
Abstract
Background
Anxiety disorders are increasingly recognized as involving neurocognitive impairments in executive functioning, including working memory, inhibitory control, and cognitive flexibility. However, Indian research has predominantly emphasized emotional and behavioural manifestations, leaving the neuropsychological correlates of anxiety severity underexplored.
Purpose
To investigate the relationship and differences in executive functioning among individuals with varying levels of anxiety.
Method
A cross-sectional study was conducted with 60 patients, classified into mild, moderate, or severe anxiety using the PROMIS Anxiety–Adult Short Form. Neuropsychological assessment included the Wechsler Memory Scale (WMI), Stroop Test (inhibitory control), and Wisconsin Card Sorting Test (conceptual processing). Data were analysed using ANOVA, post hoc comparisons, chi-square tests, Pearson’s correlations, and linear regression. Ethical approval and informed consent were obtained.
Results
Significant group differences emerged across all domains (WMI: F = 6.87, p = .002; Stroop: F = 13.09, p < .001; WCST: F = 17.72, p < .001). Post hoc tests showed superior performance in the mild group relative to moderate and severe groups, with no significant differences between the latter two. Anxiety severity correlated negatively with executive functioning (r = −0.45 to –0.61, p < .01). Regression analyses confirmed severity as a significant predictor, explaining 20%–37% of variance in executive performance.
Conclusion
Executive dysfunction worsens with increasing anxiety severity, with cognitive decline plateauing between moderate and severe levels. Strong correlations highlight severity as a critical determinant of working memory, inhibitory control, and conceptual processing. Findings underscore the need to integrate neuropsychological assessment and cognitive rehabilitation into anxiety management in Indian clinical settings.
Keywords
Introduction
Anxiety disorders are among the most prevalent mental health conditions worldwide, with a global prevalence of approximately 301 million people in 2019. 1 The COVID-19 pandemic further exacerbated this burden, contributing to a 25% rise in anxiety cases in just one year. 1 These disorders are characterized not only by excessive worry and emotional distress but also by significant cognitive dysfunctions, particularly in domains of executive functioning such as working memory, inhibitory control, and cognitive flexibility. Such impairments reduce adaptive decision-making and problem-solving abilities, thereby worsening functional outcomes and quality of life.2, 3
In India, the burden of anxiety disorders is particularly high. Epidemiological studies report prevalence estimates ranging from 3.9% (using stringent diagnostic criteria) to 15.9% (using broader screening measures), with urban youth being especially vulnerable.4, 5 Despite this, Indian research has traditionally focused on the emotional and behavioural manifestations of anxiety, while the neuropsychological underpinnings remain underexplored. This gap hampers the development of culturally tailored cognitive rehabilitation strategies.
Neurobiological evidence supports the role of executive dysfunction in anxiety disorders. Neuroimaging studies consistently report hyperactivity in limbic regions such as the amygdala and hypoactivity in prefrontal regions, including the dorsolateral prefrontal cortex (DLPFC), which is central to executive control processes.6, 7 Disrupted connectivity between these networks contributes to impaired top-down regulation of emotional responses. Theoretical models such as the Attentional Control Theory (ACT) 2 and the Dual-Competition Model 8 further explain how anxiety consumes attentional resources, reduces working memory capacity, and heightens inhibitory control deficits.
Executive functioning encompasses a cluster of higher-order processes essential for adaptive behaviour. Among these, three domains are particularly relevant to anxiety:
These impairments are not merely secondary symptoms but may represent vulnerability factors that precede the onset of anxiety disorders. 12 Moreover, they influence treatment outcomes. For example, deficits in inhibitory control and conceptual processing can reduce the effectiveness of cognitive-behavioural therapy (CBT), while targeted neurocognitive training has shown potential to enhance therapeutic gains. 13
Despite growing transnational evidence, studies differentiating executive function performance across severity levels of anxiety are limited, particularly in the Indian population. Some research suggests that moderate anxiety may not differ significantly from severe anxiety in terms of executive deficits, indicating a plateau effect. 14 Clarifying this relationship has clinical implications, as it can inform individualized treatment planning and the integration of cognitive rehabilitation into standard care.
The present study was therefore designed to examine executive functioning specifically working memory, inhibitory control, and conceptual processing across mild, moderate, and severe anxiety groups in an Indian clinical sample. By addressing this gap, the study aims to provide empirical evidence for incorporating neuropsychological assessments into routine anxiety management and to contribute to culturally relevant interventions.
Methods
Participants
The study sample comprised 60 participants (aged 18–50 years) recruited purposively from the outpatient department of the Hospital for Mental Health, Ahmedabad. Participants were divided into three groups, that is, mild, moderate, and severe anxiety, based on their scores on the PROMIS Anxiety–Adult Short Form. Each group included 20 participants.
Inclusion and Exclusion Criteria
Inclusion Criteria
Aged 18 to 50 years,
Individuals who scored the raw score of 16 (t-score 55) and above on the PROMIS Anxiety-Adult Short Form,
Ability to read and understand the instructions and,
Provision of informed consent.
Exclusion Criteria
History of major psychiatric illness other than anxiety disorders (e.g., psychosis, bipolar disorder),
Neurological conditions such as epilepsy, head injury, or dementia,
Have severe visual impairment (uncorrected), colour blindness, or other vision related conditions and,
Having history and/or current use of psychoactive substance(s).
A sample size of 60 was selected in line with comparable neuropsychological studies in Indian clinical population.
Tools
Procedure
After obtaining institutional ethics clearance, eligible participants were screened and stratified by anxiety severity using the PROMIS scale. Each participant was assessed individually in a quiet clinical setting in one session of approximately 45 minutes each. Neuropsychological tools were administered in a fixed order: WMS-IV (WMI), Stroop, and WCST. Standard administration and scoring protocols were followed for all instruments.
Sociodemographic details (age, gender, education, religion, occupation, socio-economic status) were also collected. Clinical demographic details (first onset of illness and duration of illness) were also collected. Confidentiality and anonymity were maintained throughout.
Statistical Analysis
Data were analysed using SPSS version 27.0. Descriptive statistics (mean, standard deviation, frequencies) were calculated. One-way ANOVA was used to test group differences across mild, moderate, and severe anxiety categories for WMI, Stroop interference, and WCST conceptual level. Post hoc Tukey’s HSD tests were applied where significant effects were found. Pearson’s correlations were conducted to examine associations between anxiety severity and executive function measures. Finally, linear regression analyses were performed to test anxiety severity as a predictor of working memory, inhibitory control, and conceptual processing.
Results
Discussion
The present study examined executive functioning across different levels of anxiety severity in an Indian clinical sample, with a focus on working memory, inhibitory control, and conceptual processing. The findings demonstrated significant impairments in all three domains, with increasing anxiety severity associated with poorer performance. However, a plateau effect was evident, whereby the magnitude of impairment stabilized at moderate levels, with severe anxiety not always showing proportionately greater deficits.
Sociodemographic and Clinical Comparisons
The socio-demographic characteristics of participants across mild, moderate, and severe anxiety groups are presented in Table 1, in which, significant associations were observed between anxiety severity and both educational attainment and socioeconomic status (SES). Participants with higher education were overrepresented in the mild group, while lower education levels were concentrated in the moderate and severe groups. This supports prior evidence that education offers protection against anxiety through improved coping, economic security, and greater mental health literacy.19, 20 Similarly, lower SES participants were disproportionately represented in the severe group, consistent with findings that economic disadvantage and poor access to resources elevate risk for anxiety disorders.21–23
Other demographic variables such as age, religion, and occupation were not significantly associated with severity. Gender showed a non-significant trend, with more females in the mild and moderate groups, echoing earlier reports of greater help-seeking among women. 24
As depicted in Table 2, clinical characteristics related to the onset and duration of illness varied across anxiety severity levels. Clinically, first-onset cases were predominant in the mild group, while recurrent illness was more common in the moderate and severe groups. This suggests that chronicity and recurrence are linked with greater severity, as shown in prior studies of anxiety progression and disability.25, 26 Illness duration, however, did not differ significantly across groups, possibly reflecting recall biases or underestimation of chronicity in anxiety disorders.27, 28 In the Indian context, stigma and low mental health literacy may further contribute to delayed recognition and treatment.29, 30
Socio-demographic Details of the Sample.
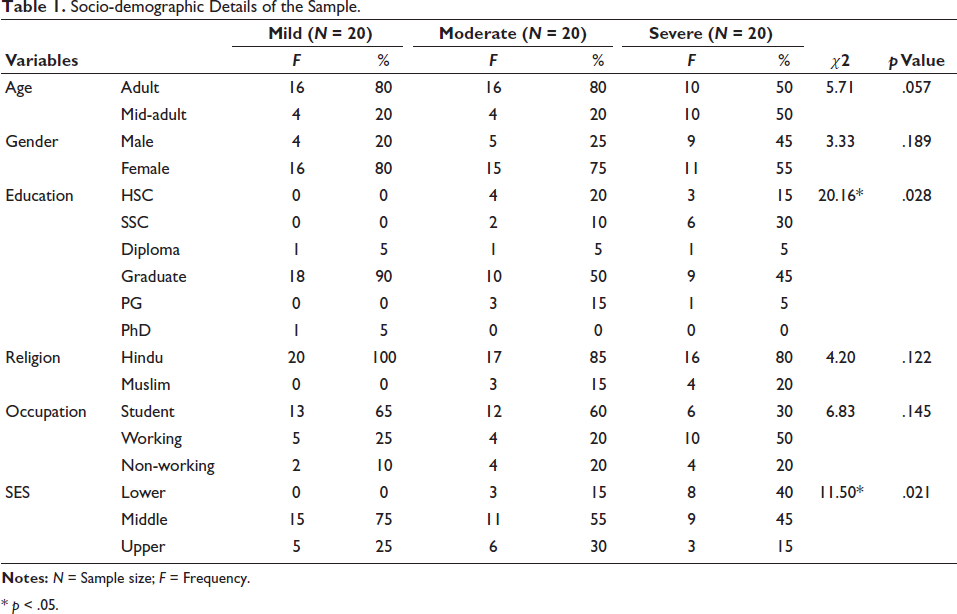
* p < .05.
Clinical Demographic of the Sample.
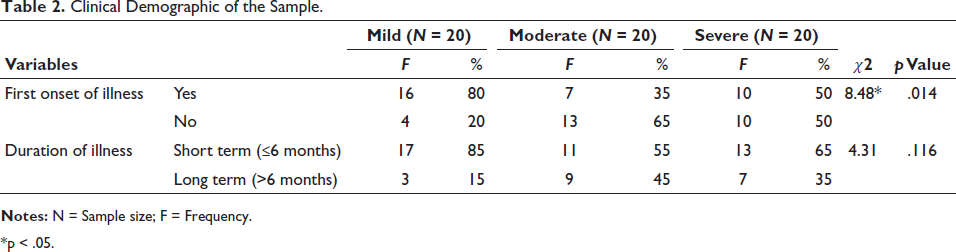
*p < .05.
Taken together, these findings highlight the role of education, socioeconomic factors, and illness recurrence in shaping anxiety severity, reinforcing the need for early intervention and public health strategies that address structural vulnerabilities.
Group Level Differences
ANOVA results (Table 3) indicated significant differences across anxiety groups in all domains of executive functioning. Working memory, as measured by the WMS-IV WMI, showed the most pronounced decline with severity. This finding is consistent with Eysenck and Derakshan’s Attentional Control Theory, 31 which proposes that anxiety consumes limited working memory capacity due to intrusive threat-related cognitions. Similar deficits have been observed in both clinical and subclinical populations, suggesting that working memory may represent a core vulnerability factor for anxiety.9, 32, 33
One-way ANOVA Results for Executive Functioning.
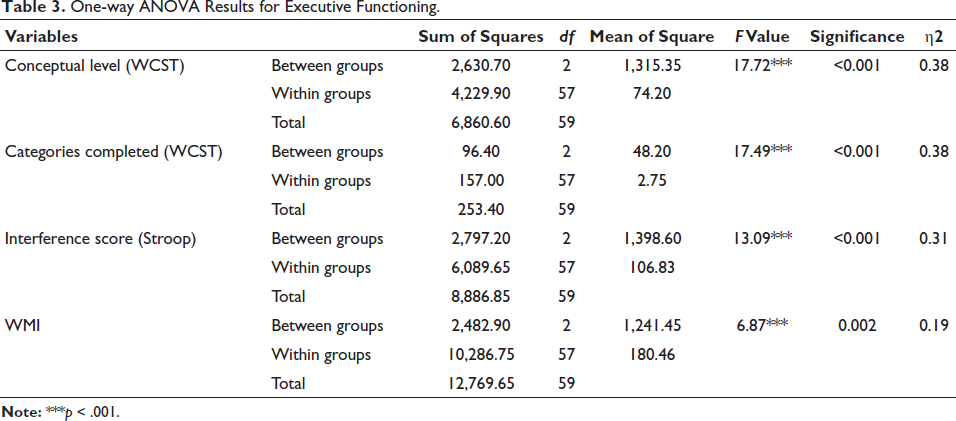
Inhibitory control, assessed through Stroop interference, also declined significantly across severity groups. This aligns with prior evidence showing that anxiety impairs the ability to suppress prepotent responses and disengage from threatening stimuli. 11 Chamberlain et al. 10 highlighted inhibitory control deficits as an endophenotypic marker for anxiety-related psychopathology, a view supported by the present findings.
Conceptual processing, indexed by WCST performance, was significantly poorer among higher-severity groups. This suggests impaired cognitive flexibility and increased perseveration, consistent with earlier work linking anxiety to rigid, rumination-prone thinking styles.12, 13 These results collectively reinforce the conceptualization of executive dysfunction as a broad cognitive correlate of anxiety. 30
Post Hoc Patterns and Plateau Effect
Post hoc comparisons (Table 4) revealed that severe anxiety groups performed significantly worse than mild groups across domains, but differences between moderate and severe groups were smaller or non-significant. This supports the notion of a cognitive plateau effect across executive functions.
Post Hoc Comparisons of Executive Functioning Across Anxiety Severity Levels.
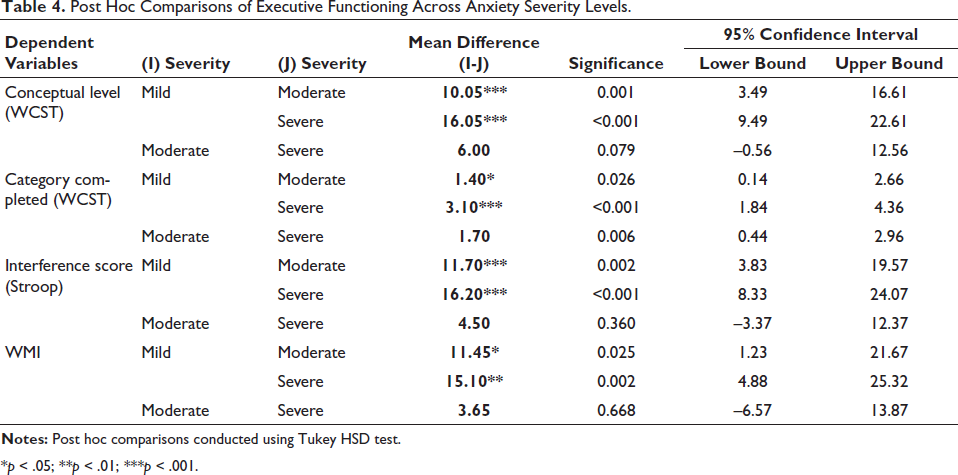
*p < .05; **p < .01; ***p < .001.
Similar patterns have been reported by Lisica et al.14, 32 who found that executive dysfunction does not always increase linearly with anxiety severity. Ansari and Derakshan31, 34 demonstrated that neural correlates of inhibitory control deficits in anxiety reach a saturation point, suggesting compensatory mechanisms collapse once a certain threshold of severity is reached.
The plateau effect observed here may reflect the exhaustion of cognitive control resources. At mild levels of anxiety, compensatory prefrontal activation may help maintain performance, but by moderate severity, these reserves are fully engaged, producing measurable deficits. At severe anxiety, the system may already be at or near floor levels of functioning, leaving little room for further deterioration. Clinically, this indicates that executive dysfunction is a core feature of anxiety that emerges early, not just in the most severe cases.
Performance Distribution
Chi-square analyses (Table 5) on WCST scores of participants showed a disproportionately higher number of low-performance cases in the severe anxiety group compared to the mild and moderate groups. This categorical approach provides convergent evidence for the dimensional findings. While ANOVA captured group means, chi-square analysis demonstrated that the distribution of poor performers was heavily skewed toward severe anxiety, reinforcing the clinical significance of executive dysfunction in this population. Such convergent results are particularly compelling, as they reduce the likelihood that findings are due to chance or statistical artifact.
Chi-square Distribution of Performance Levels Across Different Levels of Anxiety on WCST.
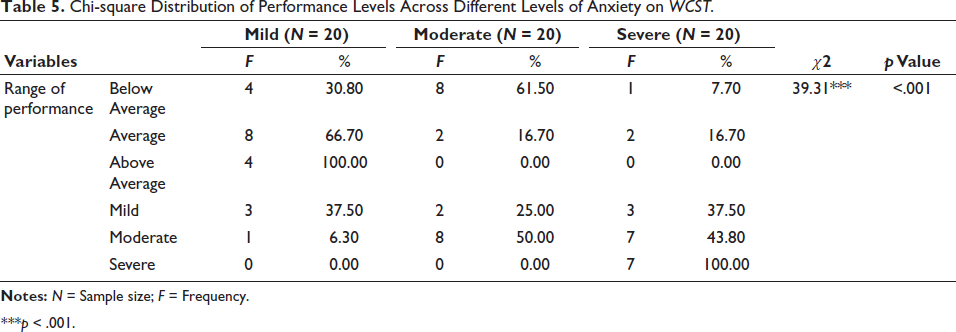
***p < .001.
Correlation Findings
Pearson’s correlations (Table 6) revealed strong negative associations between anxiety severity and executive function performance. Conceptual processing showed the strongest correlation (r = −0.61), closely followed by inhibitory control (r = −0.59), while working memory was moderately correlated (r = −0.45). These results confirm that anxiety severity has a measurable impact across executive domains, with variability in strength of associations.
Correlation Between Executive Functioning and Anxiety Severity Levels.

Although working memory showed the weakest association in the present sample, previous meta-analytic evidence highlights it as the most consistently impaired domain in anxiety, likely due to intrusive threat-related cognitions consuming attentional resources. 9 Moran’s findings, together with evidence of inhibitory deficits in anxiety and related disorders, 10 suggest that different executive processes may be vulnerable through partly distinct mechanisms. The relatively stronger association with conceptual processing in this study may also reflect cultural or sample-specific factors, or the plateau effect, whereby cognitive flexibility deficits manifest prominently once anxiety reaches moderate-to-severe levels.
Together, these findings point to both domain-general impairment across executive functions and domain-specific vulnerabilities, reinforcing the importance of comprehensive cognitive assessment in anxiety.
Predictive Role of Anxiety Severity
Regression analyses (Table 7) established anxiety severity as a significant predictor of executive dysfunction, explaining 37% of the variance in conceptual processing, 34% in inhibitory control, and 20% in working memory. These findings indicate that executive dysfunction is not incidental but integral to the cognitive profile of anxiety, in line with meta-analytic reviews reporting broad EF impairments in anxiety and related disorders. 35
Linear Regression Analysis Predicting Executive Functioning from Severity.

The particularly strong predictive effect on conceptual processing and inhibitory control highlights the role of anxiety in diminishing cognitive flexibility and attentional control, processes known to depend on prefrontal regulation.8, 36 While working memory accounted for a smaller proportion of variance in this sample, prior meta-analytic work has consistently identified it as the most reliable domain of impairment across anxiety disorders. 9 This discrepancy may reflect sample-specific characteristics or cultural differences in cognitive style.
Clinically, these results underscore the importance of neuropsychological assessment in anxiety. Executive deficits, particularly in flexibility and inhibition, have been shown to predict poorer outcomes with cognitive-behavioural therapy, while targeted cognitive remediation has demonstrated additive benefits. 13 Incorporating EF screening into clinical pathways may therefore help tailor interventions to patient cognitive profiles.
Neurobiological Interpretation
The observed impairments are consistent with neurobiological models of anxiety that emphasize disrupted prefrontal limbic connectivity. Functional neuroimaging shows that anxiety is associated with hyperactivity in the amygdala and hypoactivity in dorsolateral prefrontal cortex (DLPFC) regions.6, 7 This imbalance undermines top-down regulation, resulting in diminished executive control over emotional responses.
Working memory deficits may stem from inefficient DLPFC recruitment, while inhibitory control impairments may reflect compromised anterior cingulate cortex (ACC) function, which is critical for conflict monitoring.8, 34 The plateau effect observed here can also be explained neurobiologically: compensatory prefrontal activation may sustain performance until moderate anxiety, after which these mechanisms collapse, leading to a ceiling effect on deficits.
Clinical and Cultural Implications
The findings underscore the importance of incorporating neuropsychological assessment into routine clinical evaluation for anxiety disorders. Deficits in inhibitory control and flexibility may reduce the effectiveness of CBT, which depends on attentional shifting and cognitive restructuring. 14 Identifying these impairments early could allow clinicians to adapt therapy by integrating attention-control training or working-memory-enhancing tasks.
For India, the present study fills a gap in the literature, as most local research has focused on emotional or behavioural symptoms rather than cognitive underpinnings.2, 3 By demonstrating executive dysfunction across severity levels, this study advocates for culturally tailored interventions that address cognitive deficits alongside symptom reduction.
Strengths and Limitations
A major strength of this study is its comprehensive assessment of executive functioning using multiple validated neuropsychological tools, including the WMS-IV, Stroop, and WCST, which together capture working memory, inhibitory control, and conceptual processing. The study also contributes culturally specific evidence by focusing on an Indian clinical population, where research on cognitive aspects of anxiety remains limited. Another strength lies in the use of diverse statistical approaches ANOVA, post hoc testing, chi-square analyses, correlations, and regression which provide convergent evidence for the observed findings and enhance the robustness of conclusions.
At the same time, certain limitations must be acknowledged. The modest sample size (N = 60) and the cross-sectional design prevent causal inference regarding whether executive deficits precede or result from anxiety severity. Furthermore, neuroimaging data were not collected, which would have allowed direct testing of the neural mechanisms hypothesized to underlie the observed impairments.
Future Directions
Future research should employ larger, community-based, and longitudinal designs to clarify the trajectory of executive dysfunction in anxiety. Neuroimaging studies could directly test whether prefrontal compensatory mechanisms account for the plateau effect. Intervention trials should examine whether cognitive training can remediate executive deficits and enhance treatment response, particularly when initiated at moderate severity levels.
Conclusion
This study provides convergent evidence that executive dysfunction is closely linked to anxiety severity in an Indian clinical population. Findings from ANOVA, post hoc, chi-square, correlation, and regression analyses consistently indicate impairments in working memory, inhibitory control, and conceptual processing, with evidence of a plateau effect across domains. These results highlight the importance of early neuropsychological assessment and support the integration of cognitive rehabilitation strategies into culturally adapted anxiety treatment protocols.
Footnotes
Authors’ Contribution
All authors contributed to the study’s conception and design of the study. All authors read and approved the final manuscript.
Statement of Ethics
Approval was granted by the Ethics Committee of Hospital for Mental Health (HMH), Ahmedabad.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ICMJE Statement
The manuscript complies with ICMJE guidelines.
Patient Consent
Written informed consent was obtained from all participants prior to their inclusion in the study. Participants were informed about the nature and purpose of the study, voluntary participation, and confidentiality of their data.