
Abstract
Background
Attention deficit hyperactivity disorder (ADHD) is a prevalent neurodevelopmental disorder characterised primarily by inattention, hyperactivity, and impulsiveness with associated impairments related to sensory processing and motor coordination, and attributed to abnormalities in the brain areas responsible for sensory-motor integration and cognitive control. The symptoms may persist until adulthood, impacting various aspects of life. Traditional treatment and pharmacological approaches chiefly target behavioural aspects, highlighting the need to address sensory, motor, and cognitive issues via an integrative approach.
Purpose
This study aims to determine the effect of a multi-modal exercise programme on improving cognitive, sensory, and motor function among children with ADHD.
Methods
The study will be a randomised controlled trial involving 60 children diagnosed with ADHD, aged 6–12 years. Children will be randomly allocated to either the intervention group or the control group. Both groups will be subjected to a 45-minute therapy session four times a week for eight weeks. The intervention group will receive sensory, motor and cognitive training, and the control group will receive standard care. Outcomes Paediatric Balance Scale (PBS), Short Sensory Profile (SSP), Trail Making Test, and Developmental Coordination Disorder Questionnaire 2007 will be analysed at baseline, two weeks, four weeks, and at the end of the eight-week training programme.
Results
It is anticipated that an integrative training approach among the intervention group, will concurrently address the underlying neurodevelopmental deficits and improve sensory, motor, and cognitive functions instead of focusing solely on symptom management among children with ADHD.
Conclusion
Incorporating sensory, motor, and cognitive training offers a promising supplementary approach in ADHD management. The multimodal stimulation of neural circuits will serve to improve core functions and promote more adaptive behaviours.
Trial Registration
This prospective trial has been successfully registered with the Clinical Trial Registry of India with registration number (CTRI/2025/05/086742).
Introduction
Attention deficit hyperactivity disorder (ADHD), a condition marked by inattention, hyperactivity, and impulsivity, affects 5%–8% of children worldwide. 1 Children with ADHD often face challenges with motor coordination and sensory processing, making it harder for them to learn and carry out motor-related activities effectively, which can affect their balance, coordination, fine and gross motor skills, and ability to perform everyday tasks. These difficulties can have lasting effects on their personal lives, social interactions, and academic performance.2, 3
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, defines ADHD as a condition where the symptoms persist for at least six months and are severe enough to interfere with daily activities, academic performance, or social interactions. 4 Importantly, research shows that about 50% of children with developmental coordination disorder also meet the criteria for ADHD. 5
Neuroimaging studies have revealed differences in the structure and function of certain parts of the brain in people with ADHD compared to people without the disorder. Specifically, abnormalities were found to be related to the cerebellum, activity and connectivity of the prefrontal cortex, and differences in the size and shape of the basal ganglia.6–8 There is a favourable association between somatosensory discrimination and motor planning, motor learning, and motor abilities, as demonstrated by the various studies that have shown the sensory processing differences in children with ADHD. 9 It has been demonstrated that reduced cognitive functioning is associated with delayed acquisition of motor skills and movements needed for activities of daily living (ADLs). 10 In addition, compromised sensory integration affects the ability to process and respond appropriately to sensory stimuli. Given the complex nature of ADHD and its wide-ranging effects, early detection and targeted treatments are crucial. 11 Pharmacological interventions mostly aim to target the core symptoms associated with symptom reduction and behaviour compliance. However, their long-term use is associated with side effects, including potential cardiovascular risks, and does not address the functional limitations associated with the disorder. 12
Investigation on how children with ADHD’s motor skills link to their social and cognitive abilities suggests that issues with cognition obstruct the development of motor skills. 13 This connection between cognitive deficits and motor impairments underscores the interconnectedness of these areas, highlighting the importance of a comprehensive understanding of the disorder and the development of evidence-based interventions for children with ADHD. 14 Interrelatability in deficiencies related to perception, motor control, and attention requires a multimodal approach that addresses cognitive, sensory, and motor challenges in a coordinated way to improve both functional abilities and quality of life for children with ADHD. Early detection and intervention using such a treatment strategy will allow for more personalised, effective treatment that supports children’s development from an early stage and helps prevent long-term negative outcomes. Despite the growing body of research, there remains a gap in standardised protocols and robust evidence regarding the combined impact of such interventions. This study seeks to contribute to the evolving understanding of multimodal interventions and their role in reshaping clinical practice and educational support for children living with this complex condition. Given this context, the present study aims to explore the need for and efficacy of an integrative training approach that concurrently targets sensory, motor, and cognitive domains in children with ADHD. By addressing the underlying neurodevelopmental deficits rather than merely managing symptoms, such an approach may offer a more holistic and sustainable strategy for enhancing the functional outcomes and quality of life for individuals with ADHD.
Methods
Ethical Approval
This study is a two-group, pretest-posttest design, randomised controlled trial targeting children with ADHD. The study protocol was approved by the Research Ethics Committee of the School of Allied Health Sciences, Galgotias University (Ref. no. SEC/SAHS/PHD/24/10). This prospective trial has been successfully registered with the Clinical Trial Registry of India (acknowledgement number REF/2025/04/103647) and obtained trial registration number (CTRI/2025/05/086742) on 13 May 2025. The study will be conducted per the ethical principles for medical research involving human subjects outlined in the Declaration of Helsinki (revised 2013) and the Indian Council of Medical Research National Ethical Guidelines for Biomedical and Health Research Involving Human Participants (2017).15, 16 This FOCUS protocol document is identified as version 1.0, dated 9 January 2025, reflecting all amendments and updates as of this date. Any further updates will be systematically documented with new version numbers and dates, as required.
Compliance with Ethical Standards
The protocol is prepared following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 guidelines, which offer an evidence-based framework to ensure that all essential scientific, ethical, and methodological aspects of the trial are thoroughly addressed.
17
Additionally, this protocol has been formally submitted for registration with the Copyright Office, Government of India, with a unique diary number 11478/2025-CO/L (
Study Setting and Design
To evaluate the effect of the FOCUS protocol trial, this study will adopt a two-group, pre-test-post-test design and will be conducted in a teaching hospital with a physiotherapy outpatient department located in Dehradun, Uttarakhand, India and equipped with standardised facilities and appropriate infrastructure to carry out the trial effectively. The children will be randomly assigned to either the intervention group or the control group. Baseline assessments (pretest) will be conducted for all children before the intervention, followed by post-intervention assessments (posttest), enabling within-group and between-group comparisons to evaluate the proposed outcomes and assess the effect of the intervention.
Eligibility Criteria
The inclusion criteria are as follows: Girls and boys aged 6–12 years with a clinical diagnosis of ADHD; cooperation in understanding and performing tasks as determined by the Modified Mini-Mental Scale for Cognitive Function in Children. Inclusion will be based on obtaining informed consent from both the parent or guardian and the child participant. The following will be excluded from the study: Children who have undergone recent surgical procedures; those with visual or auditory impairments; associated birth defects and congenital anomalies; diagnosed neurological disorders and systemic diseases other than ADHD; and any physical deficits leading to motor disorders.
Randomisation, Allocation and Blinding
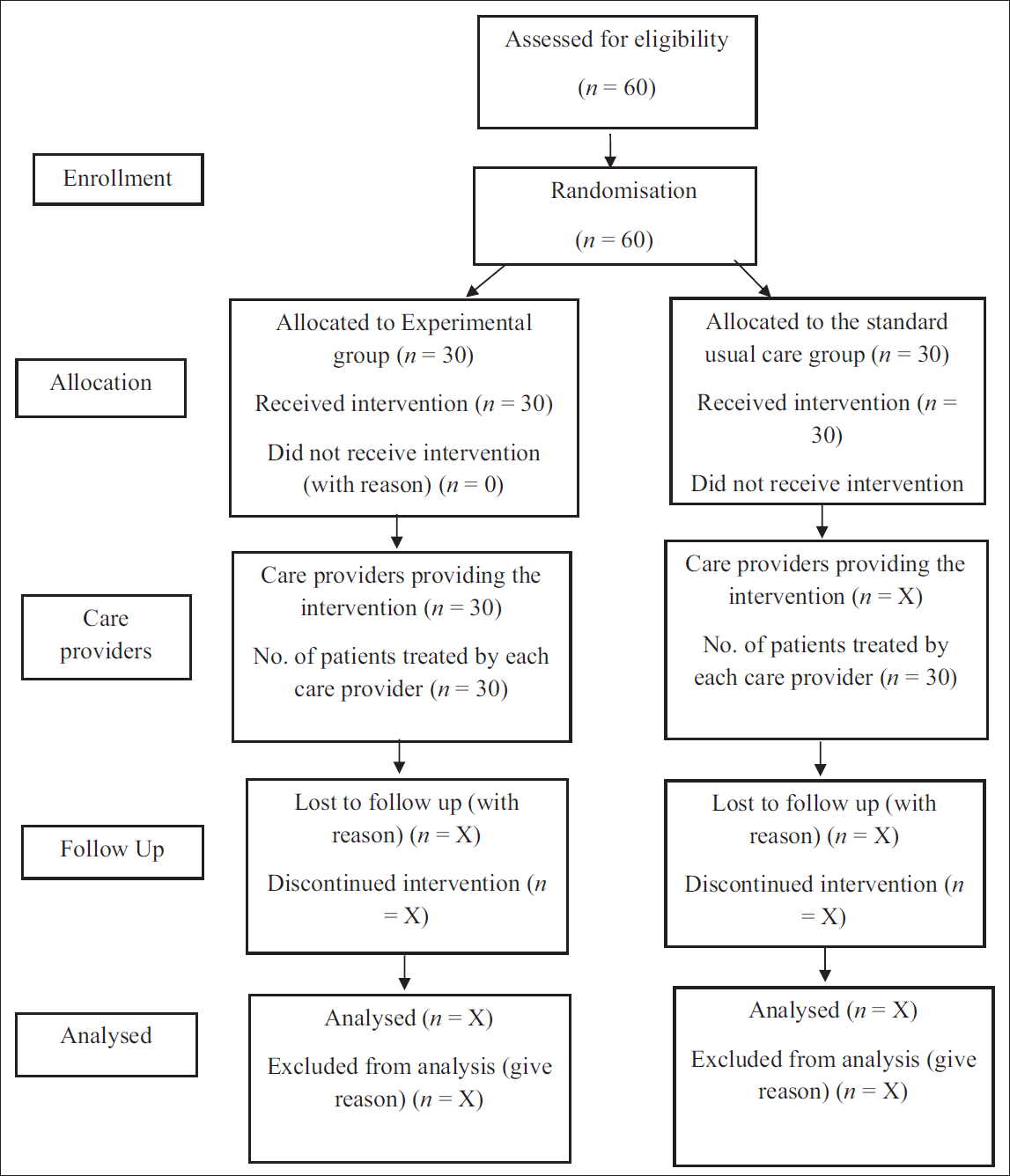
Children will be randomised to the sensory, motor and cognitive training group and the standard care group. A computer-generated random number table employing the block randomisation method will be administered. To ensure allocation concealment, sequentially numbered, sealed, opaque envelopes will be used. Children will be randomly assigned to either the intervention or control group based on the generated sequence. Both children and outcome assessors will be blinded to group allocation to minimise performance and detection bias. The physiotherapist administering the intervention will not be blinded; however, they will not be involved in outcome assessments. Unblinding will be permitted only in cases involving medical emergencies or adverse events, only after consulting the principal investigator. The schematic Consolidated Standards of Reporting Trials flow chart for the study protocol is displayed in Figure 1.
Proposed Consolidated Standards of Reporting Trials (CONSORT) Flow Chart for Non-pharmacological Intervention. 29
Sample Size Estimation
The sample size was calculated using the Systat 13.2 Software, and was 60 (30 in each group).
Recruitment, Enrolment, and Baseline Measurements
Eligible children who meet the selection criteria will be included in the study after obtaining informed consent. The enrolment will be conducted over 10 months, ensuring adequate time to complete the assessment. Baseline characteristics of each patient will be determined through a standardised assessment proforma, including demographic details. Children in both groups will participate in an eight-week training programme.
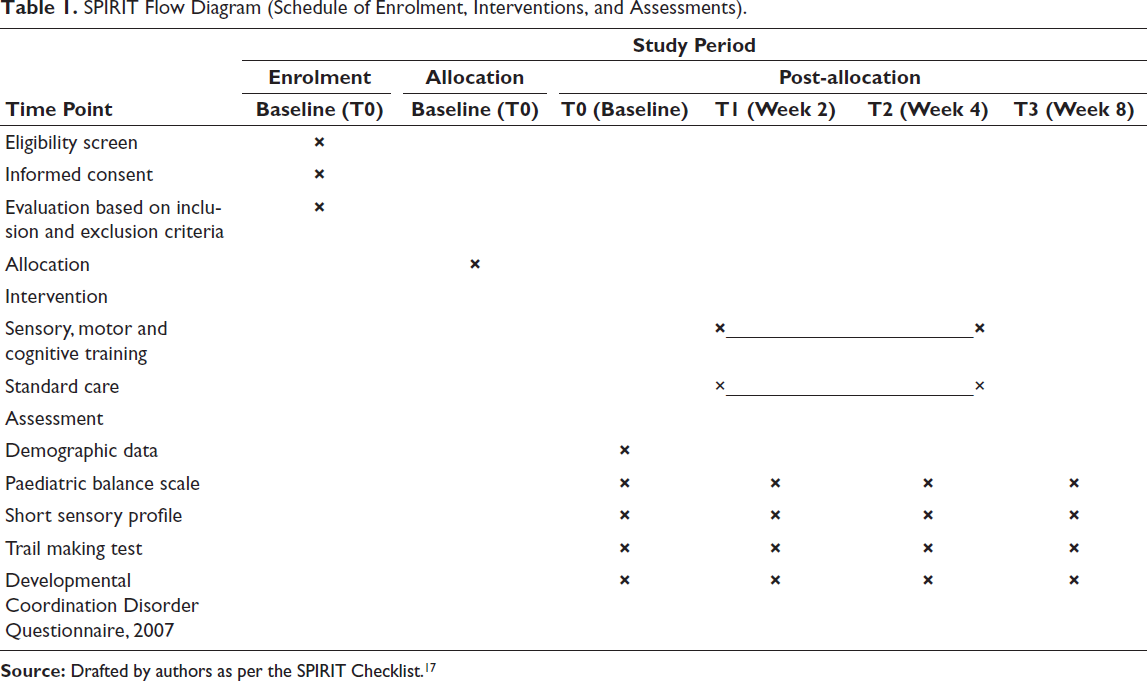
Patient participation schedules for the trial will be determined as per Table 1.
SPIRIT Flow Diagram (Schedule of Enrolment, Interventions, and Assessments).
Procedure
After meeting the selection criteria and obtaining baseline measures, children will be randomly assigned to the intervention group and the control group. The therapy will be administered as four sessions per week over eight weeks, with each session lasting approximately 45 minutes.
Intervention Group (Sensory, Motor and Cognitive Training Group)
Children in this group will receive a self-designed, structured therapy programme based on a multimodal approach incorporating sensory, motor, and cognitive therapeutic components to address different aspects of the needs of children with ADHD. Each component of the intervention will follow a planned progression schedule, with modifications implemented once every two weeks. Table 2 illustrates the intervention group (sensory, motor and cognitive) training protocol.
Protocol for Sensory-motor and Cognitive Training.

Control Group (Standard Care Group)
The standard care provided to participants will include: Range of motion exercises, aerobic training, strength and balance training, along with relaxation techniques, administered for the same duration.
Protocol Adherence and Discontinuation
The intervention will be performed under the supervision of a skilled physiotherapist. To enhance adherence to the intervention protocol, strategies such as scheduling sessions at similar timings and educating parents or guardians on the benefits of completing all scheduled sessions to maximise therapeutic effect will be incorporated. Adherence to the intervention will be monitored through structured attendance logs and a checklist to document the completion of prescribed activities during every session. Any missed sessions from the protocol will be recorded systematically. Rest periods will be allowed, as required, to ensure sustained engagement of the child throughout the session and prevent feelings of being overwhelmed. In case of adverse events, involving exercise-induced cardiovascular symptoms or worsening of behavioural symptoms, intervention will be subject to discontinuation. The emergence of any psychiatric conditions that are contradictory to exercise participation, repeated non-compliance with therapy sessions despite reminders, will also necessitate discontinuation from the therapy. Parents or guardians can withdraw their consent at any stage during the therapy. Participation in any other structured training or consumption of unprescribed cognitive-enhancing supplements will be prohibited to avoid confounding effects.
Outcome Assessment
Following a baseline assessmnt, follow-up assessments for the outcome measures will be repeated after two weeks, four weeks, and at the end of the training programme (eighth week), to determine both short and long-term impact. The assessors will be trained physiotherapists, acquainted with the use of the included outcome measures tools. All the assessments will involve blinded assessors, not involved in the delivery of intervention throughout the therapy, and will have no access to the intervention data. Any accidental unblinding will be immediately reported to the principal investigator and reassigned to another unblinded assessor.
Outcome Measures
Scoring sheets specific to the outcome measures and data entry forms will be used for documentation. Secured folders specifically assigned for documentation will be used to maintain assessment records.
Paediatric Balance Scale
The Paediatric Balance Scale (PBS) is used to assess the functional balance skills of school-aged children. It has a maximum score of 56 points and consists of 14 items, with scores ranging from 0 (least functional) to 4 (most functional). PBS’s validity is supported by its high test–retest and interrater reliability (ICC = 0.998 and 0.997, respectively), as well as its strong correlation with other motor function assessments, including the Paediatric Evaluation of Disability Inventory and the Gross Motor Function Measure. 18
Short Sensory Profile
The Short Sensory Profile (SSP) is a questionnaire used to assess a child’s low energy, tactile sensitivity, taste sensitivity, movement sensation, desire sensation, auditory filtering, and visual sensitivity. The SSP has shown good content validity and high test–retest reliability (r = 0.76–0.90), enabling it to distinguish between children with and without sensory processing issues. 19
Trail Making Test
The test has Part A and Part B. In Part A, the participant must make as many accurate and timely connections between numbered circles (1, 2, 3, etc.) in order, while in Part B, the participant switches between letters and numbers in ascending order, such as 1-A-2-B-3-C, and so on. Inter-rater reliability is very high, often exceeding 0.95, and shows a strong correlation with other executive functioning tests. 20
Developmental Coordination Disorder Questionnaire 2007
It has 15 items that are divided into three categories: General coordination, fine motor and handwriting skills, and control during movement. Concurrent validity exhibits a moderate to strong range of correlation coefficients (r = 0.50–0.70), while studies have demonstrated strong test–retest reliability with correlation values (r) greater than 0.90. 21
Statistical Analysis
The collected data will be analysed by the principal investigator. Descriptive statistics will be employed to present the baseline characteristics of eligible participants. The Kolmogorov–Smirnov test is applied to establish the normality of the collected data for a sample size >50, and for the sample size < 50, the Shapiro–Wilk test will be applied. Descriptive statistics will be expressed as mean ± standard deviation or median and interquartile range. Depending on the normality of data, within-group comparisons and between-groups comparisons will be conducted using the Statistical Package for the Social Sciences (SPSS) version 16 software (SPSS Inc., Chicago, IL, USA). The analysis will follow the intention-to-treat approach.
Data Management
Data will be entered into an electronic database and will be password-protected to help prevent unauthorised data access. Discrepancies, if any, will be cross-verified and corrected via double data entry. Each participant will be allotted a unique identification code to maintain data confidentiality. Regular data monitoring will be conducted to detect missing or erroneous entries. To ensure the confidentiality of the data, access will be restricted to the principal investigator only.
Discussion
ADHD, a complex neurodevelopmental condition, often involves issues with attention regulation, overactivity, and impulsiveness. Currently, research highlights multi-factorial treatments tailored to individual profiles, whereas traditional models primarily emphasised medication. While medications remain an essential component, non-medical options have gained prominence as understanding of this multifaceted disorder continues to grow.
Multimodal training enhances neuroplasticity, aiming to strengthen functional connections across brain regions associated with ADHD. Specifically, irregularities in tactile, auditory, and vestibular modalities can worsen inattentiveness and behavioural regulation issues. 22 Structural and functional imaging research shows that children with ADHD often exhibit altered activity in the areas of the brain involved in sensorimotor integration and executive function. 23 Therefore, incorporating sensory integration into ADHD treatments addresses these sensory modulation challenges and boosts attentional control. By combining cognitive and sensory-motor-based techniques, multimodal training has the potential to offer more comprehensive support for children facing multiple challenges.
Sensorimotor activities that involve coordination and balance stimulate the cerebellum’s connections to the cortex in ways that are underdeveloped in those with ADHD. Studies have shown that balance training and rhythmic movement therapies improve behaviour and focus by promoting cerebellar development, which, in turn, strengthens motor planning and impulse control. 24 For instance, programmes that incorporate rhythmic entrainment, such as Interactive Metronome training, have shown improvements in timing, attention, and academic performance. Rhythmic activities challenge the cerebellum to regulate movements and attention over time better, leading to improved coordination between thoughts and actions. Diverse sensorimotor routines engaging the cerebellum’s role in cognition show promise for reducing ADHD’s impact on executive functions. 25 Cognitive interventions centring around working memory, inhibitory control, and processing speed display reasonable efficacy in mitigating fundamental ADHD signs, specifically when adapted to singular shortcomings. Studies imply programmes such as Cogmed have exhibited improvements in executive performance and lessened unfocused behaviours. 26 However, when paired with sensory and motor facets, such as in neurocognitive coaching routines, the synergistic impact appears more robust. Findings from the investigation have demonstrated that these trainings might strengthen connectivity between prefrontal and parietal regions. 27
While medication remains an important treatment option for many, the incorporation of alternative therapies can provide symptom relief without dependence or undesirable side effects. This multi-pronged nature of integrative interventions aids neuroplastic adaptation through repeated exposure across domains. Sensory stimulation refines cortical maps, motor skills support synaptic pruning and coordination, and cognitive exercises augment dopamine and norepinephrine along prefrontal circuits, key neurotransmitters in ADHD. Baseline evaluations inform individualised programmes targeting sensory sensitivities, motor function, and executive control to optimise neuroplasticity through a personalised approach. Enhanced neuroplasticity may then support compensatory skill development. 28
Conclusion
In conclusion, integrative sensory, motor, and cognitive training represents a promising adjunctive intervention in ADHD management. The multimodal stimulation of neural circuits enhances core functions and facilitates more adaptive behaviours. This approach aligns with current guidelines emphasising non-drug strategies for ADHD, engaging the individual, and applying skills in real-world contexts. Moreover, such techniques tend to gain broader applicability when deployed in educational or community environments, optimising academic performance and quality of life over the long-term.
Footnotes
Abbreviations
ADHD: Attention Deficit Hyperactivity Disorder, DCD: Developmental Coordination Disorder, ADL: Activities of Daily Living, SPIRIT: Standard Protocol Items: Recommendations for Interventional Trials, OPD: Outpatient Department, RCT: Randomised Controlled Trial, PBS: Paediatric Balance Scale, SSP: Short Sensory Profile, TMT: Trail Making Test, DCDQ’07: Developmental Coordination Disorder Questionnaire 2007, SPSS: Statistical Package for the Social Sciences
Authors’ Contribution
Nidhi Sharma: Principal investigator, conceptualisation of study design, drafting the protocol, data collection, sample size estimation, and manuscript preparation.
Aksh Chahal: Senior investigator, supervision, revision of the protocol, conceptualisation, critical review. The authors approved the final version of the protocol.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Data Availability Statement
The data generated during the current study will be available upon request from the corresponding author, subject to ethical approval.
Data Sharing
The results will be communicated via publications in peer-reviewed journals, conference presentations, and updates in the clinical trial registry.
ICMJE Statement
Form attached as Annexure I (Supplementary File).
Informed Consent
Written informed consent is obtained from each participant before undertaking any trial-related activities. (Supplementary File: Attached as Annexure II).
Statement of Ethics
The present study is being conducted in accordance with the principles outlined in the Declaration of Helsinki and has obtained approval from the Ethics Committee of the School of Allied Health Sciences, Galgotias University, Greater Noida, Uttar Pradesh, India (Ref. no. SEC/SAHS/PHD/24/10).