
Abstract
Background
Osteoarthritis (OA) is a degenerative joint disease increasingly linked to neuroinflammation, and a heightened response of nociceptive neurons called central sensitisation, leading to persistent pain and functional decline. Neuroinflammation, along with dysfunction in serotonergic and noradrenergic pathways, and chronic activation of the hypothalamus pituitary adrenal (HPA) axis, prolongs the pain sensations. Conventional treatments, including Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and opioids, primarily offer symptomatic relief but fail to address these central mechanisms while posing risks of adverse effects.
Purpose
This narrative review explores alternative approaches, specifically Ayurveda and yoga-based interventions, as potential strategies to mitigate neuroinflammation and pain hypersensitivity in OA.
Method
A comprehensive literature search was conducted across databases of PubMed, ScienceDirect, Scopus and Google Scholar from the year 2005 to 2025 using multiple keywords related to OA, central sensitisation, yoga, and Ayurveda. Published studies were reviewed for outcomes related to central sensitisation and OA.
Results
Ayurvedic herbs consistently have been shown to have positive results in modulating inflammatory mediators and oxidative stress without adverse effects. Yoga has been shown to regulate the HPA axis, enhance vagal tone, and promote neuroplasticity, all of which contribute to pain modulation. Furthermore, mindfulness and meditation practices stimulate the release of endogenous opioids, thereby reinforcing descending pain inhibitory pathways. Both interventions contribute to OA management by supporting weight control, improving metabolic function, enhancing executive-level modulation of pain perception, and promoting better sleep quality. Their active analgesic effects, combined with a holistic mind-body approach, offer a safe and sustainable strategy for long-term OA management.
Conclusion
Yoga and Ayurveda have shown reliable results in providing safe and effective management of chronic OA accompanied by central sensitisation. However, there is a need for large-scale studies to integrate these into the mainstream treatment regimens.
Introduction
Osteoarthritis (OA) is a degenerative joint disease with cardinal features of pain, stiffness and loss of normal joint movement. It affects 595 millions of people worldwide. 1 Its prevalence is increasing with the global rise in elderly population, placing a disproportionate burden on older adults, women, certain racial and ethnic groups, and individuals with lower socioeconomic status. 2 Anatomical and physiological changes such as cartilage deterioration, bone remodelling, osteophytes formation, joint inflammation, and loss of normal joint function are common features of OA. The condition often begins with micro- and macro-injury to the joint, which initiates maladaptive repair processes that produce aberrant tissue metabolism. 3 World Health Organisation has also addressed the rising burden of OA through its rehabilitation initiative 2030, and declared current decade as the decade of healthy ageing. 4 These programs aim to support rehabilitation of approximately 344 million people affected. The hallmark symptom of OA is joint pain, which can turn into chronic pain due to involvement of neuroinflammation and central sensitisation pathways. 5 Intercommunication between the nervous systems and immune system can transpire at multiple levels: within the affected synovium, where nociceptors and macrophages interact, in the dorsal root ganglion, which may become infiltrated by macrophages due to peripheral inflammation, and in the spinal cord dorsal horn, where microglia can modulate synapses between nociceptors and second-order neurons. 6 Evidence suggests that initially OA pain is mediated by peripheral pathways; however, in chronic stages, central nervous system hypersensitivity can play a major role. 7 OA is primarily a biomechanical disease with a component of chronic low-grade inflammation mediated by ageing, obesity and metabolic syndromes contributing to its progression. The key inflammatory mediators involved with OA include cytokines, chemokines, growth factors, adipokines and neuropeptides. 8
The modern medical treatment transiently relieves symptoms, but in the long run, can cause havoc to health. 9 Oral and topical use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) can temporarily alleviate pain and improve function in hand, knee and hip OA. 10 With oral preparations, the lowest effective dose and shortest duration of treatment are recommended due to the wide range of potential side effects. 10 Consequently, there is a lack of safe and effective long-term treatment options available for OA. This underscores the need for more effective and sustained therapies that target not only pain but also central sensitisation in OA management.
The ancient Indian medical knowledge systems of Ayurveda—the science of longevity, and Yoga—a holistic lifestyle with the aim of self-actualisation, have been explored as a therapeutic approach in the OA population.11, 12 Ayurveda offers detoxification therapies and herbo-mineral pharmacological formulations for managing OA. It provides personalised medicine according to the constitution (Prakriti) of the individual, which aligns well with modern precision medicine. 13 In parallel, Yoga with postures (asanas), breathing practices (Prananyam) and meditation (Dhyan) provide a safe and effective approach to address the mind-body connection. Together, these traditional practices not only improve the joint function and relieve pain but also enhance the overall quality of life in individuals with OA.14, 15
This review explores how two indigenous therapeutic approaches from the Indian Knowledge System (IKS): Yoga and Ayurveda, cater to the burden of OA by targeting on their potential to modulate associated neuroinflammation and central sensitisation. Furthermore, it examines how a biopsychosocial framework that integrates Ayurveda and yoga-based interventions can offer a comprehensive, safe and effective strategy to modulate neuroinflammation, central sensitisation, and pain processing in OA. A comprehensive literature review was conducted, covering studies published between 2005 and 2025. This narrative review appraises a range of outcomes associated with yoga and Ayurveda interventions, including physiological, psychological, biochemical, cellular, and molecular changes relevant to OA pathophysiology, and presents novel study findings while emphasising the necessity for further high-quality research. It also delineates key actions required to advance clinical translation and integration of these approaches.
OA, Neuroinflammation, and Pain: An Evolving Perspective
Osteoarthritis
OA is not just a wear-and-tear condition but a multifactorial disease involving localised inflammation, biomechanical stress, and neuroinflammatory processes, including central sensitisation. Various guidelines recommend educating patients about the underlying disease pathology. 16 The pathology involves chronic inflammation driven by innate and central immunisation mechanisms. 3 Multiple processes such as osteophyte formation, neuroinflammation and central sensitisation contribute to progression of chronic pain in OA. 5
In many cases, radiological features of OA do not correlate well with the patient’s clinical presentation. Therefore, OA diagnosis is based upon a combination of radiological, clinical and pathological findings. Emerging evidence defines OA as a multifaceted joint pathology induced by inflammatory and metabolic factors, leading to joint degeneration.5, 17, 18 Improved understanding of the underlying pathophysiological mechanisms and factors that influence them is critical for developing more effective treatments for OA. Current pharmacological treatments for pain relief include topical and oral NSAIDs such as diclofenac, ibuprofen, opioids, and intraarticular corticosteroid injections. Both NSAIDs and opioids pose a threat of increased cardiovascular mortality. 19 Currently, there are no disease-modifying medications available in the modern medical system that can stop or reverse the progression of OA. 20 While knee replacement procedures are performed to enhance function, concerns remain regarding their long-term viability and the possibility of the need for repetitive surgeries. Whereas complementary and alternative approaches of yoga and Ayurveda have shown long-lasting positive outcomes through some research evidence. An online unsupervised yoga intervention was found to achieve the minimal clinically important difference (MCID) in a randomised controlled trial (RCT) involving 212 adults with symptomatic knee OA. 21 Participants were provided with video recordings of weekly yoga sessions and were instructed to perform them thrice per week. Notably, improvement in physical function was observed. In particular, chair yoga was more suitable, convenient and acceptable for elderly individuals with OA. 22 Similarly, Ayurveda has also shown promising results in the management of OA. In an RCT conducted in the German population with OA, a 12-week intervention involving 15 sessions of Ayurvedic multimodal treatment was compared to conventional multimodal treatment. Ayurveda group demonstrated significantly greater improvement in function, sleep, and quality of life, along with significant reduction in pain & stiffness, with sustained benefits lasting from 6 months to 1 year. 15
Neuroinflammation
Afferent nerve fibres that transmit pain information are responsible for peripheral sensitisation, which is associated with inflammatory mediators. These fibres release neurotransmitters in the spinal cord’s dorsal root ganglion and dorsal horn, which can activate microglia. Activated microglia release pro-inflammatory cytokines, chemokines, and neuropeptides that interact with second-order neurons as well as segmental and descending inhibitory neurons, causing neuroinflammation. Furthermore, it amplifies the hypersensitivity of second-order neurons, causing central sensitisation. 23 Chronic pain and mood abnormalities have been linked to the onset of neuroinflammation in the peripheral nervous system, spinal cord, and supraspinal brain regions. 24 OA has been shown to intensify and hasten the progression of neuroinflammation, contributing to both symptom severity and disease progression.25, 26
Yoga tends to reduce the inflammation, potentially by its positive effect on metabolism and cellular health. With advancing age, there is derangement in the immune system leading to higher levels of vascular inflammation markers such as fibrinogen, hs-CRP, and ESR. A 10-week Hatha yoga intervention in elderly women was found to significantly reduce these inflammatory markers. 27 Additionally, elevated biological stress mediated through the hypothalamus pituitary adrenal (HPA) axis, immune system response and autonomic nervous system is correlated. 28 Yoga is known to reduce stress, which partly explains its positive effect in lowering inflammation and improving vagal tone. 29 In addition to that, yoga intervention helps in reducing circulatory cortisol, IL-6, IL-1ß, CRP, TNF-α, INF-γ, CD56 and IgA. 28 A non-randomised yoga-based lifestyle intervention study reported a reduction in stress and inflammation markers within 10 days in patients with chronic diseases. A significant reduction in plasma cortisol, β-endorphin, IL-6 and TNF-α was reported. 30 An RCT in patients with rheumatoid arthritis showed a reduction in proinflammatory cytokines (IL-6, IL-17A, and TNF-α) and an increase in anti-inflammatory cytokine (TGF-β) with an 8-week yoga-based lifestyle intervention. 31 In a placebo-controlled RCT on COVID-19 positive patients, 7 days of Ayurvedic treatment resulted in significantly lower serum levels of hs-CRP, IL-6 and TNF-α. 32 The Ayurveda group achieved 100% recovery within a week compared to 60% recovery in the placebo group.
Pain
Chronic pain is the most common symptom experienced by patients with OA, yet it is often inadequately managed. Nerve Growth Factors (NGF), inflammatory cytokines, chemokines, and Damage-Associated Molecular Patterns (DAMPs) activate nociceptors, leading to pro-analgesic effects. In OA-affected joints, neuronal sprouting occurs in the synovium and subchondral bone, leading to neuroimmune interactions which further exacerbate discomfort. Additionally, neuroinflammation in the dorsal root ganglia (DRG) and dorsal horn can activate pain-signalling pathways, leading to chronic pain. Factors such as obesity and female gender are known to influence cytokine levels, thereby sustaining inflammation and increasing pain sensitivity in patients with OA. 33 The US Food and Drug Administration (FDA) has also approved Glucagon-Like Peptide (GLP-1) receptor agonists such as Semaglutide and Liraglutide for the treatment of obesity, a major risk factor for OA. 34 However, these pharmacological agents may induce side effects, including nausea, diarrhoea, constipation and vomiting. 35 Given the limitations and side effects of modern pharmacological intervention, there is a growing interest in non-pharmacological strategies to manage chronic pain in OA. Yoga, including mindfulness meditation, has emerged as a promising tool in safely managing chronic pain through various mechanisms. One of those is the physiological activation of the anterior cingulate cortex and the orbitofrontal cortex, along with reduced activity in the thalamus, indicating a shift towards executive-level modulation of pain perception. 36 An RCT conducted on patients with nonspecific low backache investigated the efficacy of the Integral Approach of Yoga Therapy (IAYT), which showed notable improvements in psychological wellbeing and overall quality of life, significant reduction in pain intensity, Tumour Necrosis Factor-alpha (TNF-α) levels, and disability scores. 37 These findings highlight the psychological and molecular mechanisms through which chronic pain can be effectively managed. Another RCT conducted in patients with knee OA demonstrated anti-inflammatory and analgesic effects of ginger powder, a common ingredient of pain management treatment in Ayurveda. The serum levels of TNF-α and Interleukin-1 beta (IL-1β) were reduced after 3 months by taking 500 mg of ginger powder, in comparison to the placebo. 38
Central Sensitisation in OA: The Neurobiological Basis of Chronic Pain
Sensitisation is an enhanced perception of the stimulus. In nociceptors (pain receptors), it can be peripheral, characterised by allodynia (a non-painful stimulus creating a pain sensation) and hyperalgesia (a lower stimulus evoking a higher potential for pain sensation) at the nerve fibre. 39 It becomes central sensitisation when the changes occur in spinal processing of primary afferent inputs, which leads to continuous or prolonged hyperalgesia and allodynia. 40 Central sensitisation is characterised by increased excitability of spinal dorsal horn neurons, impaired descending pain inhibition, and spontaneous pain generation. 41 It is driven by a cascade of neuroinflammatory mediators, including IL-1β, TNF-α, and prostaglandins, which amplify nociceptive transmission and alter synaptic plasticity.33, 42, 43 The involvement of microglia and astrocytes in pain processing has been widely documented, indicating that sustained glial activation exacerbates neuronal hyperexcitability and prolongs pain states. 33 Functional neuroimaging studies have demonstrated structural and functional changes in the brains of OA patients, particularly in regions of the corticolimbic system associated with pain modulation, emotional processing, and cognitive function. The constant activation of the corticolimbic system leads to structural changes in the cortex, which is linked to the conversion of acute pain to chronic pain. 44 This suggests that chronic pain in OA extends beyond peripheral joint pathology, reinforcing the necessity of addressing central pain mechanisms. Steen Pettersen et al. investigated the effects of central sensitisation on hand OA and identified a link between erosive hand OA and central sensitisation. 45 A reverse phenomenon, where improvement in OA symptoms impacts central sensitisation, has also been observed. A study revealed that 6 weeks of balance exercise significantly improved OA symptoms of pain, dynamic balance, function and reduced central sensitisation. 46
Glutamate and GABA play a crucial role in central sensitisation in OA. 47 Glutamate is an excitatory neurotransmitter associated with pain hypersensitivity. GABA, the inhibitory neurotransmitter, regulates pain by inhibiting excitatory signals. Dysregulation in these neurotransmitters, with increased Glutamate and decreased GABA, may contribute to chronic pain in OA. 47 Glutamate, an excitatory amino acid which is present as a neurotransmitter in the CNS, is also found in skin, pancreas and bone. Studies have reported that the involvement of glutamate in bone remodelling and peripheral pain transduction contributes to OA. 48 Glutamate antagonists are seen as possible treatment options for joint pathologies like OA. Glutamate receptors play a major role in chronic-persistent pain of neuropathies, and inflammatory joint pains associated with rheumatoid and OA. 49 Bonnet et al. report high glutamate concentration in the synovial fluid of OA patients. 50 Glutamate receptors regulate IL-6 release, which is an important mediator in arthritic joint degradation. 51 Intra-articular injections of AMPA/kainate glutamate receptor antagonists have shown positive results in the prevention of posttraumatic OA. 50
Emerging evidence suggests that reduced gamma-aminobutyric acid (GABA) levels may significantly influence the pathophysiology of OA pain. Reckziegel et al. demonstrated an inverse correlation between GABA concentrations in the mid-anterior cingulate cortex and the intensity of pain in chronic knee OA patients, indicating that reduced GABA levels may contribute to heightened experience of chronic pain. 47 Similarly, a systematic review highlighted the efficacy of GABA derivatives, such as pregabalin and gabapentin, in alleviating OA pain, further underscoring the role of GABAergic mechanisms in pain modulation. 52 These findings collectively suggest that reduced GABA levels may exacerbate OA pain by impairing inhibitory control within central nociceptive pathways, leading to increased neuronal excitability and pain sensitisation. An RCT compared yoga with an active control arm has shown an increase in GABA levels immediately and even after 3 months of intervention. There was better improvement in mood and anxiety, which was correlated with improved GABA levels. 53 Oral intake of GABA is known to improve sleep and reduce stress. 54 Withania somnifera (Ashwagandha) is a common ayurvedic pain, stress and sleep management medicine. Withanolides and triethylene glycol were the two active compounds found in ashwagandha root and leaves. 55 One RCT reported reduced cortisol and stress in subjects with psychological stress, with an intervention of oral Ashwagandha extract with 300 mg twice a day for 2 months. Possibly by positive impact on the HPA axis, implicated in the regulation of glutamate, GABA and cortisol hormone; yoga and Ayurveda tend to improve the central sensitisation.
Impaired Descending Pathways
Impaired descending inhibitory pathways significantly contribute to central sensitisation, particularly in OA, affecting pain perception and responses. These pathways operate in the dorsal horn of the spinal cord and influence pain response through complex interactions with various neurotransmitters. 56 Glutamate’s impact on N-methyl-D-aspartate (NMDA) receptors is a significant modulator of central sensitisation, resulting in increased intracellular levels of calcium and subsequent kinase activation, amplifying pain signals. In a healthy system, descending pathways including serotonin-norepinephrine and opioidergic processes help to diminish pain sensitivity and to sustain the analgesia. However, in chronic pain syndromes like OA, there is typically a significant loss of descending analgesia, which can result in heightened pain experiences that include hyperalgesia and allodynia and sympathetically maintained pain. 57 Notably, central sensitisation not only alters pain processing but also signifies a shift in central pain mechanisms, making it essential to understand these impairments for therapeutic applications.
Conditioned pain modulation (CPM) is a centrally controlled measure of the overall impact of the descending pain pathway. This includes both the facilitative and inhibitive effects. 58 CPM has been described under several terms, including diffuse noxious inhibitory control (DNIC), heterotopic noxious conditioning stimulation (HNCS), and endogenous analgesia (EA). The restoration of CPM has been documented in patients following joint replacement surgery, indicating that improved descending inhibition can relieve widespread mechanical hyperalgesia. 59 Given the intricacies of central pain processing, tailored treatments that boost descending analgesic pathways may give more effective pain relief for people with OA than standard pain drugs that focus primarily on the peripheral mechanism. There are effective complementary medicines like dietary supplements of curcumin, vitamins, lipolic acid, omega-3, capsaicin, along with yoga intervention, and ayurveda practices that target all three orders of neurons; thus, suggesting a multimodal, customised treatment for each patient. 60 Patient’s responses to therapies vary greatly from one another. Hence, a combination of Ayurveda and yoga can serve the patient well.
Treatments from Ayurveda for Neuroinflammation and Pain Modulation
Ayurveda, the ancient Indian system of medicine, advocates the use of various herbo-mineral formulations for pain relief. Several commonly used components in these formulations have individually demonstrated efficacy in managing pain and inflammation.
Withania somnifera (Ashwagandha): In Ayurveda, it is a known anxiolytic, anti-inflammatory and muscle strength-enhancing herbal medicine. Studies have shown its effect on managing pain, neurodegenerative conditions, 61 and arthritis. 62 A retrospective database search of the trial registry in India suggests a dose of 500–1000 mg of ashwagandha taken for 8–12 weeks in arthritic patients. It has anxiolytic, pro-cognitive, anticarcinogenic, anti-inflammatory, anti-arthritic, and GABA mimetic effects, which promote the formation of dendrites. 63 Preclinical studies have also shown positive results in various disease models. 64 Withanone, a compound found in ashwagandha extract, when given to Wistar rats for 21 days, showed improvement in cognitive function and reduced proinflammatory cytokines. 65
Commiphora wightti (Guggul): It is used to treat diverse chronic diseases, including Alzheimer’s disease, pancreatitis, cancer, arthritis, inflammatory bowel disease (IBD), infectious diseases, diabetes, psoriasis, dermatitis, intestinal metaplasia, otitis media, respiratory diseases, asthma, and gingivitis. It employs hepatoprotective, neuroprotective, anti-inflammatory, antioxidant, cardioprotective, hypolipidemic, and thyroid-stimulatory effects by targeting multiple signalling pathways. 66 This ayurvedic medicine is used for the treatment of several ailments, including bone fractures, arthritis, gout, inflammation, rheumatism, obesity, and lipid abnormalities. 67
Curcuma longa (Turmeric): It is a recognised remedy for numerous respiratory ailments, including asthma, bronchial hyperactivity, and allergies, liver problems, anorexia, rheumatism, diabetic wounds, sinusitis, skin diseases, bowel disorders and arthritis. 68 A meta-analysis suggests 1000 mg/day of turmeric use is recommended for arthritis management, and it blocks NF-κB signals. 69 A randomised controlled trial compared the combination of turmeric, black pepper and ginger to naproxen in 60 OA patients for a period of 4 weeks. The herbal intervention was given twice a day, as compared to naproxen, which was given daily. Prostaglandin E2 (PE2) was evaluated in the two groups. There was a significant reduction in PE2 levels in both of groups, which shows comparable efficacy of the herbal combination to naproxen. 70
Zingiber officinale (Ginger): It has an anti-inflammatory, analgesic and antitumour effect. The analgesic effect is due to the impact on the spinal cord and dorsal root ganglion. There is involvement of substance P, serotonergic receptors, transient receptor potential vanilloid (TRPV), N-methyl-D-aspartate (NMDA) receptors, voltage-gated sodium (NaV) channels and phosphorylated extracellular signal-regulated kinase. 71 A study on cell lines for osteoarthritic and non-osteoarthritic chondrocytes compared the effect of ginger extract on the production of inflammatory mediators. Ginger extract was added at various concentrations between 0 and 2000 µg/mL, and cells were cultured for 24 hours in the presence of cytokine inducers, which were (IL)-1 at 2 ng/mL, tumour necrosis factor (TNF) at 1 ng/mL, and lipopolysaccharides (LPS) at 10 g/mL. In both cell lines, Nitric oxide and prostaglandin E2 reduced with the addition of ginger extract in a linear manner, showing the inhibitory impact of the ginger extract. 72
Syzygium aromaticum (Cloves): It has antifungal, antibacterial, antinociceptive, antibacterial, and anticancer properties. Clove contains anti-inflammatory compounds, such as flavonoids and eugenol, which help reduce pain and inflammation. Clove oil has gained popularity as a natural remedy for toothaches and gum pain due to its anti-inflammatory and analgesic properties. 73 The medicinal properties of clove oil are attributed to the transient receptor potential cation channel subfamily V member 1 (TRPV-1), sometimes referred to as vanilloid receptors 1, which is known to desensitise nerve endings. 74
Yoga Treatment for Neuroinflammation and Pain Modulation
Yoga, a holistic discipline rooted in the IKS, encompasses physical, mental and ethical principles aimed at achieving physical, mental, and spiritual wellbeing. In therapeutic contexts, yoga is increasingly recognised as a mind-body intervention. 75
Yoga Therapy: Yoga is a highly adaptable therapeutic modality that can be tailored to varying intensities based on individual patient needs. Most of its physical components involve low-impact, light-intensity movements, making it especially suitable for older adults and individuals with limited mobility. Recognised as the most popular complementary therapy by the National Centre for Complementary and Integrative Health (USA). 75 This adaptive system provides preventive and curative health benefits while also being safe and effective, which demonstrates distinctive advantages as a pain management approach. Approaching yoga as a therapy implies that mind-body research should focus on long-term systemic changes rather than short-term isolated impacts. 76 Systematic analysis on studies with yoga as intervention for patients with knee OA has proven to reduce stiffness, pain and improve function. 77
Integrated Approach of Yoga Therapy (IAYT): It is a combination of cleansing practices, yoga postures, breathing practices, relaxation-yoga, devotional sessions, stress management and yogic counselling. The intervention, when given for a short duration of 6 days to patients with OA, has been found to be effective in comparison to a control with no treatment. A total of 66 patients with pre-diagnosed knee OA were enrolled to assess for functional improvement of the knee, fear of falls, and range of motion were assessed with significant improvement in all parameters in comparison to the control group in a Randomised Controlled Trial (RCT). 14 In another RCT on patients with chronic low back ache, IAYT showed improvement in clinical, molecular and psychological parameters, and overall quality of life of the individual. 37
Rhythmic Breathing for Vagal Tone: An RCT involving 520 healthy adolescents demonstrated that a six-month yoga intervention of Bhramari Pranayama resulted in a positive shift towards parasympathetic domain, while the controlled group showed a drift towards sympathetic domain, measured by Heart Rate Variability (HRV) and Electro Cardio Gram (ECG). 78 The study findings highlight the beneficial effect of simple Pranayama (breathing) practices on sympathovagal tone. Vagal regulation encompasses eight hierarchical levels, ranging from the brainstem nuclei, hypothalamus, amygdala, and cortical networks to the cardiac ganglia and reflex arcs. 79 By enhancing parasympathetic tone, yoga practices may exert influence across these levels, contributing to improved self-regulation in the behavioural, neuronal, emotional, and cognitive domains. 80 These parasympathetic-driven autonomic inhibitory processes, reflected in vagal nerve-mediated HRV, play a crucial role in dictating attention, emotional stability and mood. 80 Additionally, yoga has been shown to elevate oxytocin levels, a neuropeptide associated with prosocial behaviour and emotional bonding. 81 Through these mechanisms, yoga fosters a range of physiological, psychological and social health benefits through its capacity to facilitate eudaimonic wellbeing as conceptualised in the polyvagal theory. 82
Yoga Modules for Pain: One comprehensive yoga module comprised warm-up exercises, body scan practices, upper body stretches, and a sequence of postures including Cat and Cow Pose, Table Pose, Tree Pose, King Pose, Sun Salutations, Warrior Pose, Triangle Pose, Extended Leg Pose and Spinal Twists. The module also integrated breathing techniques, relaxation practices, chanting, and meditation. 83 A recent RCT involving this module as an intervention was conducted on 117 patients with knee OA, over a 12-week period. The study found the yoga intervention to be non-inferior to strength training, with modest yet meaningful improvement in pain and other symptoms. 84 Additionally, a mindfulness-based program among older adults (>65 years) with chronic low back ache exhibited statistically and clinically significant 30% reduction in current and peak pain intensity (in the past week), in comparison to control, whereas most therapies do not achieve this level of pain reduction. 85 Multiple mindfulness-based interventions ranging from 5 minutes to an hour have also shown efficacy in both acute and chronic pain contexts, leading to reduced dependency on opioids and improved pain-related outcomes.86, 87 Meta-analytical evidence supports the safety and effectiveness of yoga and mindfulness-based interventions in pain management across diverse populations. 88 Yoga has demonstrated efficacy in managing arthritic pain and its associated symptoms. 89 Beyond physical benefits, yoga fosters psychological resilience by enhancing acceptance, self-regulation and overall well-being. Pain, being a subjective experience, is influenced by cognitive and emotional factors. Mindfulness-based elements inherent in yoga promote acceptance of pain, serving as a critical coping mechanism. 87 Further, a systematic review and network meta-analysis involving systematic reviews of Yoga turned out to be more effective in managing acute and chronic spinal pain. 86 A systematic review and network meta-analysis including 1442 participants implicated yoga along with hot fomentation as the most effective treatment for managing chronic nonspecific neck pain, showing reductions in pain intensity, disability, and improved quality of life. 90
Yoga for OA: A targeted yoga module for knee OA includes breathing and loosening practices, postures such as Seated Forward Fold, Earth Salutation, Cobra Pose, Locust Pose and Inverted Pose, and Bridge poses, along with relaxation techniques (instant, quick, and deep). It also incorporates cleansing practices (nasal wash, internal cleansing, candle-gazing, Kapalabhati), pranayamas (sectional, alternate nostril, humming bee, bellows, and cooling breath), and meditation (Om chanting, Cyclic Meditation, Mind Sound Resonance Technique). This integrated module showed significant improvement in OA symptoms within six days of intervention. 14 Yoga has been shown to be effective in managing OA through the physical component of postures and breathing practices, as well as meditation alone. 91 The physical component improves flexibility, muscle strength and joint range while breath regulation stimulates the parasympathetic system, contributing to interrupt the stress-pain cycle associated with chronic pain. This holistic effect contributes to a reduction in pain and stiffness, along with enhancements in psychological health and well-being of the patient. 91 In an RCT involving patients with arthritis, an 8 weeks of Yoga intervention showed lasting positive impact on functional capacity, symptomatic relief, psychological status and quality of life. Importantly, safety analysis was also taken up, implicating no adverse effect associated with the intervention. 83 Another RCT comparing yoga with strength training in 118 patients with knee OA over 24 weeks found that yoga yielded superior results in pain reduction, functional mobility, stiffness, patient global assessment, quality of life and depression scores. 92
Improvement in Quality of Life with Yoga: A study compared the quality of life of yoga practitioners to non-yoga practitioners in Poland. Three hundred adults aged 30–50 years were included in two groups. Results revealed higher quality of life scores with more life & health satisfaction in the yoga group. Participants repeatedly reported a close relation of their yoga practice to a better quality of life. 93 A systematic review on RCTs with 752 participants aged over 60 years, implicated that yoga brought statistically significant improvement in health-related quality of life and mental wellbeing. 94 A cross-sectional study on 3164 participants from 39 countries explored Quality of Life with a 100-day virtual yoga intervention. The positive changes were noted in all domains pertinent to health, healthy lifestyle, stress, workplace productivity, and keeping healthy during the COVID-19 pandemic. 95 Long-term meditation practice was associated with increased benefits. Further, tele-rehabilitation with yoga as an intervention has been found to be more convenient and effective to reach masses. This, however, requires community-based digital education and/or equipment sharing. 22 Moreover, yoga has been shown to be effective in managing acute and chronic spinal pain, with superior results in improving quality of life and mood of the patients in comparison to the active exercise group86, 92 and in sedentary patients with arthritis as a control. 83
Integration of Yoga and Ayurveda
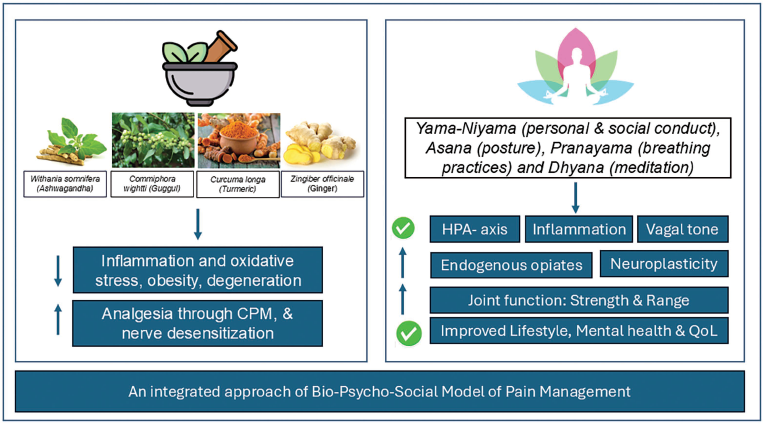
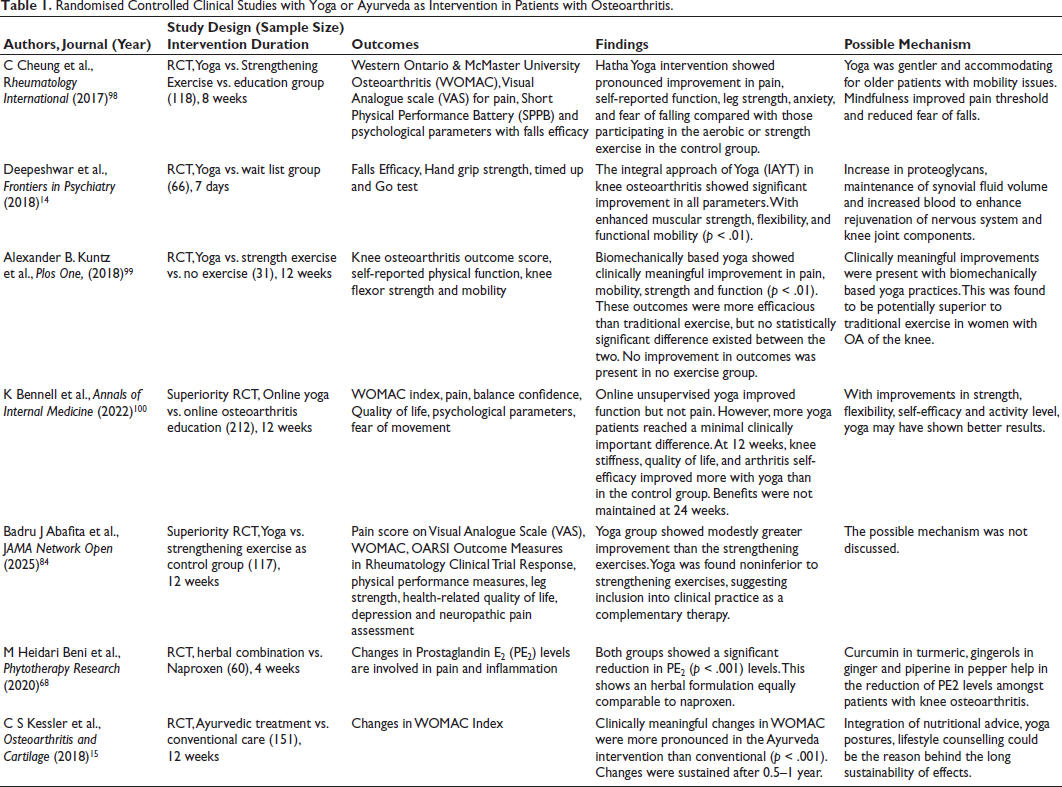
Because OA pain is multifaceted, a biopsychosocial strategy that incorporates both yoga and Ayurveda provide a thorough approach to address pain processing, central sensitisation, and neuroinflammation (Figure 1). Pharmacological therapies mostly target the management of peripheral symptoms, whereas yoga and Ayurveda target the underlying neuroimmune dysregulation by working on the psycho-neuro-immune-axis that contributes to the persistence of chronic pain.31, 96 Yoga and Ayurveda pose positive results in managing obesity, which plays a pivotal role in OA.97–99 The increased mechanical load, as well as adipose tissue dysfunction, adversely impacts immune cells that can lead to central sensitisation. 97 Further, Ayurveda promotes food as medicine, and yoga promotes healthier eating behaviours. 100 Thus, the two approaches bring about positive lifestyle changes in the individual. There exists an analogy at the theoretical aspect of the two with, Triguna theory of Yoga (Satva, rajas and tamas) seeking a balance among the three components, like the tridosha (Vata, pitta and Kapha) theory of Ayurveda. Together, these two can provide better health outcomes in OA management. Table 1 shows various RCTs that used yoga and Ayurveda in managing OA.
Randomised Controlled Clinical Studies with Yoga or Ayurveda as Intervention in Patients with Osteoarthritis.
Future Directions
Although integrative approaches like yoga and Ayurveda have shown promise in managing OA, several critical gaps hinder their widespread clinical adoption. There is a pressing need for high-quality, large-scale RCTs with strong methodology, appropriate blinding, and long-term follow-up to generate strong evidence for their efficacy and safety. 77 Most existing studies suffer from small sample sizes, heterogeneous outcome measures, a limited theoretical framework, a rationale for the choice of the comparator and variability in intervention delivery, limiting their generalizability. 101 Further, the lack of standardised therapeutic protocols for Yoga and Ayurveda remains a significant barrier. Currently, interventions vary widely in terms of duration, intensity, sequencing, dosage, and practitioner expertise. Standardising these practices, while allowing for some degree of variation, is crucial for reproducibility and comparison across studies. The development of consensus guidelines informed by traditional texts and clinical evidence would enhance scientific rigour and acceptance in mainstream healthcare. 102 Integration of modern biomedical tools, such as neuroimaging and biomarker-based assessments, is essential to elucidate the mechanistic underpinnings of these therapies. Functional MRI, PET scans, and inflammatory or neurotrophic biomarkers can help demonstrate how mind-body interventions modulate neural circuits involved in pain perception, inflammation, and central sensitisation. This integration will facilitate translational research and validate the neurophysiological basis of traditional practices.
Moreover, ayurveda-driven personalised medicine approaches, including Prakriti-based stratification, offer an innovative path forward. Interestingly association of Prakriti with genomics has already been established. 103 Ayurveda’s emphasis on individual constitution (Prakriti) aligns with current trends in precision medicine and could be systematically evaluated as a stratification tool for optimising intervention outcomes. This would allow tailoring of therapies to individuals’ biological and psychosocial profiles, potentially enhancing efficacy and adherence. Digital health platforms and telerehabilitation offer scalable solutions for delivering these interventions, especially in underserved or rural areas, which constitute two-thirds of India and harbour an elderly population requiring more medical care rehabilitation services. Incorporating virtual delivery models can reduce barriers to access, ensure continuity of care, and support long-term behavioural change. 104
Future research should therefore aim to develop an evidence-based, individualised, and technology-enabled integrative care model for OA, which not only addresses symptomatic relief but also targets disease mechanisms, including central sensitisation, ultimately reducing dependency on long-term pharmacotherapy, for a healthier tomorrow.
Conclusion
The interplay between neuroinflammation, central sensitisation, and chronic pain in OA necessitates a paradigm shift in its treatment strategies. Conventional pharmacological interventions, while effective in managing acute pain and inflammation, fail to address the underlying neurobiological mechanisms contributing to chronic OA pain. Ayurveda and Yoga offer a promising, integrative approach to OA management, providing neuroprotective, anti-inflammatory, and autonomic regulatory benefits. Ayurvedic herbs such as Ashwagandha, Guggul, Ginger and Curcumin act through cytokine modulation and oxidative stress reduction, while Yoga, Pranayama, and mindfulness-based interventions enhance neuroplasticity, regulate the HPA axis, and improve endogenous pain inhibition. Together, the two approaches work holistically on the bio-psycho-social model of the individual with a potential contribution towards eudemonic wellbeing. In addition to assessing the therapeutic potential of Ayurvedic and yoga-based therapies in regulating pain pathways, this review combines recent studies on neuroinflammation and central sensitisation in OA. This comprehensive viewpoint on indigenous medical approaches, combining knowledge from clinical research, neurology, and traditional medicine, will add value to managing the global rise in the burden of OA.
Footnotes
Acknowledgement
We are thankful to Patanjali Research Foundation for the administrative support and Dr Neha Sharma & Dr Pooja Nadholta for helping with an initial review of the article.
Authors’ Contribution
KB conceptualised, prepared first draft and graphics for the manuscript, AV provided guidance & administrative support for research, AB ensured administration support. All authors have reviewed the manuscript and provide approval for publication.
Data Availability
Available upon request to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
Not applicable.