neuroimaging has provided additional evidence supporting the behavioural data previously described. Chronic opioid use has been linked to decreases in grey matter volume and reductions in white matter integrity in frontoparietal networks that are involved in memory (working), cognitive flexibility and meta-cognitive oversight.64, 65 Such structural and connectivity abnormalities have been linked to difficulties in verbal encoding, slower information retrieval and weaker visuospatial processing, patterns that are reflected in poorer performance on standard neuropsychological assessments.
The mindfulness-related deficits identified in the current research were supported by prior research demonstrating how chronic drug and alcohol use can lead to a decrease in awareness of the present moment; lower levels of interoception (the perception of internal bodily states); and lower ability to recognise internal experiences without judgement.23, 31, 66 These disruptions are thought to reflect dysregulation within prefrontal–limbic circuits, affecting attentional stability and emotional regulation, which may be associated with WM difficulties.
Interestingly, the relationship between mindfulness and metacognitive processing was greater in this sample compared to prior studies using Western samples.20, 34 This difference may represent some form of cultural influence unique to Indian culture. Men in collectivist societies (such as India) typically carry significant social, economic and interpersonal responsibilities, making it important to regulate oneself in order to meet expectations from others.67, 68 Such contextual demands may be associated with a closer coupling of cognitive monitoring and emotional–attentional regulation, which may help explain the high correlations observed in this study.
Novel Contributions and Cultural Context
Research on mindfulness and metacognition has commonly focused on them individually in studies related to OD.30, 69 The present study looks at both of these cognitive processes together from an integrated perspective and does so with a population that has been generally ignored in addiction research. An integrated perspective of mindfulness and metacognition, while examining the two through a similar analytical lens, is also theoretically relevant in supporting the idea that mindfulness and metacognition work jointly in relation to OD; theoretical frameworks have described mindfulness as a type of metacognitive awareness.28, 29
Second, India has had contemplative traditions for centuries (e.g., yogic attention practices and Vipassana), which may provide some basis for understanding what it means to be mindful in this culture.15, 70 Given that the availability of services related to mental health and cultural beliefs may impact how people engage in psychology-based interventions, such familiarity may also impact how people interpret and understand mindfulness-related concepts. 71
Third, many South Asian cultures place strong emphasis on collective family values, and because many people live in extended or joint families, those experiences may shape how people experience illness, participate in treatments and experience recovery.33, 72 The socio-demographic differences observed between individuals with OD and healthy controls highlight the importance of considering family context and cultural factors when examining cognitive and emotional functioning, underscoring the need for culturally informed research in South Asian populations.
International Relevance
The study’s findings have implications for mental health from a global perspective; the relationship found here between mindfulness and metacognition indicates a possible cognitive-emotional process that can be applied to other cultures, even though it is likely to be expressed differently due to varying levels of social support, marital expectations and economic pressure.71, 72 The finding is also supported by international evidence showing that both verbal and visual WM are processed using common executive control processes that are influenced by external factors such as stress exposure, environmental demands and cultural practice.75, 76
Another implication relates to the need for culturally responsive approaches to both research and treatment design. There is some evidence that evidence-based treatments such as MBRP and MCT require adaptation in order to make them relevant and acceptable in different settings and, therefore, require consideration of whether family members should be involved, the use of culturally meaningful metaphors, or indigenous contemplative practices.77, 78 There is also cross-national evidence that performance on the verbal and visuospatial N-back task is determined by more than just the neurocognitive load associated with each type of task, but also by the degree of exposure to attention training, contemplative practices and dominant cognitive norms in an individual’s culture.79, 80 These contextual factors could help explain why the relationship between mindfulness and metacognition was so much stronger than previously found in the current Indian sample.
A final implication relates to the use of internationally standardised measurement tools such as the MAI and the CAMS-R. These provide a way to compare data collected in one culture to those collected in another culture and enable researchers to contribute to international literature reviews and meta-analyses. This is consistent with the World Health Organization (WHO) recommendations that emphasise the inclusion of evidence-based psychosocial frameworks into drug use research and service delivery in low- and middle-income countries. 81 International neuropsychological studies have shown that many substance users around the world exhibit deficits in WM, which include difficulty with verbal updating, visual monitoring and attentional inhibition.82, 83 Structural magnetic resonance imaging (MRI) work links individual differences in metacognitive accuracy to grey matter volume in the anterior prefrontal cortex, supporting a neural substrate for self-monitoring and metacognition.84 Functional MRI (fMRI) studies of WM (N-back) reliably engage the dorsolateral prefrontal and parietal cortices; overlap between these regions and those implicated in mindfulness and metacognitive reports provides a plausible neurobiological route linking the three constructs.85
Taken together, these findings highlight the relevance of examining mindfulness and metacognitive processes within a global framework when studying cognitive functioning in OD. While the present results are correlational, they highlight the potential value of culturally adaptable research approaches for understanding executive functioning and cognitive vulnerability across diverse populations.
Theoretical Implications
Results from the study support the cognitive theory of how mindfulness and metacognition serve as related self-regulating strategies used in controlling attention and the ability to think flexibly. Research indicates that there is a positive relationship between mindfulness and an individual’s awareness of their cognitive state (i.e., ‘how we are thinking’), and also, there are many studies that have demonstrated a relationship between mindfulness and an individual’s ability to ignore or block out distractions (irrelevant stimuli) while focusing on a particular task. Both of the above-mentioned relationships exist because they are thought to contribute to higher-order cognitive functioning.84,85 In line with this framework, the current study’s output showed statistically significant associations among mindfulness, metacognition and WM outcomes.
Clinical Implications
Results from this study provide evidence that both mindfulness and metacognitive processes can serve as potential constructs in future research examining cognition in individuals who have been diagnosed with OD. Results from the study were consistent with prior research examining mindfulness and metacognitive processes in relation to attention and WM. As such, the majority of previous intervention-based research has focused on either mindfulness or metacognitive processes to develop strategies to improve executive function and self-regulation. However, due to the cross-sectional nature of this study, no causal inference could be made. Therefore, in India, which has a cultural familiarity with contemplative practices, longitudinal and intervention-based methods should be utilised to continue to investigate the cognitive domains mentioned above.
Limitations
Limitations of the current study are discussed next. A major limitation of the study was that it used a cross-sectional design, which does not allow for making any conclusions about cause and effect. Another significant limitation of the study is that it only included male participants, and therefore, the results from the study cannot be generalised to other populations. Mindfulness and metacognition were self-report inventories that may be resulted in biasness. Clinical details such as duration and severity of opioid use were not systematically recorded, and residual withdrawal or subclinical symptoms may have affected cognitive performance.
WM was assessed only through N-back tasks, offering a limited view of cognitive functioning. Participants were drawn from a single geographic region, which may restrict global applicability. The correlational nature of the analyses means that alternative explanations for the observed relationships cannot be ruled out.
Very large effect sizes were observed for metacognitive awareness, likely reflecting strong group differences alongside low variability among healthy controls. To improve clarity and reduce potential inflation, analyses focused on overall metacognitive scores rather than individual subdomains.
Future Directions
Future studies could use longitudinal and intervention-based designs to clarify how mindfulness and metacognitive processes influence changes in WM across time. The inclusion of comprehensive neurocognitive test batteries alongside neuroimaging methods such as fMRI, electroencephalography (EEG) and diffusion tensor imaging (DTI) may help clarify the neural pathways associated with these cognitive processes. Greater inclusion of women, adolescents and participants from culturally diverse backgrounds, particularly within the Indian context, is needed to enhance generalisability and to better understand culture-specific influences on cognition.
Further studies may explore how cognitive rehabilitation approaches and integrated mindfulness–metacognitive frameworks are associated with verbal and visual memory functioning. Examining factors such as duration of opioid use, polysubstance involvement, treatment modality and psychosocial stress may also provide insight into individual differences in cognitive profiles. Finally, implementation-focused research is needed to assess the feasibility, acceptability and scalability of culturally adapted approaches within community and primary-care settings in India.
Conclusion
The study shows that men with OD have significant deficits in WM, metacognition and mindfulness, with both cognitive processes strongly predicting memory performance. The observed associations indicate that mindfulness and metacognition may be important targets for future research examining cognitive functioning in OD.
Footnotes
Authors’ Contributions
Hemant Kashyap conceptualised the study, designed the research framework, and prepared the manuscript. Lalhmingmawii Khiangte supervised data collection and Nandan Kumar Thakur contributed to data collection and statistical analysis. Sunita Purty, Kalpana Randhawa and Karuna Kashyap assisted in data interpretation and manuscript editing. Khushpreet Kaur and Abhilasha Agarwal contributed to literature review and manuscript preparation. Vinod Kumar Shanwal provided academic guidance and critically reviewed the manuscript. All authors read and approved the final manuscript.
Statement of Ethics
This study was approved by the Human Ethics Committee of Mizoram University, Aizawl, India (Approval No. MZU/HEC/2024/019; June 17, 2024). Written informed consent was obtained from all participants prior to their participation, and all procedures were conducted in accordance with institutional ethical guidelines.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ICMJE Statement
All data collection, analysis and manuscript preparation were conducted independently.
Patient Consent
Written informed consent was obtained from all participants prior to their inclusion in the study. Participants were informed about the study purpose, procedures, confidentiality, voluntary participation and their right to withdraw at any time without penalty.