
Abstract
Background
Internet has become a necessity among adolescents in recent years. The accessibility of Internet and associated platforms for adolescents is a major problem which is leading to Internet Addiction (IA). Adolescents spend plenty amount of time playing online games, chatting on various social media platforms, using shopping websites, watching pornographic content, etc. Excessive use of Internet can quickly become ingrained, which can result in anxiety, low self-esteem, boredom and warped perceptions of reality.
Purpose
The study aimed to explore the therapeutic effectiveness of Motivational Enhancement Therapy (MET) on IA, along with anxiety and low self-esteem in adolescents.
Method
A Single case report method is used in this study. We present a case of a 17-year-old male presented with the chief complaints of overuse of Internet, disturbed sleep, poor academic performance, irritability, and increased aggression over the last three and a half years. As per the parents, his internet usage has increased since the COVID-19 lockdown. This case report focuses on the brief case history with the detailed assessment and psychotherapeutic formulation of the case. A total number of 12 sessions in 3 phases of MET were taken, and the pre- and post-therapeutic assessments were also done.
Results
As per the post-therapeutic assessment, the changes in the symptoms were seen in the client along with improved academic performance. As reported by parents of the client, the client now uses internet for his academic requirements and for some recreational time too.
Conclusion
MET is an effective technique not only for substance addiction but also for IA among adolescents. It can be used as a brief intervention for those facing challenges to overcome from IA.
Introduction
The notion of internet addiction (IA) refers to excessive, compulsive and maladaptive use of the internet that significantly interferes with daily functioning, social relationships, and psychological well-being. Individuals with IA may prioritise being online over responsibilities such as academics, work, personal hygiene or interpersonal connections.1, 2 It is considered a behavioural addiction because it shares features with substance-related addictions, including craving, tolerance, and withdrawal-like symptoms, and it can encompass various online activities such as gaming, social networking or general browsing. 3 Adolescent IA has become a growing global concern, with prevalence rates varying significantly across regions. Studies indicate that 24.6% of adolescents in India suffer from IA, and even prior to the COVID-19 pandemic, 65% of teenagers exhibited mild, moderate, or severe levels of online addiction.4, 5 Excessive internet use among adolescents has been associated with a range of negative consequences, including psychological, cognitive and social impairments. Prolonged engagement online can lead to fixation and detachment from real-world activities, causing adolescents to lose interest in offline relationships and experiences. 6 This pattern of use is linked with increased risk-taking behaviours, impaired critical thinking, heightened conflict in family and peer interactions, and the emergence of mental health issues such as anxiety and depression.7–9 Adolescents may turn to the internet as a form of escapism, which further reinforces dependence and reduces their ability to manage real-life stressors effectively. 10 Several studies have identified a strong correlation between IA and elevated levels of stress, anxiety, and depression among adolescents. For instance, a cross-sectional study conducted in Jeddah, Saudi Arabia, involving 462 adolescents aged 12–18 years, found that 68% exhibited mild to moderate levels of IA. Furthermore, higher IA scores were significantly associated with increased levels of perceived stress, anxiety, and depression. 11 IA has been consistently associated with increased levels of loneliness and decreased self-esteem among adolescents. A meta-analytic review encompassing multiple studies found a significant negative correlation between IA and self-esteem, indicating that higher levels of IA are linked to lower self-esteem in adolescents. 12 Furthermore, a study conducted in Kashmir reported a significant positive correlation between IA and loneliness, suggesting that adolescents with higher IA scores tend to experience greater feelings of loneliness. 13 These findings underscore the adverse impact of IA on adolescents’ psychological well-being, highlighting the need for targeted interventions to address these issues. Pornography addiction represents a salient form of harmful Internet use that is increasingly attracting adolescents. A recent scoping review documented that excessive pornography consumption in this group is associated with a spectrum of psychological sequelae, including irritability, impaired concentration, stress, guilt, frustration, depressive symptoms, sleep disturbance, and psychosomatic complaints. 14 Interpersonally, affected adolescents often withdraw socially, struggle to initiate or sustain relationships, prefer solitude, and experience feelings of alienation. 14 Neurophysiological evidence summarised in the same review indicates a predominance of delta activity in the prefrontal cortex on quantitative electroencephalography, signifying reduced executive cognitive function; this dysfunction may erode adolescents’ ability to exercise moral judgement and inhibit maladaptive behaviour. 14
Motivational Enhancement Therapy (MET) is a client-centred, directive therapeutic approach designed to facilitate behavioural change by helping individuals resolve ambivalence. Rooted in the principles of Motivational Interviewing, MET emphasises collaboration between therapist and client, focusing on eliciting intrinsic motivation rather than imposing external directives. This method has been effectively applied to various behavioural issues, including substance use disorders and behavioural addictions like IA. In the context of IA, MET has shown promise in reducing maladaptive behaviours. For instance, a study conducted in Thailand implemented a group activity-based MET program among junior high school students. The intervention led to significant reductions in social media usage, emotional behaviour issues, and depressive symptoms compared to a control group. These findings suggest that MET can be an effective component in treating internet-related behavioural addictions.15, 16
Method
A single case report method is adopted. The adolescent was reported to be using excessive Internet in various forms, like using social media, playing online games, watching web series on OTT platforms, etc. After taking a detailed case history and Mental Status Examination, the psychological assessments and baseline measures were conducted on him. A total of 12 psychotherapeutic sessions of MET were conducted. After completion of sessions, post assessments were done, and two follow-up assessments were also conducted after three and six months, respectively.
The Case
Mr A, a 17-year-old male, studying in class XI in a school in Lucknow, belongs to middle socio-economic status, briefed his chief complaints as overuse of the Internet, disturbed sleep, poor academic performance, irritability, and increased aggression since the last three and a half years. His father also reported that sometimes he observed his child used to lock himself in the room, and most of the time he usually skips his meals too. The boy reported that he had not felt any interest in academics in the past three years, as he uses his mobile phone to surf different sites for around 10–11 hours per day. He performed poorly in his 10th-class Board examinations. He also likes to play online games specifically related to pornography. After two to three sessions he also mentioned that he likes to surf porn sites and spends his most of the time to see porn videos. He reported that when he does not see these videos, he feels so restless, along with palpitations and irritability. His father also mentioned that once he caught him watching porn video in his room during night, he was shocked and disgusted at the graphic images, some of which involved gay sex and group sex as well. He confronted him, and he became outraged, defensive and accused him of violating his privacy. He used to become angry, hostile or irritable when asked to stop using mobile phones. Later, he accepted that he is now addicted towards pornography and feels a craving to see it. Parents also reported that he even becomes hostile and used to become destructive sometimes if the parents become strict towards his studies or ask him to cut down his internet use. He presented for treatment by the family after becoming increasingly more agitated, restless, ashamed and ‘fed-up’ with himself. The Client was well-kempt and tidy, in touch with surroundings, eye contact was maintained with the examiner, rapport established easily. The attitude towards the examiner was cooperative, the motor behaviour was normal, speech was relevant, coherent and goal-directed with nil deviation. Cognitive functions were intact. Affect was irritable, communicable, and appropriate. In thought content, Ideas of guilt were present, no abnormality detected in perception. Judgement was intact, with Grade Level 2 Insight. The client was at the pre-contemplation stage of motivation, and the locus of control was external.
He reported the following symptoms while taking a detailed history: I feel powerless to resist the urge to view pornographic content. I frequently spend more time and energy browsing the Internet than I initially intended. I have made many unsuccessful attempts to limit or stop viewing pornographic content or playing online games. I spend a significant portion of time viewing porn, thinking about porn or engaging in activities that will enable access to porn and online games. I neglect family, social or work obligations to use my mobile phone and laptop. I continue to use excessive internet despite experiencing negative consequences. I feel anxious, stressed, or irritable if I am unable to access the Internet for gaming, chatting or using mobile phones. I feel that I am not worthy to study in a good school.
Test Administered/Baseline Assessment
IA Test
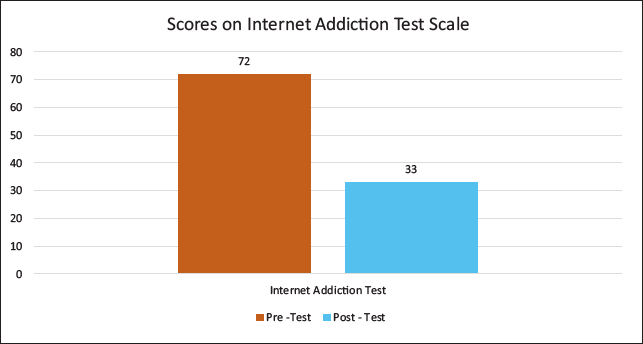
This test was administered to measure the presence and severity of Internet dependency in the patient. His score was 72 in this test, which suggests a Moderate level of IA.
Hamilton Anxiety Scale
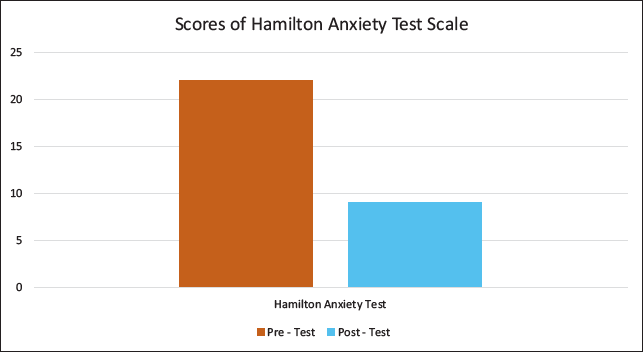
The total score on this scale was 22, which indicates Mild to Moderate severity of Anxiety.
Academic Performance Scale
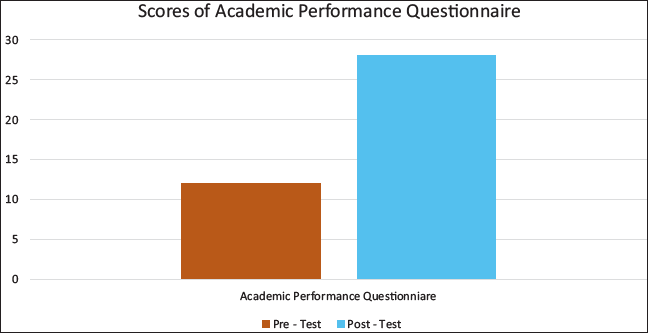
The score was 12, indicating poor academic performance.
Readiness to Change Questionnaire
Pre-contemplation = 8, Contemplation = 2, Action = 0.
Target Areas for Therapy
To provide detailed information regarding the nature, course & outcome of excessive internet use.
Build and enhance motivation to change for the overuse of the Internet and habit of watching pornography.
Enhance coping skills to prevent relapse.
Rationale of the Therapy
The client had low motivation and was in the pre-contemplation stage. Mr A. had a history of relapse and struggled to maintain his abstinence. Thus, during the acute period, it is vital to increase motivation and identify high-risk situations that may lead to relapse in the client. Coping skills are crucial in the long-term management plan to help the patient maintain their abstinence.
Structure of the Therapy Sessions
A total of twelve MET sessions had been scheduled based on symptomatology, clinical case history, mental state examination, and test results. Each session lasted between 45 and 60 minutes, and the goals were determined based on an agenda created by the client and therapist together. Pre, post, and follow-up assessments were done to assess the effectiveness of the MET techniques. After completion of every session, the summary was given to the client and along with that, feedback was taken.
Initial Phase:
Four sessions were planned for the initial phase of the therapy. The first session was conducted with the goals of building rapport and conducting of assessment. After that, MET was introduced to the parents and the client. Open–ended discussions were made to allow the client to share his concerns. The administration of IAT was done, and the score was 72, which suggested the severity of IA was at Moderate Level. Readiness to change Questionnaire was also used in this session, where the client scored 8 in Precontemplation, in contemplation he scored 2, whereas in Action stage he scored 0, which suggests the client was in contemplation stage of the readiness to change. The stages of change model was introduced to the client, and he was psycho-educated about the process of the therapy in detail. In the second and third session, the goal was to make the client understand ambivalence towards change and provide feedback to increase discrepancy between goals and current behaviour. The Decisional Balance exercise was introduced to the client where with the help of therapist, he explored the pros and cons of internet use. The identification of internal conflict, that is, enjoyment versus academic and family stress, was also done. The therapist reinforced the client’s autonomy and asked the client to think about the goals which is suitable and feasible for the client. The client reflected his feelings in the following way ‘I am aware that the overuse of internet is affecting my studies and interpersonal relationships but that is the only thing which makes me feel good’. The client was then informed in detail about the consequences of overusing of internet and gadgets on the brain and behaviour. The use of internet by the client was also compared with the peer norms based on available research. The client was then asked to assess and discuss his life goals and compare them with his current behaviour. This session helped the client to understand the consequences which are directly affecting him, and he was surprised by getting this insight, but at the same time, he was also defensive about his overuse of Internet. At the end of the session, he agreed to monitor his Internet usage for a week. The client’s motivation was again assessed, and he was in contemplation stage. The techniques used in these two sessions were Decisional Balance Worksheet, double–sided reflections, feedback report, affirmations, normalisation and encouragement. Session 4 was focused on strengthening the motivation for change in the client. The client came with his review about his daily use of the internet, which was up to 10–11 hours a day. With the help of a therapist, the future goals were explored, which came out to be working hard for his examinations and making new friends. The discussion related to how the internet use is hampering his future goals was made, and how he can overcome this barrier. The client said, ‘Maybe I don’t need to quit the use of internet completely, but I can control its usage’. The client was on transition to preparation stage of Motivation. The techniques which were used were importance/confidence rulers and eliciting change talk.
Middle Phase: The 5th and 6th sessions were focused on developing SMART goals for reducing excessive internet use and enhancing copying skills for high-risk situations. The realistic goals were set, and the use of the Internet was reduced to seven to eight hours per day over four weeks. The behavioural substitution, like reading books, walking, meeting friends and spending an hour on outdoor sports, was also introduced. The client was asked to monitor and track the time and emotions while using the change plan worksheet. The common triggers were identified, such as stress, boredom, alone time and based on that, new healthy coping strategies were developed, such as activity scheduling, exercise and limited use of apps. The urge–surfing technique was introduced for cravings to use mobile phones or play online games. In the next two sessions (sessions 7 and 8), the goals were to review the progress and troubleshoot the lapse that happened during the time of examination. The reasons for lapse were explored without judgement, and it was reframed as a learning opportunity. The external support strengthening was also introduced in session 8, where the client explored his reluctance to share the goals with family and friends. Mr A’s sibling was also involved in the therapeutic process to take accountability for the client. To manage peer pressure related to online gaming was also discussed, and assertive communication skills were introduced, such as ‘for me it’s time to play cricket instead of online game’. The client agreed to be reminded by the sibling about the screen limit as and when required. The techniques used for this session were role-playing, affirming and values clarification.
Terminal Phase: Sessions 9 and 10 were focused on reinforcing identity change and developing a long-term change plan. The goals were to support identity away from ‘Internet addict gamer’ self-perception and to create a suitable overall recovery plan. The client was asked to recall his hobbies and skills during pre-addiction. Reconnection with past activities like playing football, chess and playing guitar was introduced. The client was also asked to develop self-affirmation statements like—I can do well in studies, I am a strong determinant, I can achieve my goals with hard work. Finalisation of internet use limit was done in the 10th session, and client was asked to keep four to five hours per day as his maximum screen time, which includes breaks in between. A weekly outing was also planned with the family to avoid boredom in the schedule and to enhance interpersonal relationships among the family members. He was also advised to track his app usage by installing the software on his phone and laptop. While ending the session, 10 clients quoted that ‘I miss my old days which were IA free, I wanted to relive that stress and anxiety free life again’. The techniques which were used in sessions 9 and 10 were Identity mapping, self-efficacy building, lifestyle balance wheel and contingency planning. The 11th session was aimed to prevent relapse and to practice coping strategies in the session. Here, the high-risk situations were reviewed and responses towards those were analysed. The relapse response plan was developed with contacts and steps. In this session, the techniques used were coping cars and rehearsal of relapse protocol. Session 12 was the last session of the therapy, where the goals were to consolidate gains, celebrate success and preparation of future goals. The client mentioned that the internet usage is now reduced to four to five hours per day which included his academic-related work as well, he resumed his school and coaching centre, and his anxiety symptoms were also improved. Client expressed on the process via a guided letter to past self. The therapist also discussed about the possible booster sessions and the journaling method too. The techniques used in last session were reflection, closure ritual and future pacing. A booster session was planned to review progress after a month of termination.
Results
The post-assessment tests were done after completion of 12 sessions of MET. In IAT, he scored 33, which suggests a mild level of IA (Figure 1). In the Hamilton Anxiety Test, the score was 9, suggesting a mild level of anxiety severity (Figure 2). The score of Academic Performance Questionnaire was 28, indicating good performance (Figure 3). The overall score of post-assessment test after application of MET was positive, which indicated that the MET is an effective therapy for the management of IA among adolescents. As reported by the parents, Mr A started focusing on his studies and stopped being aloof and self-centred. He has also started showing interest in sports and music, along with spending time with family and friends.
Graph Showing the Pre-intervention and Post-intervention Scores on the Internet Addiction Scale.
Graph Showing the Pre-intervention and Post-intervention Scores on the Hamilton Anxiety Scale.
Graph Showing the Pre-intervention and Post-intervention Scores on the Academic Performance Questionnaire.
Discussion
IA among adolescents has emerged as a growing behavioural concern, often associated with comorbid symptoms such as anxiety, low academic performance, and social withdrawal.1, 5 Traditionally, treatment modalities have included psychoeducation, behaviour modification techniques, and, in some cases, pharmacological interventions.3, 4 However, the present study aimed to establish the therapeutic significance of MET in treating IA among adolescents.
MET is a brief, person-centred intervention approach grounded in the transtheoretical model of change and has been widely used in the treatment of substance use disorders. 15 With its focus on resolving ambivalence and strengthening intrinsic motivation, MET has shown efficacy in modifying maladaptive behaviours such as excessive digital engagement.14, 15 Several studies have demonstrated the effective application of MET in reducing problematic internet use and enhancing treatment compliance among adolescents.14, 15
The findings of the present study align with existing literature and demonstrate a marked reduction in IA severity following a structured MET protocol. The client’s Internet Addiction Test (IAT) score was reduced from 72 (moderate) to 33 (mild), consistent with prior findings supporting MET’s role in managing behavioural addictions. 14 Furthermore, the client showed a significant decrease in anxiety symptoms, as reflected by the Hamilton Anxiety Scale, which is in line with studies suggesting a bidirectional relationship between anxiety and excessive internet use.10, 11
Additionally, improvements were observed in the client’s academic functioning, with performance scores increasing from 18 to 28. This outcome supports earlier research indicating that therapeutic reduction in IA can lead to enhanced academic motivation and improved school performance. 13 Techniques, such as decisional balance, eliciting change talk, relapse prevention planning, and family involvement, were instrumental in achieving and sustaining these changes, as supported by previous work on MET-based interventions in adolescents.14, 15
Although the study presents promising outcomes, the findings are limited by the single-case design. Future studies should focus on controlled trials with larger adolescent samples to better understand the long-term efficacy and generalisability of MET in the treatment of IA.
Conclusion
Problematic Internet use is a major concern among adolescents and young people. The problem is escalating as technology advances and the Internet, gadgets, and other tools become more accessible. Unlike substance addiction, managing IA presents a difficulty for healthcare providers because their availability and other obligatory uses play a significant role in lapses and relapses. MET is one of the most successful approaches for substance use disorders, coupled with relapse prevention techniques. Its efficiency has also been demonstrated in problematic internet use and pornography addiction. The present study highlights the potential of MET as an effective psychotherapeutic approach for IA in adolescents. With its structured and client-centred framework, MET can be utilised not only in substance-related conditions but also as a brief intervention for behavioural addictions such as problematic internet use among adolescents as well.
Footnotes
Abbreviations
AD: Anshuma Dubey
SS: Shivali Sharma
MP: Madhurima Pradhan
SZHZ: S. Z. H. Zaidi
Authors’ Contribution
All authors contributed to the study’s conception and design. Research conceptualization, data sorting, analysis, and duplication checks were performed by AD, SS, MP, SZHZ. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The written informed consent was taken from the parents and assent form was taken from the client to participate in the study. Client was briefed about their voluntary participation and confidentiality of their responses.
Statement of Ethics
This study was performed in line with the principles of ICMR and World Medical Association Declaration of Helsinki. The approval was granted by Ethics Committee of Amity University Uttar Pradesh Lucknow Campus.