
Abstract
Background
Studies suggest that obesity is linked to both autonomic nervous system dysfunction and cognitive impairment, but the specific quantitative associations are not well explored.
Purpose
This study was proposed to explore the quantification of different neurocognitive signatures and heart rate variability (HRV) parameters with increasing body weight among metabolically healthy obese participants for better analytical predictors.
Methods
The present research is a cross-sectional study, including a total of 101 (n = 101) participants. Out of the total, 71 were metabolically healthy obese or overweight individuals (body mass index [BMI] = 23.0–30.0 kg/m2; age 36–55 years; both genders) and 30 participants were enrolled as the control group. All the participants completed various neurological and psychological assessments, including the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), serum levels of brain-derived neurotrophic factor (BDNF) and cardio-autonomic tone by HRV analysis.
Results
Significant changes were observed for neurocognitive performances and HRV indices for the metabolically healthy obese group compared with the control group. With the association heatmaps, BMI was found to be significantly negatively associated with the BDNF and high-frequency band (HF band, ms2). In socio-demographic-adjusted models, the analysis showed a substantial decline (p < .05) in the HF band, ms2 with an increase in BMI, emphasising its significant effect on vagal tone among the obese group. Also, a noteworthy association between BDNF levels and the standard deviation of all normal-to-normal intervals (SDNN)-HRV indices have confirmed the robustness of the findings for obese participants when compared with the control group.
Conclusion
The findings of the present study support that HRV could be a valuable early non-invasive tool for future cognitive decline in a population with metabolically healthy obesity.
Clinical Trial Registry
The study was registered at Clinical Trial Registry of India (CTRI/2022/10/046935).
Keywords
Introduction
In today’s era, obesity and being overweight are the major concerns in modern society and its related healthcare policies. 1 These health issues are due to decreased physical activity, consumption of fatty food items and sweetened carbonated drinks and sedentary lifestyles that potentially impact the quality of life in modern society.2, 3 From the above scenario, studies have shown that overweight and obesity are associated with autonomic disturbances, poor cognitive performance, cognitive decline and dementia at various ages, but less is known about the physiological basis of these differences and about prognostic predictors.4–12
Heart rate variability (HRV) has become a valuable cardinal biomarker of cardiac autonomic tone 13 and studies have shown that reduced HRV has been associated with risk factors for cognitive impairment, such as high cholesterol, hypertension, diabetes mellitus and depression 14 ; yet the more direct association between HRV and cognitive functioning is poorly understood and rarely explored, especially among metabolically healthy obese populations. Further, it is also unclear whether worsening of autonomic nervous system function during mid-to-late-life could predict worse cognitive performance with increasing body mass index (BMI). 15 Therefore, the present study proposed to explore and quantify the relationship between cardio-autonomic tone regulation as measured by HRV and neurocognitive variables using the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA), as well as a cognitive biomarker, namely brain-derived neurotrophic factor (BDNF), among middle-aged metabolically healthy overweight and obese participants.
Methods
Study Population
A present cross-sectional research study was carried out in the Department of Physiology in collaboration with the Department of Psychiatry, Endocrinology and General Medicine at AIIMS-Bathinda, from January 2023 to March 2024. After the approval from the Institutional Ethics Committee (IEC/AIIMS/BTI/370) and the Clinical Trial Registry of India (CTRI/2022/10/046935), a total of 101 middle-aged metabolically healthy obese participants were enrolled, aged between 36 and 55 years of both genders. From the total, 71 participants were metabolically healthy, overweight or obese with BMI values between 23.0 kg/m2 and 30.0 kg/m2; as per Indian Council of Medical Sciences, New Delhi (ICMR) guidelines (2014), 16 and 30 participants were controls with BMI 16 of 18.5–22.9 kg/m2. Patients with a history of smoking and alcohol, who were currently involved in any weight-reduction programme, cases of diabetes or hypertension, neuroendocrinological illnesses or taking drugs for any chronic diseases were excluded from the study. The goal of involving the control group was only to comprehend the normal difference in HRV indices and cognitive functions. All patients provided their informed consent.
Anthropometric Measurements
The participant’s height was recorded using a standardised stadiometer (Holtain Ltd., UK). Body weight measurement was carried out with the help of a digitised weighing balance (Seca, Germany). Waist circumference (WC) was estimated at the widest part of the trunk, between the xiphoid process and the iliac crest. Systolic and diastolic blood pressure were measured in the sitting and resting position using a sphygmomanometer.
Cognitive Assessment Tools
All participants in the present study completed their valid and reliable cognitive tools—MMSE and MoCA questionnaires (both the English and Hindi versions)—under the guidance of an expert clinician from the Department of Psychiatry.
Mini-Mental State Examination 17
It consists of 11 sets of questions with different cognitive domains, including orientation, registration of words, attention, calculation, recall and language. The total score is 30 and a score of <24 indicates cognitive impairment.
Montreal Cognitive Assessment 18
It consists of two main domains that include recalling memory and executive functions. MoCA scores were categorised as severe cognitive deficit (<10), moderate cognitive deficit (10–17), mild cognitive deficit (18–25) and normal cognition (>26).
Electrocardiograph Recording and HRV Analysis13, 19
ECG recordings and HRV were carried out between 08:00 and 10:00 h, as per the guidelines of the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. 20 The ECG recording of the data obtained by the PowerLab 26-T system and LabChart hardware and software version 8.0 of AD instruments were used for time and frequency analysis. The time domain includes the mean heart rate (HR, beats per minute), standard deviation of all normal-to-normal intervals (SDNN, ms) and RMSDD (ms). While the frequency domain includes VLF (0.0037–0.04 Hz), low frequency (LF; 0.04–0.15 Hz) and high-frequency (HF; 0.15–0.4 Hz). After this, the participants were made to feel comfortable.
Serum Levels of Brain-derived Neurotrophic Factor4, 21, 22
A molecular marker for neurotrophic sustenance and synaptic plasticity. The fasting venous blood (5 mL) was taken during morning hours between 8:00 and 10:00 h for the estimation of the marker as per the company protocol, a commercially available sandwich-based ELISA kit (G-Biosciences Human BDNF ELISA Kit; Immunotag™ Inc., USA). The detection limit for clinical evaluation of BDNF levels ranged from 31.25 to 2000 pg/mL. The quality control and validation were performed for the present biomarker. The fasting blood glucose levels were estimated by an enzymatic method using commercially available kits (Randox Laboratories Ltd., UK).
Statistical Analysis
The present study data were analysed using SPSS software version 29.0 (IBM, Chicago, Illinois, United States of America, October 2020). The data normality was analysed using the Kolmogorov–Smirnov test. The present study data are presented as mean ± standard deviation and interquartile range for parametric and non-parametric variables, respectively. The differences in mean values for various socio-demographic and neuropsychological variables were analysed using an ‘independent two t-test’ for parametric data and a ‘Mann–Whitney test’ for non-parametric data. The ‘multivariate linear regression’ analysis was applied to explore the quantitative relationship between BMI and BDNF, MoCA, MMSE and HRV indices. The correlation heat maps were evaluated between BMI and various neurocognitive parameters and HRV indices with Spearman’s rank correlation coefficient analysis. Statistical significance was considered at p value <.05.
Results
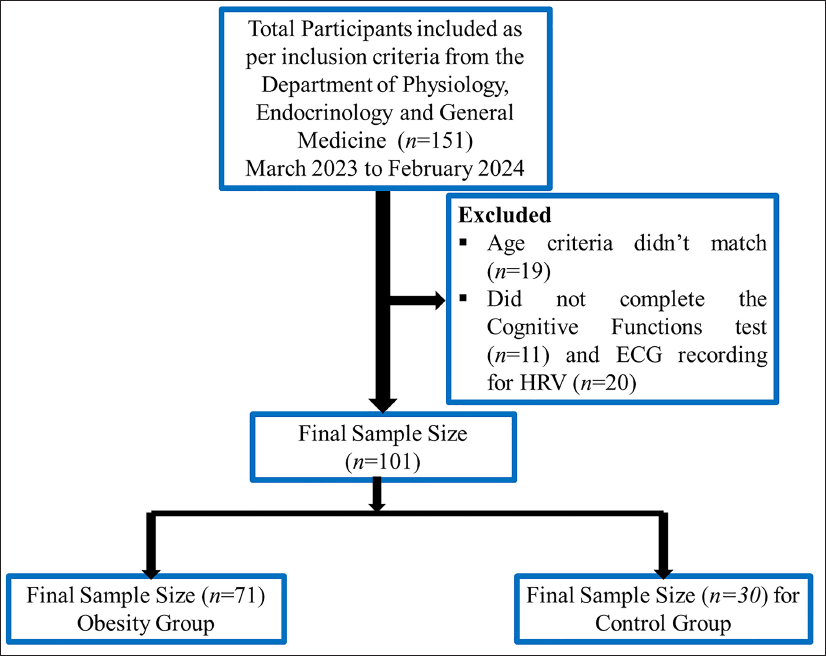
A total of 71 (n = 71; F = 25, M = 46; age 44.29 ± 7.32 years) metabolically healthy obese participants and 30 (n = 30; age 44.16 ± 6.70 years) control participants were included in the analysis. The selection of the sample process for the study is shown in the form of a flowchart Figure 1. The participants with obesity had a baseline BMI of 27.53 ± 2.31 kg/m2 and the control group had a BMI of 22.68 ± 1.57 kg/m2. The mean differences were found to be significant for weight (p = .002), BMI (p = .001), WC (p = .01), FBG levels (p = .02), systolic blood pressure (SBP; p = .04), MoCA scores (p = .03) and MMSE scores (p = .01) were observed for the obese group versus control group with independent two t-test with equal variance as shown in (Table 1). Whereas using the Mann–Whitney test, the serum BDNF levels was significantly (z = −4.26; p = .001) reduced and LF/HF ratio was found to be significantly increased (p = .05; p = .001, respectively), HF frequency band (p = .012), root mean square of successive differences (RMSSD; p = .016) and pNN50% (p = .001) was found to be significantly reduced for obese participants versus controls. For the other HRV indices, including LF-band and SDNN, the average RR interval was found to be altered among obese participants when compared to controls, though it was not found to be statistically significant (Table 1).
Flowchart: Present Study Sample Selection Process.
Socio-demographic and Anthropometric Variables Among the Obese Group Versus the Control Group.
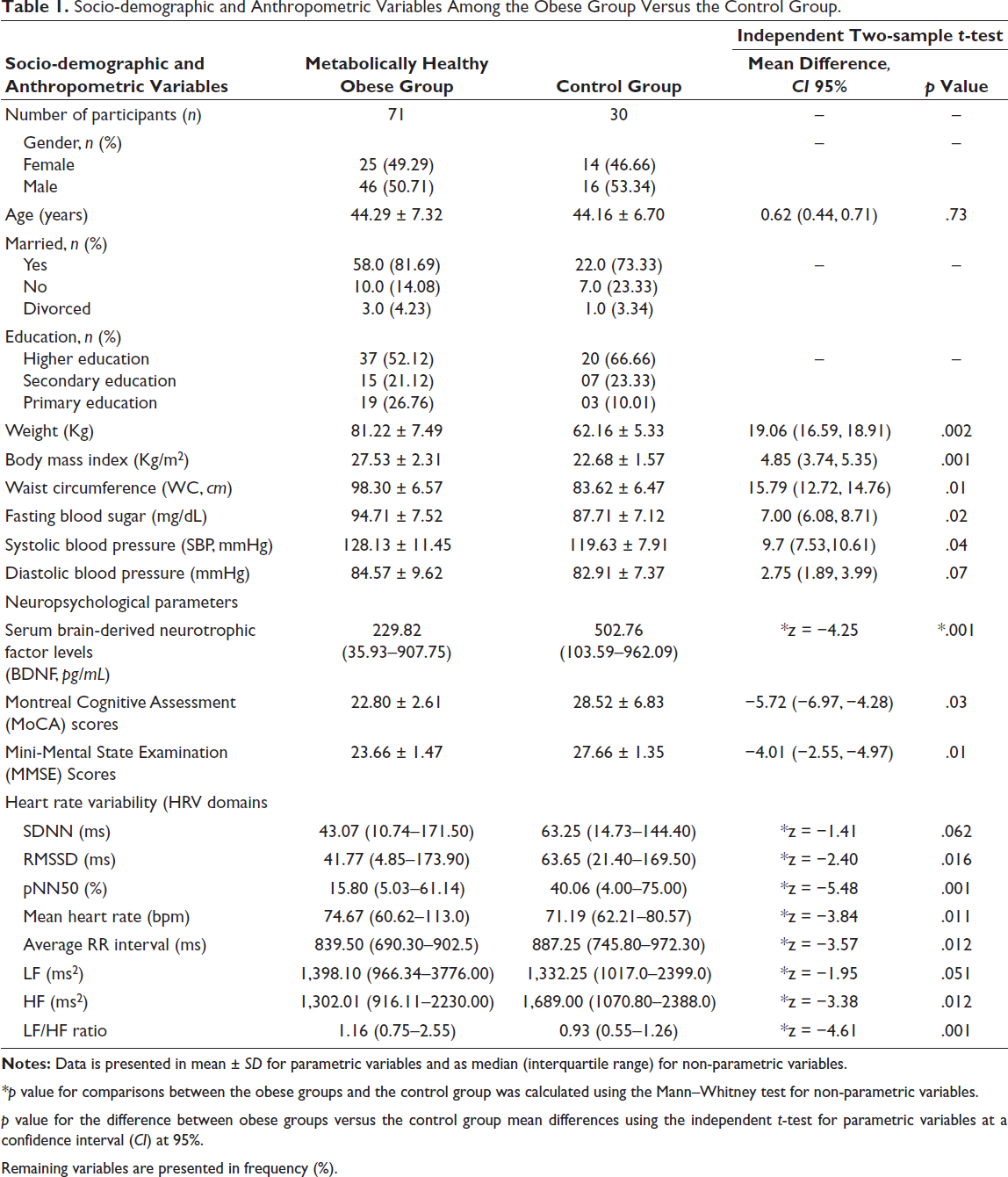
*p value for comparisons between the obese groups and the control group was calculated using the Mann–Whitney test for non-parametric variables.
p value for the difference between obese groups versus the control group mean differences using the independent t-test for parametric variables at a confidence interval (CI) at 95%.
Remaining variables are presented in frequency (%).
Associations Between Different Neurocognitive Functions and HRV Indices
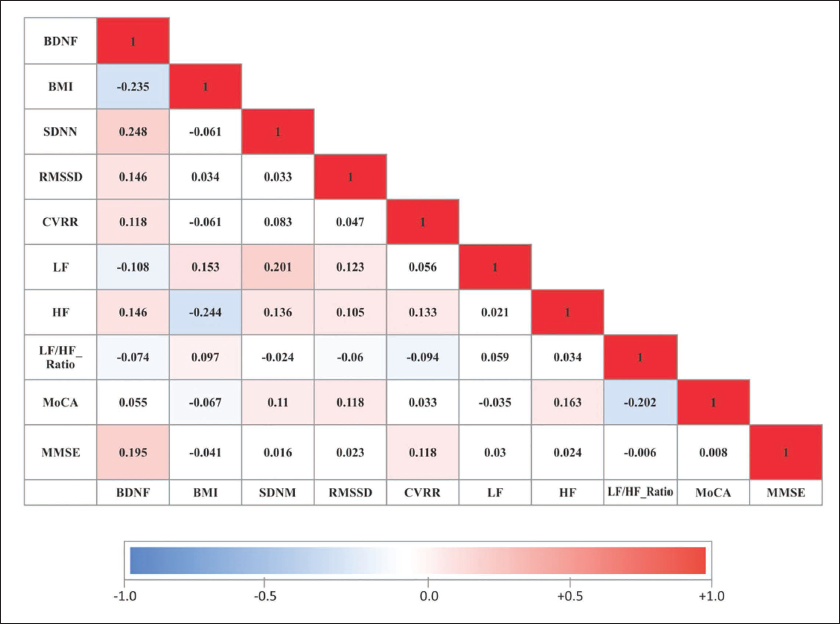
Using a multi-directional pattern, distinguished variances were observed in the correlation between BMI and different neurocognitive functions, along with HRV indices among middle-aged metabolically healthy obese participants. With correlation heat maps, a noteworthy negative association was observed between the BMI and the serum BDNF concentration (r = −0.23, p = .049) and with the HF band power (r = −0.244, p = .01) among obese participants. Interestingly, a positive correlation has been observed in serum BDNF levels with SDNN (r = 0.248, p = .03) and with HF, showing a trend of positive correlation (r = 0.146, p = .05) (Figure 2). However, other variables, including SDNN, RMSSD, CVRR, MoCA and MMSE, show a negative correlation with BMI but are not statistically significant. A positive correlation between BDNF levels and RMSSD, CVRR, MoCA and MMSE was observed and a negative correlation with LF band and LF/HF ratio, though statistically not significant (Figure 2).
Correlation Heat Map Between Heart Rate Variability, Body Mass Index (BMI) and Brain-derived Neurotrophic Factor (BDNF) Among the Obese Group (n = 71).
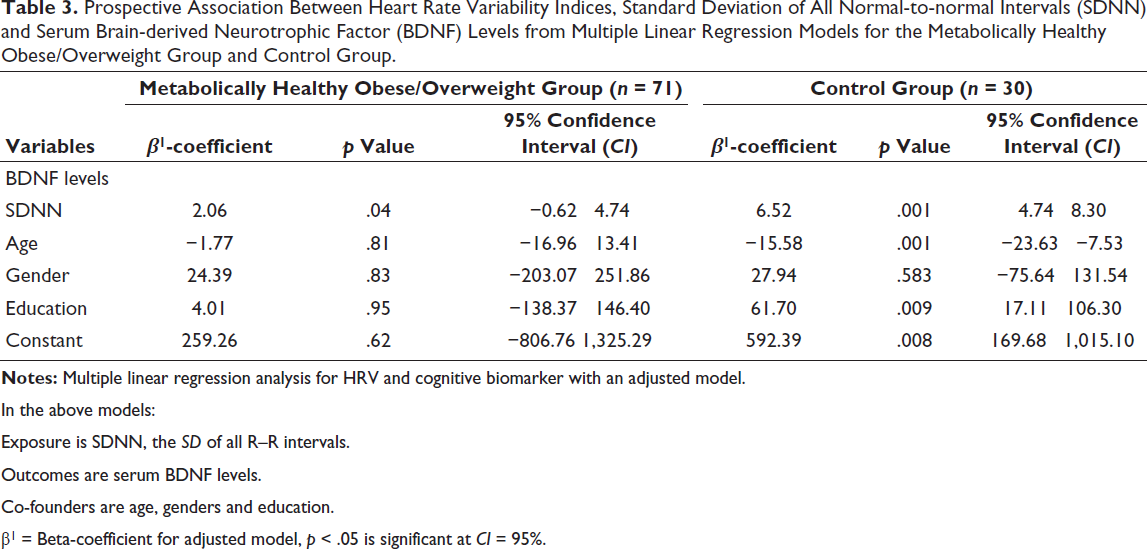
Further, to evaluate the strength of the relationship between BMI and different neurocognitive functions along with HRV indices, the multivariate linear regression was used for all possible confounders, which include age, gender and education. The negative association with the β-coefficient of −4.72, with CI at 95% of −42.61, 33.16; p = .04 between BMI and HF band has been observed significantly. This negative association signifies that as BMI increases with each unit, the HF band has a tendency to decrease with a magnitude of −4.72 and vice versa, affecting the body’s parasympathetic system, as shown in Table 2. Also, there is a trend of negative association between BMI and SDNN, but it is not statistically significant (p = .05). On the other hand, when the strength of association between neurocognitive functions and HRV indices was quantified, the present study found a significant positive association between serum BDNF levels and SDNN with a β-coefficient of 2.06 with CI at 95% of −0.62, 4.74, p = .04 has been observed. This positive association signifies that serum BDNF levels have a tendency to increase by 2.06 as SDNN increases with each unit and vice versa (Table 2). Importantly, when comparing the above association with the control group (β-coefficient of 6.52 with CI at 95% of 4.74, 8.30, p = .001), the authors observed that at the resting state, the control group had a better power to regulate the sympathetic and parasympathetic activity simultaneously than obese participants, which could reflect autonomic regulation of cognitive functions (Table 3). There is a trend of a positive association between BDNF levels and the HF band, though it is not statistically significant (Table 2).
Correlation Strength Between Body Mass Index and Different Neurocognitive and Heart Rate Variability (HRV) Variables Using Multivariable Linear Regression Among the Obese Group.
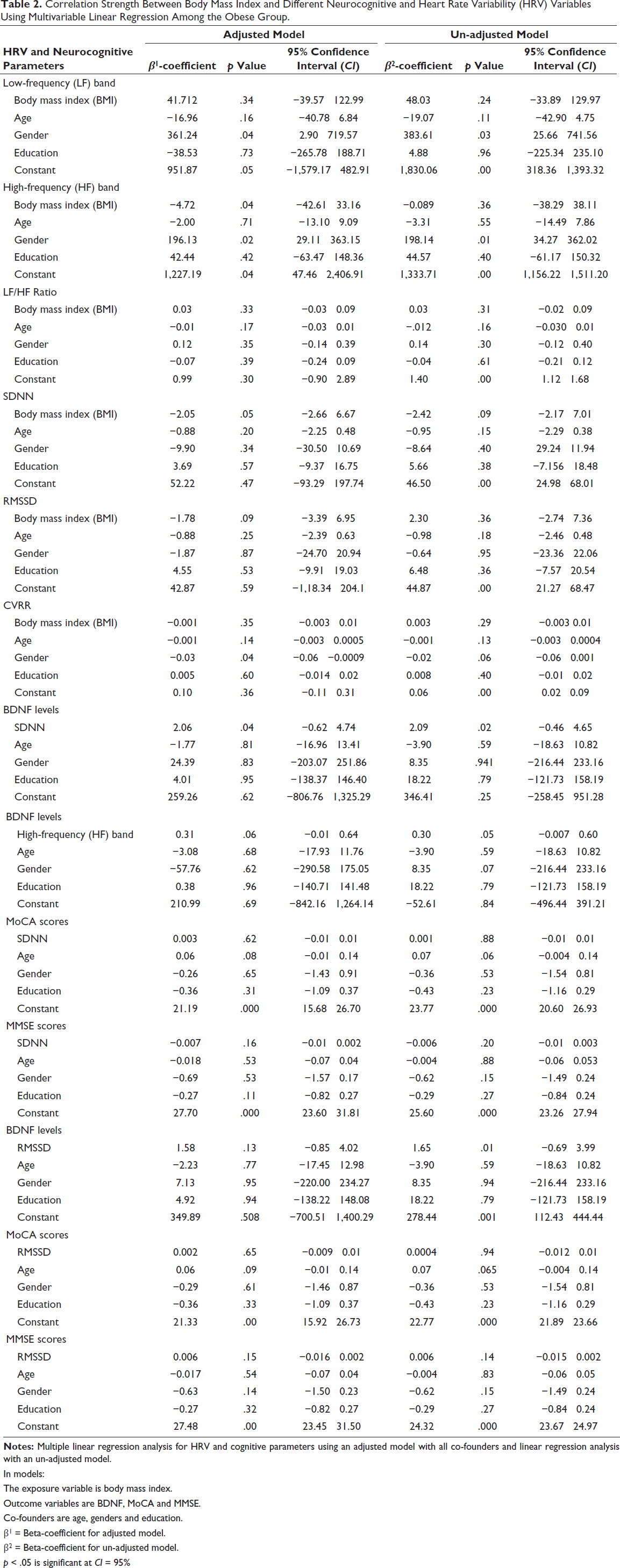
In models:
The exposure variable is body mass index.
Outcome variables are BDNF, MoCA and MMSE.
Co-founders are age, genders and education.
β1 = Beta-coefficient for adjusted model.
β2 = Beta-coefficient for un-adjusted model.
p < .05 is significant at CI = 95%
Prospective Association Between Heart Rate Variability Indices, Standard Deviation of All Normal-to-normal Intervals (SDNN) and Serum Brain-derived Neurotrophic Factor (BDNF) Levels from Multiple Linear Regression Models for the Metabolically Healthy Obese/Overweight Group and Control Group.
In the above models:
Exposure is SDNN, the SD of all R–R intervals.
Outcomes are serum BDNF levels.
Co-founders are age, genders and education.
β1 = Beta-coefficient for adjusted model, p < .05 is significant at CI = 95%.
Discussion
The present study explored and quantified the implications of BMI and neuro-cognitive markers along with HRV indices among metabolically healthy obese adults using the cardio-psychological approach. In our study, obese participants had significantly higher body weight, BMI and WC when compared to the controls. Also, the resting blood pressure and HR were significantly higher in the obese group than in the control group. Several epidemiological research findings12, 23 were in line to show the increase in basal HR and blood pressure due to variations in the autonomic modulation of the inherent HR.
The present study observed notable reduced cognitive functions with increasing BMI among the obese group versus the control group. The decrease in BDNF levels may be due to high levels of oxidative stress, increased rate of neuroinflammation, unhealthy lifestyle, brain ageing, alterations in the BDNF gene or its receptor-tyrosine kinase-B (Trk-B) and zinc finger downregulation by alteration in neuronal development and inhibiting the hormone-receptor interaction in individuals with obesity.24–26 The study also observed a mild cognitive deficiency with MoCA and MMSE scores, which was positively strengthened by reduced BDNF levels in obesity, revealing further cognitive task errors. Present findings showed variation with Monteleone et al. 27 study, noted a significant increase in BDNF-blood levels with increasing body weight. This discrepancy in the previous research findings may be due to variations in the duration of obesity, 28 an integrated cultural factor, participants’ age-group and methodological limitations.28, 29
The HRV variables SDNN, RMSSD, pNN50 and HF band power indices reflect cardiac parasympathetic nerve activity, with being lower in the obese group compared with the control group. Moreover, as expected, the sympathetic marker LF-band power and LF/HF ratio increased in obese participants compared to the control group. These findings were affirmed through correlation analysis and showed the altered state of autonomic activity/HRV indices with increasing BMI among the obese group. Studies by Thorp et al. 30 Laederach-Hofmann et al. 31 and Esler et al. 32 support our findings and they have observed that the obese population had evidently increased risk of cardiovascular disorders due to lowered parasympathetic or heightened sympathetic activation. At baseline, the obese group had decreased HF values when compared to the control participants because of reduced vagal tone/function. These findings support the present correlation studies that showed a negative correlation between HF band activity and increasing BMI. Previous studies are in line with the present findings, showing a decreased vagal function among children and adolescents.21, 28, 32 In contrast to the present findings, sympathetic activity was found to be decreased in obese participants, as has also been described in some reports.15, 28 This inconsistency in findings may be due to alterations in the length of obesity and sample size.15, 28
Importantly, to generalise these findings to the entire obese population, the authors authenticated the present findings using the strength of the relationship with BMI, different neurocognitive functions and HRV indices. For this, multivariate linear regression models’ analysis was carried out for socio-demographic variables for all possible confounders, including age, gender and education. A significant negative correlation with the β-coefficient of −4.72 between the HF band activity and BMI has been observed. This negative correlation signifies that the HF band activity has a tendency to reduce by an extent of −4.72 as BMI increases by one unit and vice versa, also affecting the age levels, which signifies a decreased vagal tone regulation among the obese group. On the other hand, a trend of negative association between SDNN and BMI was observed to signify the altered state of both sympathetic and parasympathetic activity.
Further, a positive correlation between BDNF levels and SDNN, an HRV measure, has been observed among middle-aged obese participants. BDNF plays a role in synaptic plasticity, learning and memory by enhancing neuronal bioenergetics 33 ; while on the other hand, SDNN, as a measure of HRV, reflects the balance between both divisions of the autonomic nervous systems. 34 The positive association between BDNF and SDNN, which accounts for the synchronised activity between the sympathetic and parasympathetic nervous system, could represent the autonomic regulation of the baroreflex influencing the cognitive health35, 36 among metabolically healthy obese participants. Also, a plausible mechanism behind synchronising activity of the autonomic nervous system may be due to binding of BDNF (a neurotrophic factor) to Trk-B receptors on brainstem cholinergic neurons, particularly in the dorsal motor nucleus of the vagus (DMNV), hence regulating the parasympathetic tone, which in turn, enhances cognitive health. 33 Present study findings are supported by one previous study, which showed that an increase in BDNF was significantly correlated with both basal SDNN and RMSSD among the patients with Chagas disease. 37 This strong association between BDNF and SDNN suggests that BDNF could be a potential biomarker for assessing autonomic nervous system function and potentially tracking the effectiveness of interventions that impact both BDNF and HRV. When compared with the control group, this strength of association between SDNN and BDNF was found to be greater when compared to the obese group, affirming the direct association between cardio-autonomic activity and cognitive functions. RMSSD, a measure of the parasympathetic activity, may not support the above concept since both divisions of the autonomic nervous system act synergistically for the regulation of neuronal growth, survival and maintenance and their apoptotic death that preserves the human brain’s cognitive signatures.35–38 Overall, the present study indicates that both reduced BDNF levels and decreased HRV are associated with obesity, potentially related to autonomic nervous system dysfunction impacting cognitive health.
Though the present study was conducted with conceptual analysis, it has a few limitations that include, first, the findings of this study with other HRV indices and neurocognitive functions could not be statistically significant due to the small datasets and need to be corroborated with larger datasets. Second, the present study did not evaluate the possible effects of menstrual cycle phases on cognitive parameters. Third, the correlation of the diet domain with cognitive functions and different HRV indices could not be carried out. In spite of these limits, the present findings have provided technical indication with multi-regression-based explanations for overweight/obese participants to be alert of their mental and autonomic status, which will provide direction to undergo lifestyle amendment programmes. However, the present study results provide appreciated perceptions into the elaborate association between cognitive functions, along with cardio-autonomic status and obesity among the Indian population. Further, cognitive sub-domain analysis with respect to different HRV indices is not analysed for the present study and will be included in a future research article.
Conclusion
The study scientifically upholds the measurable deterioration in neurocognitive functions with the reduction in HRV among middle-aged metabolically healthy obese participants. These results also support the impression that HRV could be a valuable tool for early detection of decline in cognition among the population with metabolically healthy obesity.
Footnotes
Abbreviations
BMI Body mass index
MHO Metabolically healthy obese
HRV Heart rate variability
RMSSD Root mean square of successive differences
SDNN Standard deviation of all normal-to-normal intervals
pNN50 Proportion of NN50 divided by the total number of NN (R-R) intervals
BDNF Brain-derived neurotrophic factor
MoCA Montreal Cognitive Assessment
MMSE Mini-Mental State Examination
HF power Absolute power of the high-frequency band (0.15–0.4 Hz)
LF power Absolute power of the low-frequency band (0.04–0.15 Hz)
LF/HF Ratio of LF-to-HF power
Research Highlights
Acknowledgement
The authors thank the participants for cooperating to make this research possible. Thanks to the committed research team, collaborators and institutions (All India Institute of Medical Sciences, Bathinda, Punjab, All India Institute of Medical Sciences, New Delhi and Centre for Biomedical Engineering, IIT Delhi) for their invaluable support.
Authors’ Contribution
Saksham Bansal, Sakshi Charaas and Vanshita Grag, MBBS students (4th year): Recruitment of the participants for the study. Dipti Magan: Study conceptualisation, study design, acquiring and interpreting the data, manuscript writing and manuscript review. Sudhashekhar Kumar: Recruitment of the participants and proofreading. Raj Kumar Yadav: Interpretation of datasets and manuscript review and approving the final content of the manuscript. KK Deepak: Data interpretation, drafting and revision to the manuscript. Jitender Aneja: Psychological questionnaire analysis and data interpretation. Shivam Pandey: Data analysis and data interpretation.
The present article material is original research, has not been previously published and has not been submitted for publication elsewhere while under consideration for Annals of Neurosciences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants included in the study.
Statement of Ethics
All study procedures and protocols involving human participants were approved by the Institutional Ethics Committee (IEC/AIIMS/BTI/370) and adhere to the tenets of the Declaration of Helsinki.
Use of Artificial Intelligence Assisted Technology for Manuscript Preparation
The authors confirm that there was no use of artificial intelligence (AI)–based technology for assisting in the writing of the manuscript and no figures were deployed using AI.