
Abstract
Background
Depression and active smoking are very common situations among the population, which also reduces the positive mental well-being of a person. Smoking is a global issue, and depression and low mental well-being interfere with the daily lives of individuals.
Purpose
This study aimed to investigate the effect of meditation on an active smoker in terms of depression and psychological well-being (PWB) as variables.
Method
The study used the pre-test and post-test design with 100 participants who were actively engaged in daily smoking. The individuals were divided equally into the two groups, and depression and PWB scores were recorded for both groups in the pre-test period. After recording the scores, the experimental group received meditation practice for one week, while the control group received no treatment. After one week, depression and PWB scores were again tested in the post-test period for both groups and recorded.
Results
Paired-samples t-tests revealed a significant decrease in depression scores from pre-test (M = 54.36, SD = 4.91) to post-test (M = 28.10, SD = 6.05), t(49) = 24.70, p = .01, and a significant increase in PWB scores from pre-test (M = 57.50, SD = 4.91) to post-test (M = 65.88, SD = 4.94), t(49) = 9.96, p = .01. Independent-samples t-tests showed that post-intervention, the experimental group had significantly higher depression scores (M = 55.02, SD = 4.42) compared to the control group (M = 28.10, SD = 6.05), F = 7.14, p = .05, and significantly lower well-being scores (M = 56.60, SD = 4.69) versus (M = 65.88, SD = 4.94), F = 0.017, p = .05.
Conclusion
The intervention was effective in reducing depressive symptoms and enhancing PWB among participants, demonstrating its potential as a beneficial programme for mental health improvement.
Introduction
Smoking is a major global health issue and refers to the inhalation and exhalation of plant-based burning substances, such as marijuana, cocaine, or most commonly, the dried leaves of the tobacco plant, into the bloodstream. 1 India faces a high risk from tobacco use, with about 29% of adults (267 million) using tobacco and 10.7% smoking regularly; smokeless forms like gutkha are even more common, especially in rural areas.2, 3 Men smoke far more than women, and tobacco contributes to roughly 1.35 million deaths annually. 2 Tobacco use also poses serious psychological risks. Users have 28% higher odds of depression, higher stress, poorer coping, and lower quality of life.4, 5 Adolescents who use cigarettes or e-cigarettes show anxiety, irritability, and low self-esteem. 6 These effects extend to families and communities, particularly in low-income and rural groups, highlighting the need for integrated mental health and cessation programmes. 7 Evidence shows smoking worsens existing mental health symptoms, while cessation reduces stress, anxiety, and depression, improving overall well-being similar to antidepressant therapy.8, 9 Addressing tobacco addiction alongside psychological health is crucial for public health in India. Tobacco’s nicotine is highly addictive, reaching the brain within seconds. 10 It briefly enhances mood, focus, and relaxation but alters brain chemistry with regular use, leading to dependence. The relationship between smoking and depression remains unclear, whether smoking causes depression or if depression increases the likelihood of smoking. 10
Depressive symptoms often appear early in nicotine dependence and during withdrawal, and smoking increases the risk of mental health disorders, worsening existing conditions, and contributing to a negative self-image. 11 Current and past smoking habits elevate the risk of developing schizophrenia, bipolar disorder, and major depression. 12 Tobacco smoking has been shown to cause more premature deaths than most other human behaviours. 13 It can also lead to or worsen schizophrenia and depression, 14 with smokers being twice as likely to experience depression and heavy smokers up to four times as likely. 15
Recent studies strengthen this association. A longitudinal study in Korea found a clear correlation between smoking intensity, cotinine levels, and depressive symptoms. 16 A 2024 Pakistani study also confirmed a significant link between nicotine dependence and depression severity. 17 Similarly, a Mendelian randomisation study from the U.S. NHANES (2005–2018) found consistent evidence of an association between tobacco exposure and depression. 18 Moreover, new research in 2025 highlights barriers and psychiatrists’ perspectives in smoking cessation among people with serious mental illness and integrates cessation treatment into psychotherapy. 19
The onset of smoking is correlated with psychotic and depressive symptoms, while cessation improves quality of life. 20 Smoking is linked to neuroticism rather than extraversion. 21 Severe nicotine dependence is associated with poorer quality of life. 22 Smoking harms physical, social, and mental well-being, particularly among older adults. 23 In contrast, smoking cessation leads to improved health-related quality of life and better psychological health over time. In contrast, relapse and second-hand smoke exposure contribute to a lower quality of life. 24
Conceptual Framework
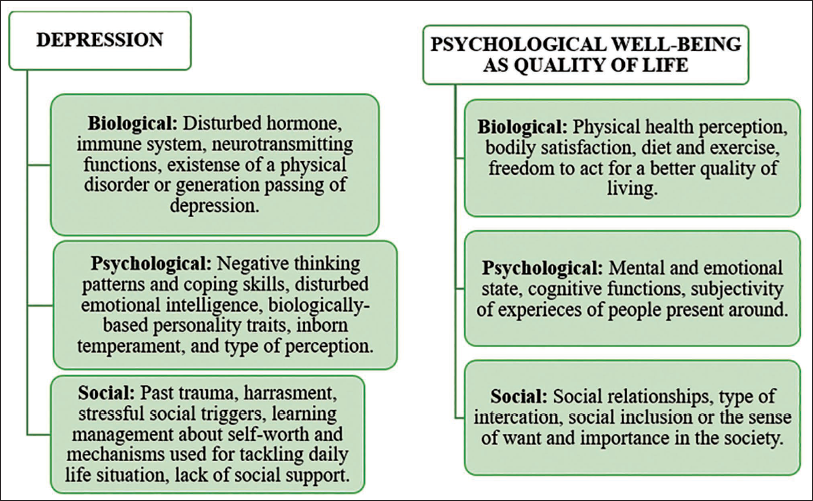
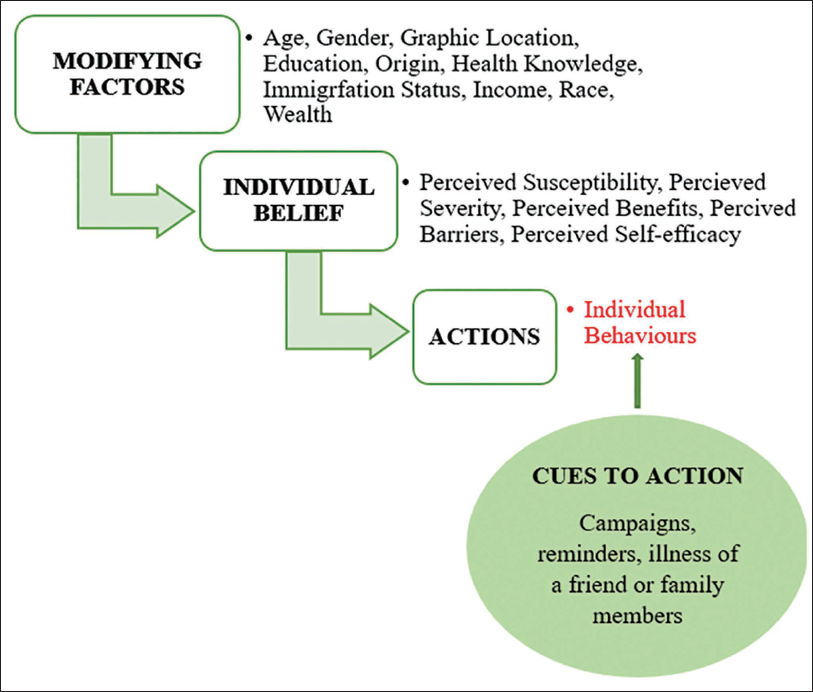
Depression and psychological well-being (PWB) are influenced by a complex interplay of biological, psychological, and social factors, as outlined in the (Figure 1) Biopsychosocial (BPS) Model. While biological factors such as hormonal imbalances, genetic predisposition, and chronic illnesses contribute to vulnerability, psychological factors like coping mechanisms, emotional intelligence, and cognitive patterns interact with social experiences, including trauma, separation, and interpersonal stressors, to shape mental health outcomes. 25 PWB, as defined by WHO, reflects a person’s ability to manage stress, maintain emotional balance, foster meaningful relationships, and realise personal potential.26, 27 The Health Belief Model (HBM) (Figure 2) further emphasises that perceptions of risk, severity, benefits, barriers, and self-efficacy influence health behaviours. 28 Integrating these models provides a multidimensional understanding of how individuals adopt behaviours that promote mental and physical health. Figure 1 shows the BPS model.
Biopsychosocial Model (BPS Model) Outlines the Biological, Psychological, and Social Framework.25–27
The Health Belief Model (HBM). 28
Although previous research has extensively examined depression and PWB, few studies have investigated the effectiveness of interventions designed to simultaneously reduce depressive symptoms and enhance PWB using multidimensional approaches. Most prior studies focus either on symptom reduction or well-being enhancement in isolation, without evaluating the combined impact of targeted interventions on both outcomes. Additionally, limited research has examined how structured interventions can produce measurable improvements in both depression severity and PWB, particularly through pre- and post-assessment using validated tools such as the depression and the PWB. The present results, showing significant reductions in depression and increases in well-being in the experimental group, underscore the need for integrated intervention strategies and highlight a gap in understanding how combined approaches can optimise mental health outcomes.
Objectives
This research article aims at the following objective:
To examine the effect of meditation on depression and PWB among active smokers.
Hypothesis
There will be a significant effect of meditation on depression and PWB among active smokers.
Method
Design
This study used a pre-test and post-test design with two groups: an experimental group with pre- and post-intervention, and a control group. This design is best suited for this article to evaluate the effectiveness of the intervention technique by comparing changes across the two groups and within the experimental group. It allows a clearer understanding of the intervention technique applied, as it makes the comparison of pre- and post-treatment scores easier for the experimental group, and also provides insight into the changes that occurred or did not occur in the control group, where no intervention is given. 29
Sampling
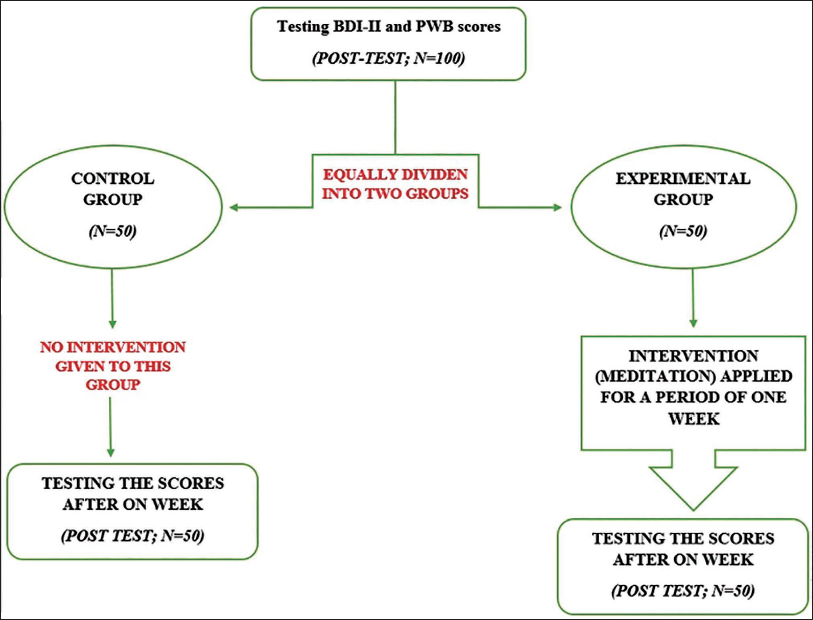
Initially, one hundred participants were picked, including students in the age group 18–30 years old, who agreed to be active smokers as per the inclusion criteria (discussed further). These participants were then randomly assigned to two groups (Figure 3):
Experimental group (n = 50): People in this group received the intervention. Control group (n = 50): People in this group did not receive the intervention.
These participants were selected from colleges in the state of Punjab.
Flowchart Showcasing the Procedure.
Inclusion Criteria
People who engaged in daily smoking, having six to eight cigarettes per day.
People falling in the age group 18–30 years old.
Exclusion Criteria
People who have any psychosomatic problem, or who are consultants in any psychiatry, or who are suffering from any mental disorders.
Tools
Beck’s Depression Inventory-II (BDI-II): The BDI-II is a 21-item self-report questionnaire developed by Aaron T. Beck (updated in 1996) to assess the severity of depressive symptoms based on DSM criteria. Each item is rated on a 4-point Likert scale (0–3), reflecting symptom intensity over the past two weeks, with total scores ranging from 0 to 63 (higher scores = greater depression severity). Interpretation: 0–13 minimal, 14–19 mild, 20–28 moderate, and 29–63 severe. It is widely used in clinical and research settings for screening, treatment planning, and monitoring progress. Still, it is not a diagnostic tool for major depressive disorder—only an indicator of symptom severity.30
Ryff’s Psychological Well-Being Scale (RPWB):31
Developed by Carol D. Ryff (2007), this 42-item questionnaire assesses PWB across six dimensions: self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth. Responses are rated on a 6-point scale (1–6), with 20 items reverse-scored. Higher scores indicate greater well-being. The scale measures overall positive functioning, reflecting how individuals perceive their purpose, personal development, relationships, and control over life circumstances (Figure 3).
Procedure
To examine this study, 100 individuals (n = 100), who reported smoking at least six to eight cigarettes per day (as the inclusion criteria says), were tested for depression scores and PWB scores for the post-test period as per Consort (Figure 2). After recording the scores, these people were randomly and equally divided into two groups: the control group (n = 50) and the experimental group (n = 50). One weak intervention—meditation—was provided to the experimental group, while none was provided to the control group. After one week, scores were again recorded for both groups separately using the same tools as applied earlier. They were calculated and analysed using SPSS 22 for descriptive analysis, paired t-tests, and independent t-tests.
Results
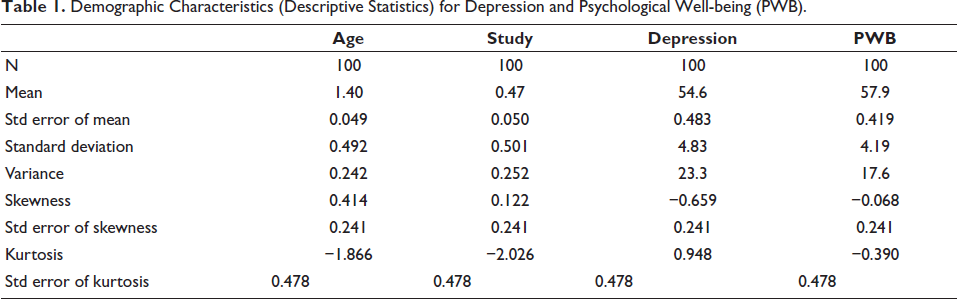
Demographic Characteristics (Descriptive Statistics) for Depression and Psychological Well-being (PWB).
A paired-samples t-test was conducted to examine the effect of the intervention on depression and PWB.
Table 2 shows that depression results indicated a statistically significant decrease in depression scores from pre-test (M = 54.36, SD = 4.91) to post-test (M = 28.10, SD = 6.05), t(49) = 24.70, p = .01. This result suggests that participants reported significantly lower levels of depressive symptoms following the intervention.
Paired Sample t-test Results for Depression and Psychological Well-being Scale (PWB) (Pre-test and Post-test).

Table 2 shows that the PWB scale results showed a statistically significant increase in well-being scores from pre-test (M = 57.50, SD = 4.91) to post-test (M = 65.88, SD = 4.94), t(49) = 9.96, p = .01. This indicates that participants experienced significantly higher levels of PWB after the intervention. Overall, these findings suggest that the intervention was effective in reducing depressive symptoms and enhancing PWB among participants.
An independent-samples t-test was conducted to compare post-intervention scores between the experimental and control groups for depression and PWB.
Table 3 and Figure 4 revealed that the depression the experimental group (M = 55.02, SD = 4.42) scored significantly lower than the control group (M = 28.10, SD = 6.05), F(1, 98) = 7.14, p = .05. This indicates that participants who received the intervention reported markedly fewer depressive symptoms compared to those in the control group.
Mean Scores for Depression and Psychological Well-being (PWB) in the Experimental and Control Groups.
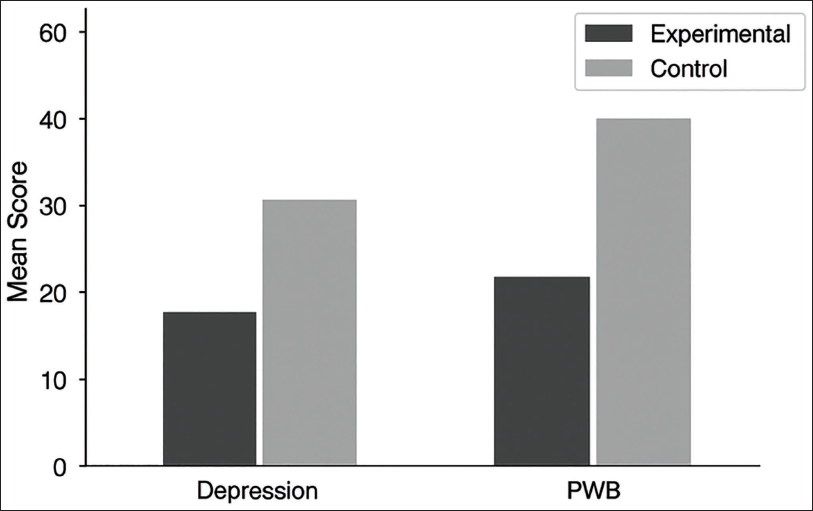
Independent Sample t-test Results for Post-intervention Depression and Psychological Well-being (PWB) Scores.

Table 3 showed that the PWB, the experimental group (M = 56.60, SD = 4.69), scored significantly higher than the control group (M = 65.88, SD = 4.94), F(1, 98) = 0.017, p = .05. This suggests that participants in the experimental group experienced greater PWB following the intervention. Overall, the results demonstrate that the intervention was effective in reducing depression and enhancing PWB, as evidenced by the significant differences between the experimental and control groups.
Discussion
The present study examined the effect of meditation on depression and PWB among individuals who are active daily smokers. Smoking is widely recognised as both a physical and mental health risk, associated with increased vulnerability to numerous health conditions, including cardiovascular diseases, respiratory disorders, and neurological complications. Beyond these physical consequences, smoking has been linked to adverse psychological outcomes, particularly depression and reduced PWB. The study’s primary objective was to determine whether meditation, as a structured intervention, could mitigate depressive symptoms and enhance PWB in smokers, thereby contributing to improved overall health outcomes. The use of both paired and independent-samples t-tests provided robust statistical evidence supporting the efficacy of meditation as a non-pharmacological intervention in this context.
Effects of Meditation on Depression
Biological, psychological, and social factors collectively contribute to the onset and persistence of depression. As outlined in the BPS Model, depression is often associated with hormonal imbalances, dysregulation in neurotransmitters, immune system dysfunction, and genetic predispositions. 25 Smokers may experience amplified biological vulnerabilities due to the effects of nicotine and other chemicals on the nervous and endocrine systems, which can further exacerbate depressive symptoms. Psychological factors, including maladaptive cognitive patterns, low emotional intelligence, and poor coping mechanisms, interact with social stressors such as trauma, interpersonal conflicts, and social isolation to reinforce depressive tendencies. 28
Meditation has emerged as an effective intervention capable of modulating these factors. This study found that participants in the experimental group exhibited significant reductions in depression scores after the meditation intervention. These findings align with previous research demonstrating the positive impact of meditation on depressive disorders. 33 Meditation enhances self-awareness, emotional regulation, and mindfulness, which collectively help individuals recognise and alter maladaptive cognitive and behavioural patterns. 34 By promoting relaxation and reducing physiological stress responses, meditation can counteract some of the biological processes implicated in depression, such as dysregulated cortisol secretion and inflammatory responses. 35
The high variability observed in post-test depression scores, indicated by a higher standard error, likely reflects individual differences in baseline psychological resilience, stress exposure, and engagement with the intervention. While meditation is broadly effective, its impact may be moderated by factors such as personality traits, temperament, or the presence of comorbid conditions. 36 Nonetheless, the overall trend supports the conclusion that meditation significantly alleviates depressive symptoms in daily smokers.
Effects of Meditation on PWB
PWB, as defined by the World Health Organization, encompasses emotional, cognitive, and social dimensions of life, including life satisfaction, purpose, autonomy, self-realisation, and the ability to manage stress effectively.26, 27 The present study demonstrates that meditation positively influences these dimensions, with participants in the experimental group showing significant improvements in PWB scores compared to the control group. This finding reinforces previous research that highlights the role of meditation in fostering self-development, emotional balance, and meaningful engagement in life. 37
Meditation promotes PWB by enhancing emotional regulation and self-efficacy, key components highlighted in the HBM. According to HBM, individuals are more likely to engage in health-promoting behaviours when they perceive susceptibility to health risks, understand the severity of potential outcomes, recognise the benefits of preventive actions, and believe in their ability to take effective steps (self-efficacy). 28 Meditation addresses these components indirectly by empowering individuals to adopt healthier coping strategies, manage stress, and cultivate mindfulness, which in turn fosters sustained engagement in positive health behaviours.
Moreover, PWB is not only influenced by internal factors but also by social interactions and environmental contexts. 38 Meditation can enhance interpersonal relationships by improving emotional intelligence, empathy, and communication skills. 39 Participants practicing meditation may experience reduced irritability, enhanced patience, and greater social connectedness, all of which contribute to overall well-being. In the context of smoking, these benefits are particularly relevant, as social support and healthy coping mechanisms are critical in reducing tobacco dependence and its associated psychological burden. 40
Meditation and Smoking Behaviour
The link between depression, reduced PWB, and smoking is well-established. Nicotine has transient mood-enhancing effects, leading some individuals to use smoking as a maladaptive coping strategy for stress and negative emotions. 10 However, smoking often exacerbates depressive symptoms and diminishes PWB over time.8, 9 Meditation offers a dual benefit by addressing both the psychological drivers of smoking and the associated depressive symptoms.
Previous studies have demonstrated the efficacy of meditation in reducing smoking frequency and promoting cessation. For instance, participants engaged in Transcendental Meditation (TM) sessions for two years showed a 51% complete cessation rate and a 30% reduction in tobacco intake, outcomes significantly better than those observed in control groups. 41 Meditation reduces common smoking triggers such as stress, cravings, and emotional reactivity, while simultaneously enhancing mindfulness and self-control. 40 These mechanisms allow individuals to recognise the habitual nature of smoking, interrupt automatic behaviours, and adopt healthier alternatives, such as relaxation or physical activity.
In the present study, the integration of meditation as an intervention not only improved psychological outcomes but also holds potential implications for smoking cessation strategies. Given the affordability and accessibility of meditation practices, individuals can engage in these exercises in their own homes, without requiring extensive resources or professional supervision. This practical advantage makes meditation an attractive complementary intervention for public health initiatives targeting smokers at risk of depression or reduced PWB.
Mechanisms Underlying Meditation’s Effects
The effectiveness of meditation can be explained through multiple mechanisms. Physiologically, meditation reduces activation of the hypothalamic-pituitary-adrenal (HPA) axis, leading to lower cortisol levels and decreased stress reactivity. 42 This is particularly important for smokers, as chronic stress is a significant predictor of both depressive symptoms and nicotine dependence. Neuroimaging studies have also shown that meditation enhances connectivity in brain regions associated with attention, self-regulation, and emotional processing, which can directly counteract depressive tendencies. 43
Psychologically, meditation fosters mindfulness, a non-judgemental awareness of the present moment, which allows individuals to recognise maladaptive thought patterns and disengage from automatic negative thinking. 44 This aligns with cognitive-behavioural principles, wherein changing maladaptive cognitions leads to improvements in mood and behaviour. Socially, meditation may encourage prosocial behaviours and empathy, enhancing the quality of interpersonal relationships and social support networks, which are protective factors against depression. 45
The BPS Model offers a comprehensive framework for understanding these mechanisms by emphasising the interplay among biological vulnerabilities, psychological processes, and social contexts.9, 46 Simultaneously, the HBM provides insight into why individuals adopt and maintain meditation practices, highlighting the importance of perceived risk, benefits, and self-efficacy in driving behaviour change. 28 Together, these frameworks explain how meditation can produce meaningful improvements in depression, PWB, and smoking-related behaviours.
Clinical Implications
The findings of this study have significant clinical implications. First, meditation can serve as a non-pharmacological intervention for depression, providing an accessible and cost-effective approach for individuals who may have limited access to conventional therapies. Second, the observed improvements in PWB indicate that meditation addresses broader aspects of mental health, including emotional regulation, self-efficacy, and life satisfaction. Third, by reducing triggers associated with smoking, meditation may support smoking cessation efforts and decrease the risk of tobacco-related diseases.
Healthcare providers can incorporate meditation into treatment plans for patients with comorbid depression and nicotine dependence, either as a standalone intervention or in combination with other therapeutic approaches, such as cognitive-behavioural therapy (CBT) or pharmacological treatment. Given the flexibility of meditation practices, patients can practice at home, adjusting the duration and frequency according to their lifestyle and preferences. This individualised approach enhances adherence and promotes long-term behavioural change.
Limitations and Future Research
Despite the promising results, this study has several limitations. First, the higher standard error in post-test data indicates variability in participant responses, which may be influenced by unmeasured factors such as personality traits, life stressors, or the severity of nicotine dependence. Future research should consider stratifying participants based on these variables to understand differential effects better.
Second, the study focused exclusively on daily smokers, which may limit the generalizability of the findings to other populations, such as occasional smokers, individuals with other substance use disorders, or those with severe psychiatric conditions. Third, while the study employed validated measures of depression and PWB, self-reported data are inherently subject to bias, including social desirability and recall inaccuracies. Incorporating physiological markers of stress and mood, such as cortisol levels or heart rate variability, could provide more objective evidence of meditation’s effects.
Future studies should also explore the long-term effects of meditation, including whether improvements in depression, PWB, and smoking behaviour are sustained over months or years. Investigating the optimal types, durations, and frequencies of meditation practices for specific populations would further enhance the practical application of these interventions. Finally, research examining the integration of meditation with other evidence-based interventions, such as mindfulness-based cognitive therapy (MBCT) or contingency management for smoking cessation, could provide insights into synergistic treatment approaches.
Conclusion
Concluding the findings of this research, which supports the notion that meditation has a highly positive effect on reducing depression and increasing well-being among the population of people who are active smokers. The results observed in the pre-test and post-test design based upon comparisons between the experimental and the control groups mark the potential of meditation as a rightful and valuable practice. Future research should investigate the long-term benefits and underlying mechanisms of meditation and pay attention to improving the overall well-being and quality of life of people suffering from depression, and also for people who engage in daily smoking.
Footnotes
Abbreviations
ICD-10: International Classification of Diseases, 10th edition
BDI-II: Beck Depression Inventory–II
PWB: Psychological well-being
HBM: Health Belief Model
BPS: Biopsychosocial
DSM: Diagnostic and Statistical Manual of Mental Disorders
N: Number of participants
M: Mean
SD: Standard deviation
df: Degrees of freedom
SE: Standard error
MBCT: Mindfulness-Based Cognitive Therapy
Acknowledgements
The authors thank all participants for their participation in the study. They express gratitude to their friends and family for their encouragement and support. The authors are grateful to all participants for enabling the researcher to conduct the study. They also appreciate their friends and family’s encouragement and support.
Authors’ Contribution
The final article has been reviewed and approved by all authors involved in the study’s conception and design.
Statement of Ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki, approved by the Ethics Committee of Lovely Professional University, Punjab, and registered with the Clinical Trials Registry – India (CTRI) LPU/IEC-LPU/2024/1/28, Date 01.04.2024.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ICMJE Statement
This manuscript complies with ICMJE guidelines.
Patient Consent
Participants provided written informed permission to participate in the study.