
Abstract
Background
Genetic polymorphisms significantly influence individual responses to antidepressant medications. Among these, variations in the cytochrome P450 enzyme CYP2C19, particularly the *2 allele, are known to affect drug metabolism, with implications for both efficacy and safety. South Indian populations exhibit a relatively high prevalence of this polymorphism, yet data specific to psychiatric cohorts remain limited.
Purpose
This study aimed to determine the prevalence of the CYP2C19*2 polymorphism among South Indian psychiatric patients and to classify the corresponding metaboliser phenotypes to inform precision prescribing strategies for psychotropic medications.
Methods
A cross-sectional observational study was conducted involving 140 psychiatric patients of South Indian ancestry across two tertiary psychiatric centres. Genomic DNA was extracted from peripheral blood samples and genotyped for the CYP2C19*2 (681G>A) variant using TaqMan-based real-time PCR. Participants were categorised into metaboliser phenotypes based on CPIC guidelines: normal (*1/*1), intermediate (*1/*2) and poor (*2/*2) metabolisers. Genotype frequencies were assessed for Hardy–Weinberg equilibrium (HWE) and descriptive statistics were used to summarise allele and phenotype distributions.
Results
The CYP2C19*2 allele frequency was 27.5%. Genotype distribution was as follows: *1/*1 in 55.7%, *1/*2 in 33.6% and *2/*2 in 10.7% of participants. Accordingly, 44.3% of patients were classified as non-normal metabolisers (NMs) (intermediate or poor). The genotype distribution did not deviate significantly from HWE (p = .0614), indicating population stability.
Conclusion
A substantial proportion of South Indian psychiatric patients exhibit reduced CYP2C19 enzyme activity due to the presence of the *2 allele. These findings highlight the clinical utility of pre-emptive pharmacogenetic testing to guide antidepressant selection and dosing in this population, supporting the implementation of precision psychiatry in routine mental health care.
Introduction
Mental health is a significant component of human well-being, yet depression continues to pose a major global health burden, affecting more than 280 million individuals worldwide. Epidemiological data indicate that approximately one in three women and one in five men are likely to experience a major depressive episode at some point in their lives.1, 2 In the Indian context, the prevalence of depression exhibits significant variability, ranging from 1.8% to 39.6%, reflecting regional and methodological differences. Notably, depression is anticipated to become the second leading cause of disease-related disability in India by 2030, underscoring the urgent need for targeted mental health strategies. 3
Although antidepressants, especially selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs), are widely prescribed, therapeutic responses remain suboptimal or inconsistent across patients. Many patients experience poor response, intolerable side effects, or premature treatment discontinuation, all of which hinder recovery.4, 5 These variable responses are influenced by a complex interplay of genetic, physiological and environmental factors, such as age, hepatic and renal function, nutritional status and lifestyle habits. Among them, genetic factors play a key role by affecting both drug pharmacokinetics and pharmacodynamics, thereby influencing treatment efficacy and tolerability. 6 Despite extensive research, there is still limited evidence identifying consistent demographic, clinical, or genetic predictors of individual antidepressant response.4, 5
Polymorphisms in drug-metabolising enzymes (e.g., CYP2C19, CYP2D6, CYP3A4), transporters (e.g., ABCB1) and pharmacodynamic targets (e.g., HTR2A, SLC6A4) have been associated with individual variability in antidepressant response. 7 In India, particularly among South Indians, the CYP2C19 poor metaboliser (PM) genotype is relatively prevalent (~12.6%), suggesting that over 28 million individuals may have reduced capacity to metabolise key antidepressants, potentially leading to altered drug levels and treatment outcomes.8, 9
Clinical pharmacogenetic guidelines from Clinical Pharmacogenetics Implementation Consortium (CPIC) and Dutch Pharmacogenetics Working Group (DPWG) recommend dose adjustments or alternative medications for CYP2C19 PMs taking antidepressants, due to the risk of drug accumulation, increased side effects and higher discontinuation rates.10, 11 However, these recommendations are largely derived from non-South Asian populations, and real-world data correlating genotypes with drug levels remain limited in Indian psychiatric populations. 12
The present study explores the prevalence of CYP2C19 PM genotypes among South Indian psychiatric patients, with the goal of elucidating the influence of genetic variability on drug pharmacokinetics in this population. These findings aim to address the critical gap in population-specific pharmacogenetic data and underscore the importance of incorporating genotype-informed approaches to optimise antidepressant therapy in genetically distinct and clinically underrepresented groups.
Materials and Methods
Study Design and Setting
This cross-sectional observational study was carried out at two psychiatric centres in South India: Department of Psychiatry, JSS Hospital, Mysuru (Karnataka) and Vazhikatti Mental Health Centre and Research Institute, Coimbatore (Tamil Nadu). Ethical clearance was obtained from the Institutional Ethics Committee of JSS Medical College, Mysuru (Ref. No. JSSMC/IEC/13042022/14NCT/2021-22). All study procedures conformed to the ethical standards set forth in the Declaration of Helsinki and adhered to national guidelines governing research involving human participants.
Study Population
A total of 140 psychiatric patients (aged ≥18 years) were recruited from both outpatient and inpatient services and included only those with at least three generations of South Indian ancestry who spoke a South Indian language as their mother tongue. Individuals with known hepatic or renal impairment, pregnant or lactating women were excluded. Written informed consent was obtained from all participants prior to their inclusion in the study. The consent form was approved by the Institutional Ethics Committee and was provided in English, as well as in the participants’ native languages (Tamil/Kannada), to ensure full comprehension and voluntary participation. Clinical and demographic details, including age, sex, anthropometrics, substance use, medical history, diagnosis and treatment regimen, were recorded using a structured data collection form. Biochemical parameters were reviewed to confirm eligibility, and all data were compiled in MS Excel for analysis.
Blood Sample Collection
Following enrolment, 5 mL of venous blood was drawn from each participant into EDTA-containing collection tubes to prevent coagulation. Samples were centrifuged at 4,000 rpm for 5 minutes. The plasma was separated, while the remaining cellular pellet (buffy coat) was retained for DNA extraction.
Genotyping of CYP2C19*2 (rs4244285, 681G>A)
Genomic DNA was extracted from the buffy coat using the conventional phenol–chloroform method. The concentration and purity of the isolated DNA were evaluated using a NanoDrop™ 2000 spectrophotometer (Thermo Fisher Scientific, USA), with an acceptable purity range defined by an A260/A280 ratio between 1.8 and 2.0. To assess the structural integrity of the DNA, all samples were analysed via 2.5% agarose gel electrophoresis. Visualisation under UV light confirmed the presence of high-molecular-weight DNA with minimal degradation, as illustrated in Figure 1.
Gel Electrophoresis Image Showing PCR Amplification Products for the CYP2C19*2 Polymorphism.

Genotyping of the CYP2C19*2 (681G>A) variant was performed by quantitative real-time PCR using a commercial allelic discrimination assay (Eurofins Genomics CYP2C19*2 kit) with TaqMan chemistry. PCR reactions (20 µL total volume) contained 10 µL of 2× Ex Taq premix (RR401, Takara Bio, Shiga, Japan), 0.4 µL of each primer (forward and reverse), 0.8 µL probe mix, 1 µL genomic DNA (~20–50 ng), and nuclease-free water to 20 µL. Primers specific to the rs4244285 locus were designed to flank the target region, with sequences as follows: forward primer 5′-CAACCAGAGCTTGGCATATTG-3′ and reverse primer 5′-CCATCGATTCTTGGTGTTCTTT-3′ (synthesised by Eurofins). Two allele-specific probes were used: a HEX-labelled probe perfectly matching the wild-type (681G) sequence (5′-AATTTTСССАСТАТСАТТGАТТАТТTСССG-3′) and a FAM-labelled probe matching the variant (681A) sequence (5′-AATTTTCCCACTATCATTGATTATTTCCCA-3′). The primer pair amplifies a 123 bp fragment spanning the CYP2C19*2 (681G>A) locus. The primer and probe sequences (Eurofins) were as provided by the manufacturer and have been previously validated for CYP2C19 genotyping.
Genotyping was performed using the Gentier® 48E Real-Time PCR System (Tianlong, Xi’an, China). The thermal cycling protocol began with an initial denaturation at 95°C for 10 minutes, followed by 40 cycles of amplification (two-step) consisting of denaturation at 95°C for 10 seconds and annealing/extension at 60°C for 30 seconds. Following amplification, a melting curve analysis was conducted by incrementally increasing the temperature from 60°C to 95°C to confirm product specificity. Fluorescence signals were captured during each cycle to monitor amplification in real-time and enable genotype differentiation. Genotypes (homozygous wild-type *1/*1, heterozygous *1/*2, or homozygous variant *2/*2) were automatically determined by the system’s software and subsequently verified through manual inspection. To validate genotyping accuracy, 10% of the samples were randomly selected for repeat analysis, with complete concordance observed across replicates. Negative (no-template) controls were included in every run to monitor for potential contamination.
Metaboliser phenotypes were classified in accordance with CPIC guidelines: individuals with the *1/*1 genotype were categorised as normal metabolisers (NMs), those with *1/*2 as intermediate metabolisers (IMs), and those with *2/*2 as PMs. 13
Statistical Analysis
The sample size (n = 140) was determined based on an estimated prevalence of 15% for CYP2C19 PMs, with a 95% confidence level and a 6% margin of error. This yielded a minimum required sample size of 136, and an additional buffer was included to compensate for potential exclusions or data loss. Continuous variables were summarised as means with standard deviations, while categorical variables were reported as counts and percentages. Genotype and allele frequencies were calculated, and the distribution of CYP2C19*2 genotypes was assessed for deviation from Hardy–Weinberg equilibrium (HWE) using the chi-square (χ²) test by comparing observed and expected counts. All statistical analyses were conducted using GraphPad InStat (GraphPad Software, San Diego, CA, USA), with a two-tailed p value of <.05 considered indicative of statistical significance.
Results
A total of 140 individuals receiving psychiatric care were included in the study to evaluate the distribution of the CYP2C19*2 polymorphism. The study population consisted of 72 males (51.4%) and 68 females (48.6%), with participant ages ranging from 18 to 75 years. The mean age was 38.5 ± 12.54 years, indicating a predominantly adult population with broad age variability, reflective of typical clinical psychiatric settings.
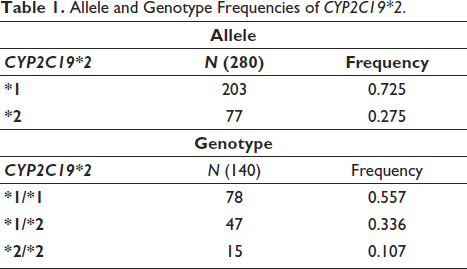
Out of the 280 alleles analysed (140 individuals × 2 alleles), the wild-type *1 allele was found in 203 individuals, yielding an allele frequency of 0.725 (72.5%). Conversely, the *2 variant allele was detected in 77 individuals, corresponding to a frequency of 0.275 (27.5%). These findings indicate a moderate prevalence of the CYP2C19*2 loss-of-function allele within this South Indian psychiatric population, emphasising the potential for altered drug metabolism, particularly for substrates like escitalopram and amitriptyline.
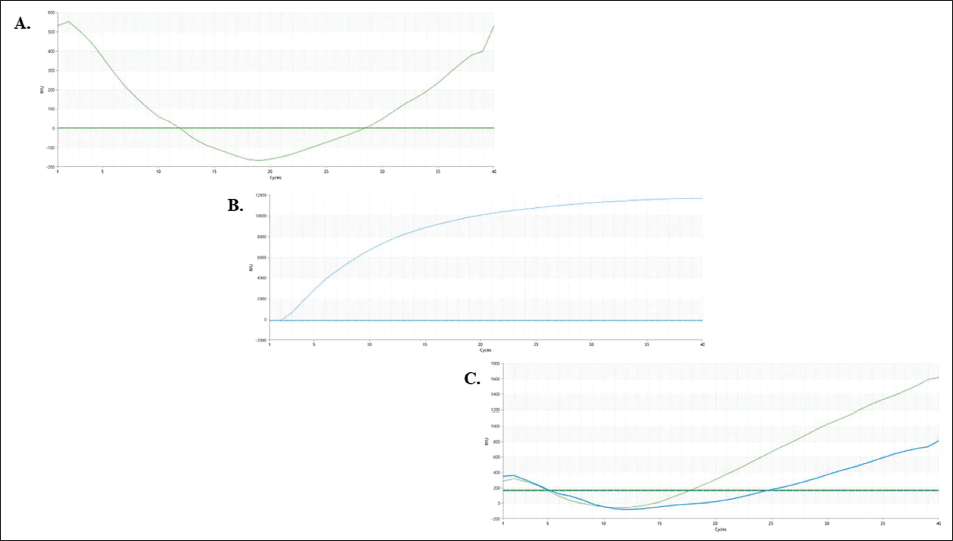
Genotype analysis of the CYP2C19*2 polymorphism among the study participants revealed three distinct genotypes: 78 individuals (55.7%) were homozygous for the wild-type allele (*1/*1), 47 individuals (33.6%) were heterozygous (*1/*2) and 15 individuals (10.7%) were homozygous for the mutant allele (*2/*2). Representative amplification curves for each genotype are shown in Figure 2. The distribution of CYP2C19*2 alleles and genotypes within the study population is presented in Table 1.
Allele and Genotype Frequencies of CYP2C19*2.
Representative Amplification Curves for CYP2C19*2 Genotyping (A) Homozygous Wild-type (*1/*1), (B) Homozygous Variant (*2/*2) and (C) Heterozygous (*1/*2).
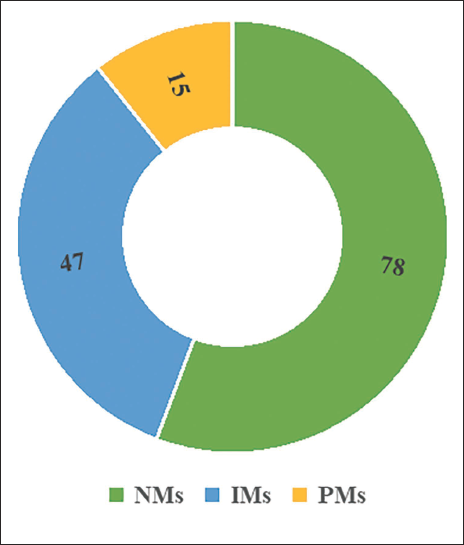
Based on this distribution, participants were further categorised into predicted metaboliser phenotypes. Individuals with the *1/*1 genotype were classified as NMs, representing those with fully functional CYP2C19 enzyme activity. Heterozygous individuals (*1/*2) were categorised as IMs, typically exhibiting reduced enzymatic function due to the presence of one loss-of-function allele. Finally, homozygous carriers of the *2 allele (*2/*2) were designated as PMs, characterised by significantly impaired or absent CYP2C19 enzymatic activity.
This phenotype-based classification revealed that 44.3% of the study population falls under intermediate and PM categories, indicating a substantial proportion of individuals with diminished CYP2C19 function. From a clinical perspective, variations in CYP2C19 metabolic activity are highly significant, as reduced enzyme function can result in elevated plasma concentrations of CYP2C19-substrate medications, thereby increasing the risk of adverse drug reactions or diminished therapeutic efficacy. Figure 3 illustrates the distribution of metaboliser phenotypes, reinforcing the need for personalised treatment strategies based on genotype-guided dosing.
Predicted CYP2C19 Metaboliser Phenotypes.
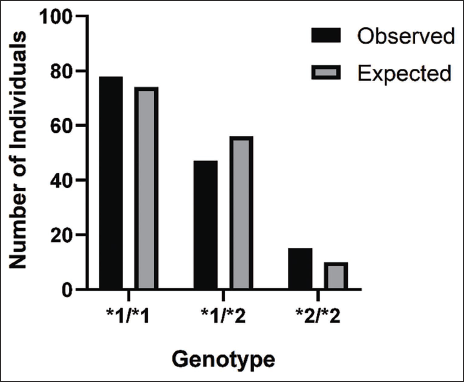
The observed genotype counts were compared with those expected under HWE assumptions to determine population-level stability of allele transmission. Using a chi-square test (χ² = 3.4986, p = .0614), the genotype distribution did not significantly deviate from HWE, indicating no apparent selection bias or genotyping errors. This suggests that the CYP2C19*2 alleles are in genetic equilibrium within the sampled population. The comparison between observed and expected genotype counts is illustrated in Figure 4.
Observed Versus Expected Genotype Distribution.
Discussion
This study provides a focused examination of the CYP2C19*2 polymorphism among South Indian psychiatric patients and its potential implications for antidepressant pharmacotherapy. The findings underscore the substantial presence of CYP2C19*2 variant alleles in this population, with a prevalence of 27.5%, and a corresponding genotype distribution of 55.7% (*1/*1), 33.6% (*1/*2) and 10.7% (*2/*2). These values are consistent with the expected HWE, indicating a genetically stable population with no apparent selective pressures influencing allele transmission. Importantly, the data suggest that nearly one in two individuals in this population carries at least one *2 allele, a loss-of-function variant known to reduce CYP2C19 enzymatic activity and thereby influence drug metabolism, particularly for SSRIs and TCAs. Approximately half of the patients carried one copy of *2 (*1/*2 genotype), and a notable minority were homozygous (*2/*2). This genotype distribution translates into many IMs and a substantial fraction of PMs among patients. These findings align with and extend previous regional data.
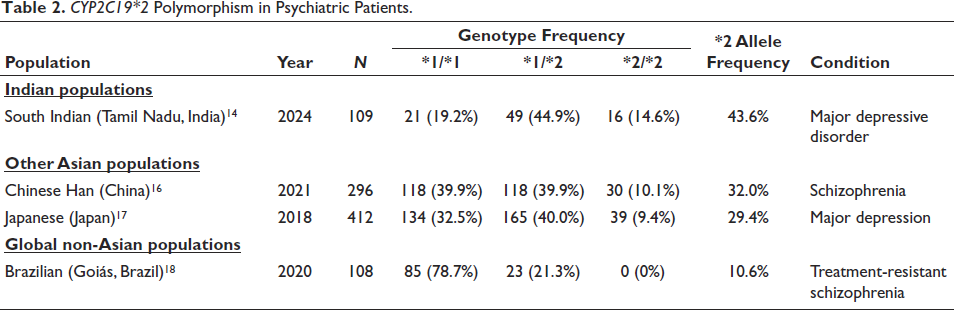
A recent South Indian study of patients with major depressive disorder (MDD) reported *2 variant alleles in ~45% of subjects, with 55% being IMs and 17.4% as PMs. 14 In healthy South Indians, CYP2C19*2 allele frequency has been reported around 35%–40%, resulting in a PM genotype frequency on the order of 12%–13%. 9 Notably, one Tamilian study found a *2 allele frequency as high as ~40% (with *2/*2 genotype ~12%). 15 Thus, our psychiatric population’s genotype proportions mirror or slightly exceed those of healthy South Indians, suggesting no protective genetic effect in psychiatric disorders. Table 2 summarises previously reported CYP2C19*2 genotype distributions in psychiatric populations across various ethnic groups.
CYP2C19*2 Polymorphism in Psychiatric Patients.
When comparing across geographic and ethnic groups, the CYP2C19*2 allele is consistently more common in South Asian populations than in Europeans or Africans. In Europe, *2 allele frequencies range roughly 8%–18%, lowest in countries like the Czech Republic (~8%) and higher (up to ~18%) in parts of Northern/Western Europe. 19 By contrast, South Asians (including Indians and Pakistanis) have markedly elevated *2 prevalence. Meta-analyses report *2 allele frequencies in Indians of 30%–35%. Reflecting this, the prevalence of non-NM phenotypes (IM + PM) is very high in India (~80%). 20 Indeed, one large review found Indian populations had the highest percentage of CYP2C19 PMs worldwide (up to ~31%), whereas Northern Europeans typically exhibit only ~3%–5% PMs (consistent with much lower *2 allele frequency). East Asian populations also have high *2 frequencies (often 25–35%); for example, Japanese studies report ~18%–20% PMs, and Han Chinese often have *2 prevalence around 30% or more. In contrast, European and African ancestries generally exhibit *2 frequencies below 20%, with PM rates of only a few percent. In sum, our South Indian population’s findings, *2 allele in ~30%–40% of alleles and PM genotype in ~10%–20% of individuals, are concordant with the elevated rates seen in other South and East Asian groups and exceed those in non-Asian populations.19, 20
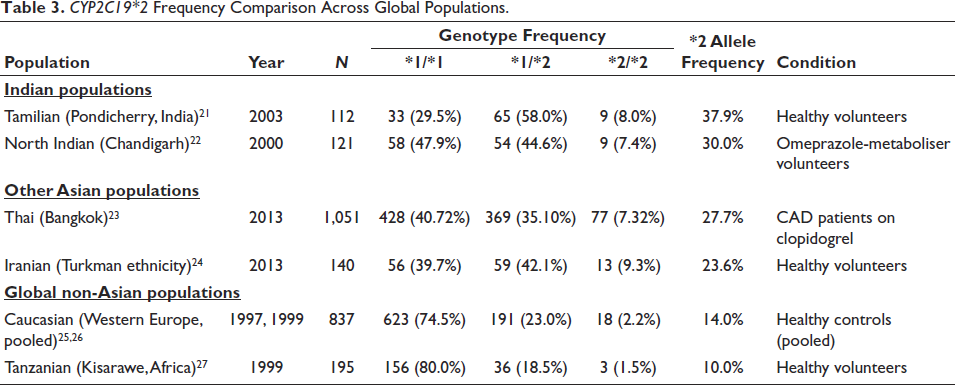
This geographic pattern underscores the need to consider population differences when interpreting CYP2C19 data. Compared to healthy Indian data, our patient population did not show major deviations; however, some psychiatric studies have observed slight differences. To contextualise our findings, Table 3 presents CYP2C19*2 allele frequencies across various global populations, including healthy volunteers and individuals with non-psychiatric conditions.
CYP2C19*2 Frequency Comparison Across Global Populations.
The high prevalence of CYP2C19 IMs and PMs in our South Indian psychiatric population has significant pharmacogenetic implications, particularly in the context of antidepressant therapy. CYP2C19 is a key enzyme in the metabolism of several widely prescribed psychotropic drugs, especially SSRIs such as escitalopram, sertraline and citalopram. Reduced-function alleles like *2 result in slower drug clearance, leading to elevated plasma concentrations. Clinical studies have demonstrated that carriers of these alleles exhibit altered therapeutic response profiles. For instance, escitalopram treated IMs and PMs have been shown to experience higher serum drug levels and diminished symptom improvement compared to NMs. 28 Joković et al. reported significantly lower response rates (~75% decrease) and greater incidence of central nervous system side effects (~43% increase) in poor CYP2C19 metabolisers. 29 Additionally, the FDA has issued warnings regarding the risk of QT interval prolongation with citalopram in PMs, underscoring the need for genotype-informed dose adjustments. Given that over 44% of our study participants fall within the IM and PM categories, a substantial portion of psychiatric patients may be at heightened risk for SSRI-related adverse events or suboptimal therapeutic outcomes unless dosing is individualised.
Beyond SSRIs, CYP2C19 also plays a crucial role in the metabolism of TCAs such as amitriptyline, which is converted to its active metabolite nortriptyline via this pathway. PMs show reduced conversion and clearance, resulting in higher exposure to amitriptyline and associated risks such as anticholinergic burden or cardiotoxicity. The CPIC guidelines recommend dose reductions for PMs initiating TCA therapy, and even IMs may require careful titration based on serum levels and clinical response. 30 The pharmacokinetic impact of CYP2C19 extends to other psychotropic agents as well. For example, sertraline plasma levels have been observed to increase in *2 allele carriers, raising tolerability concerns. Benzodiazepines like diazepam, commonly co-prescribed for anxiety or sleep disturbances, also rely on CYP2C19 for metabolism. PMs demonstrate slower diazepam clearance, resulting in prolonged sedation and risk of accumulation. 31 Clobazam, while primarily used for epilepsy, is sometimes employed in psychiatric practice; its active metabolite, norclobazam, is inactivated by CYP2C19 PMs. 32 PMs are at risk for excessive accumulation, prompting dose adjustment recommendations in prescribing guidelines. Collectively, the elevated frequency of CYP2C19*2 alleles in our population highlights the urgent need for genotype-guided prescribing strategies to optimise efficacy and minimise toxicity in psychiatric pharmacotherapy.
The pharmacokinetic variations associated with CYP2C19 polymorphisms translate into meaningful clinical outcomes, underscoring the necessity of genotype-guided treatment in psychiatric care. Ignoring such variability contributes to therapeutic inefficacy and increased trial-and-error prescribing. Emerging clinical evidence supports genotype-guided dosing: for example, a Translational Psychiatry trial showed improved tolerability when escitalopram dosages were adjusted according to CYP2C19 status, 28 while large randomised trials, including those published in JAMA, report significantly higher remission rates with pharmacogenomic-guided antidepressant selection compared to standard care. 33 These findings affirm that incorporating CYP2C19 genotyping into routine psychiatric prescribing enhances both safety and therapeutic outcomes.
Conclusion
CYP2C19 genotyping holds substantial clinical value in psychiatric practice, particularly in South Indian populations where the prevalence of the *2 allele, and thus poor or intermediate metaboliser status, is markedly high. This genetic profile predisposes a significant subset of patients to altered drug metabolism, increasing the risk of adverse effects, therapeutic failure and QT prolongation when treated with standard doses of psychotropics such as SSRIs, TCAs and benzodiazepines. Incorporating genotype-guided strategies, endorsed by CPIC and regulatory bodies, enables proactive dose adjustments or alternative drug selection, minimising harm and enhancing treatment outcomes. In our population, recognising CYP2C19 PMs (~12%) could avert numerous avoidable toxicities and inefficacies that might otherwise appear unpredictable. These results not only align with broader Asian pharmacogenetic patterns but also reinforce the imperative for precision psychiatry. By tailoring treatment to genetic makeup, clinicians can move beyond trial-and-error prescribing toward safer, more effective, and individualised care.
Footnotes
Acknowledgement
The authors gratefully acknowledge the support of JSS Hospital, Mysuru, and Vazhikatti Mental Health Centre and Research Institute, Coimbatore, for their valuable assistance in facilitating patient recruitment and sample collection. We also extend our sincere thanks to the Department of Pharmacy Practice and the Library, JSS College of Pharmacy, Ooty, for their consistent academic and logistical support throughout the research process.
Authors’ Contribution
Bhavatharini Sukumaran conceptualised and designed the study, performed the laboratory experiments, collected the clinical samples, and drafted the manuscript. Aswathy VS and Rinu Mary Xavier contributed to manuscript writing, literature review, and critical editing. Kishor M and Selvaraj Krishnamurthi assisted in patient recruitment and sample collection and provided essential clinical insights. Arun KP and Deepalakshmi M provided overall supervision, contributed to study design refinement, and critically reviewed the final manuscript for intellectual content. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Indian Council of Medical Research (ICMR), New Delhi. The first author is a recipient of the Senior Research Fellowship [F. No. 45/07/2022/HUM/BMS, dated 9 June 2022] awarded by ICMR. No additional financial support or sponsorship was received for this work.
Patient Consent
Written informed consent was obtained from all participants prior to their inclusion in the study. The consent form was approved by the Institutional Ethics Committee and was provided in English, as well as in the participants’ native languages (Tamil/Kannada), to ensure full comprehension and voluntary participation.
Statement of Ethics
Ethical approval for this study was obtained from the Institutional Ethics Committee of JSS Medical College, Mysuru (Ref. No. JSSMC/IEC/13042022/14NCT/2021-22). All procedures involving human participants were conducted in accordance with the ethical standards outlined in the Declaration of Helsinki and adhered to the national guidelines for research involving human subjects.