
Abstract
Background
In young patients, improving post-surgery quality of life is vital. A critical lacuna in glioma resections is the absence of tract-specific digital tests to safeguard cognitive functions.
Objective
This study aimed to assess cognitive impairment in patients with pre-frontal low-grade gliomas (LGG) involving the superior longitudinal fasciculus (SLF).
Material and Methods
The current study documented cognitive impairment using the battery of tests temporarily licensed from The Many Brains Project (TMB) in patients who underwent surgery for pre-frontal LGG with radiological evidence of involvement of the SLF.
Results
Post-operative neuropsychological evaluations in patients with SLF lesions revealed significantly reduced cognitive performance compared to healthy participants. These deficits were evident in tests such as Simple Reaction Time, Visual Patterns, Digit Symbol Substitution, Digit Span, Attention tasks and Trail Making Tests.
Conclusion
Functional domains like attention, working memory and executive function may be affected in patients by both the tumour and neurosurgical intervention. Based on these results, we recommend using Reaction Time, Digit Symbol Substitution, Multiple Object Tracking and Trail Making Tests as practical cognitive evaluation tools, complementing traditional Intraoperative Neurophysiological techniques.
Keywords
Highlights
Involvement of the Superior Longitudinal Fasciculus (SLF) is associated with an increased risk of cognitive impairment.
Reaction Time, Digit Symbol, Multiple Object Tracking and Trail Making tests- practical tools to assess cognition in SLF lesions.
Incorporating cognitive assessment with conventional mapping tools may minimise cognitive deficits during brain tumour resection.
Introduction
The structural integrity of grey and white matter in the brain is essential for its functional integrity. Gliomas primarily treated by neurosurgical interventions can result in iatrogenic cognitive dysfunction due to the excision, particularly near eloquent cortical regions. This presents a challenge as therapeutic interventions aimed at maximising survival through tumour resection, chemotherapy, or radiotherapy must also prioritise preserving cognitive function to maintain the patient’s quality of life. 1 Cognitive impairment has been reported in 27%–83% of adults with low-grade glioma (LGG) 2 and improving the quality of life in patients after glioma resection surgery is a key focus for neurophysiologists, given the high survival rate, with efforts directed toward preventing post-operative neurocognitive impairments.
Previous work done related to neurocognition in brain surgeries considers the pre-frontal cortex (PFC) as a critical region often affected in these surgeries, as it is essential for higher-order functions like attention, cognition and emotional regulation. 3 The Human Connectome Project has greatly contributed to our understanding of these connections by using Diffusion Tensor Imaging (DTI) to map how anatomical connectivity supports functional outcomes.4, 5 Various neurosurgical centres utilise pre- and intra-operative assessments to monitor cognitive impairment and to minimise the risk of cognitive functional loss during surgery. 6
This article focuses on the role of white matter tracts, specifically the superior longitudinal fasciculus (SLF), in maintaining cognitive functions. SLF, which connects the frontal cortex with temporal and parietal regions, is essential for tasks like spatial attention, language processing and visuospatial functions. 7 While anatomically adjacent to the arcuate fasciculus—which links frontal and temporal lobes—the SLF is better described as a frontoparietal pathway involved in attention, working memory and executive control. Identifying the white matter tracts involved is critical for preserving cognitive functions during glioma resections, as research has shown that preserving these tracts significantly enhances post-surgical quality of life.8–12
The current study aimed to document cognitive impairment in patients who underwent surgery for low-grade pre-frontal glioma with radiological evidence of involvement of the SLF white fibre tracts. Neurocognitive assessment was conducted using a battery of tests temporarily licensed from The Many Brains Project (TMB), 13 a global citizen science initiative that has collected cognitive data from over 2 million volunteers worldwide. Based on these findings, the study may help identify the most suitable neurocognitive or neuropsychological tests for dynamic sub-cortical mapping of the SLF.
Material and Method
Subjects and Ethical Clearance
The current study was a cross-sectional study. Once the Institute Ethics Committee approved for research on human subjects, the study was conducted in Department of Physiology in collaboration with Departments of Neurosurgery, Neuroradiology and Interventional Radiology.
The study included 23 patients (Mean age = 36.7 ± 8.4 years with a range: 24–52 years; 12 male and 11 female) as well as 25 healthy subjects (Mean age = 36.5 ± 7.9 years with a range: 23–50 years; 15 male and 10 female) who volunteered to be a part of the study. An independent samples t-test showed no significant difference in age between the two groups (p = .91), indicating that they were well-matched for age.
The patients who were operated for pre-frontal lesion and showed involvement of SLF on MR/DTI were recruited for the study. These patients were then called for a follow-up on days designated by the consulting surgeon in the outpatient clinic.
MRI scan was acquired with 3T Philips Machine (®Ingenia Elition), at the NMR and MRI facility of AIIMS, New Delhi, using the 32-channel head coil. Standard tumour protocol and special sequences were acquired. 3D T1, 3D T2, 3D Flair, SWI, DTI-128 directions, T1 perfusion, T2* perfusion, 3D T1+C DTI were obtained using an echo-planar imaging sequence with a b-value of 1000 s/mm2, 128 uniform directions, and a matrix size of 104 × 100 with a 2-mm isotropic spatial resolution. TR/TE equals 2618/84 ms, and the slice thickness was 2 mm. The examination time of this sequence was 05.44 min. Acquired data was processed in Philips ®IntelliSpace Portal, and the white matter tracts were automatically delineated. Qualitative assessment of involvement of SLF (deviation vs disruption) was done by a qualified neuroradiologist.
Neuropsychological/Neurocognitive Assessment Domains
After excluding possible postoperative issues (such as sensory and motor deficits) through neurological examination that could affect test outcomes, neurocognitive assessments were conducted using the web-based platform TestMyBrain (Table 1).
Neurocognitive Evaluation Tests Selected from the TestMyBrain Module, Along with the Specific Parameters Assessed in Each Test.
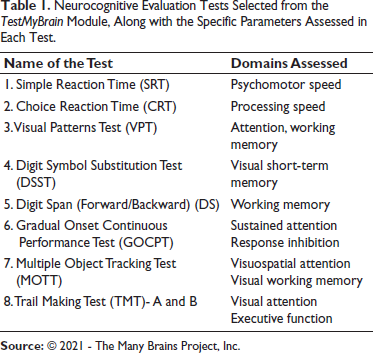
The patients recruited for the study underwent a battery of neuropsychological and neurocognitive tests. Upon completion of each test, the software generated both an absolute score for the patient and a normative reference score, which corresponds to an age- and gender-matched population from the TMB Database. The individual’s absolute score and their software-generated normative reference score were noted for statistical analysis.
Data Analysis and Statistics
The analysis involved comparing the performance scores of two distinct groups: patients and a healthy population. Each individual’s score was compared against software-generated normative reference scores initially. Following this, the average scores for each test in the battery were calculated for both the patient and control groups.
To compare the average scores between the patient and control groups, statistical tests were applied using the IBM SPSS Statistics for Windows, Version 29 (IBM Corp., Armonk, NY, USA). Given that the data distribution for the test parameters followed a Gaussian distribution, the results were expressed as Mean ± Standard Deviation (Mean ± SD). A p value was calculated to assess the significance of differences between the average scores, with a p value less than .05 considered statistically significant.
Results
Neuropsychological/Neurocognitive Evaluation in Patients Operated for Lesion Involving SLF
Twenty-three patients (12 males and 11 females) with an average age of 36.73 years performed the Neuropsychological/Neurocognitive Tests. Upon completion of the tests, absolute scores and the corresponding normative reference scores of age and gender matched population were obtained from the TMB Database (Table 2).
Average of Absolute Scores and Normative Reference Scores in the Tests for Neurocognitive Evaluation in the Patients Operated for Pre-frontal Lesion Involving SLF.
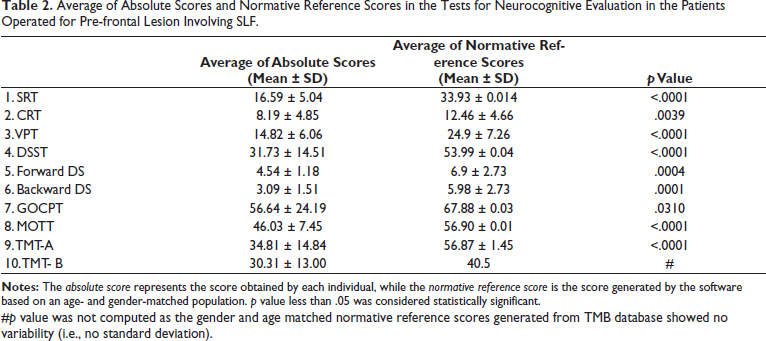
#p value was not computed as the gender and age matched normative reference scores generated from TMB database showed no variability (i.e., no standard deviation).
As evident from Table 2, patients with lesions involving SLF showed significantly lesser performance as compared to age and gender matched population. All tests show a significant difference in average values of absolute scores as compared to their corresponding normative reference scores of age and gender matched population.
The scores in the patient group showed variability, with many individuals deviating from their normative scores. These deviations indicate that the patients’ cognitive or functional performance often did not match the expected levels according to the normative data.
Neuropsychological/Neurocognitive Evaluation in Healthy Subjects
Twenty-five healthy volunteers (15 males and 10 females) performed the Neuropsychological/Neurocognitive Tests. Upon completion of the tests, absolute scores and the corresponding normative reference scores of age and gender matched population were obtained from the TMB Database. Table 3 shows the average of absolute scores and normative scores for each test in the neuropsychological/neurocognitive evaluation for the healthy control group.
The Average of Absolute Scores and Normative Scores for Each Test in the Neurocognitive Evaluation for the Healthy Control Group.
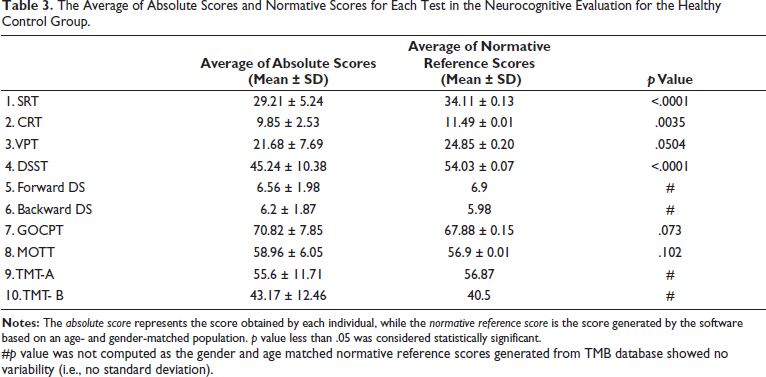
#p value was not computed as the gender and age matched normative reference scores generated from TMB database showed no variability (i.e., no standard deviation).
The healthy population performed close to their normative reference scores, with smaller deviations observed. Most individuals in this group had scores that either matched or were slightly above their normative expectations.
Neuropsychological/Neurocognitive Evaluation in Patients and Healthy Subjects
Twenty-three patients and 25 healthy volunteers performed the Neuropsychological/Neurocognitive Tests. Upon completion of the tests, absolute scores are noted. For each test, the average of the absolute scores of the patient group is compared with that of the healthy control group. p value is calculated between the average scores for analysis and interpretation.
As evident from Table 4 and Figure 1, among the absolute scores, all tests showed a significant difference between the patient and healthy groups, except for choice reaction time (CRT). Post-operative neuropsychological/neurocognitive evaluation in patients with lesions involving SLF showed significantly lesser performance as compared to healthy participants in Simple Reaction Time, Visual Patterns Test, Digit Symbol Substitution Test, Digit Span Test, Tests for Attention-Gradual Onset Continuous Performance Test and Multiple Object Tracking Test and Trail Making Test.
Comparison of Neurocognitive Evaluation in Patients with Lesion Involving SLF and that of Healthy Participants.
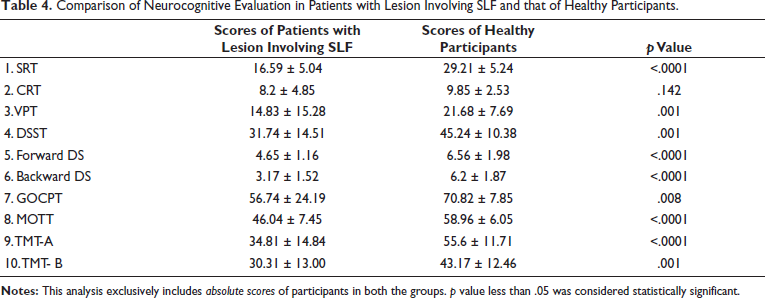
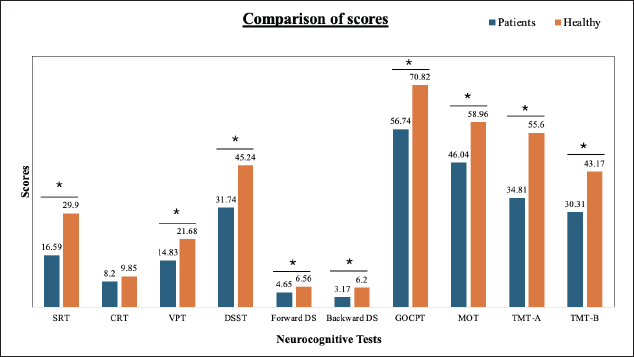
Interestingly, CRT was the only test in which patients did not show a statistically significant difference compared to controls. The average CRT scores were comparable between groups, despite notable differences observed in other reaction time and executive function tests.
Neuropsychological/Neurocognitive Evaluation in Patients with Left Versus Right Sided SLF Involvement
Among the 23 patients, 10 had left SLF-involving gliomas and 13 had right SLF involvement. When categorised by lesion laterality, cognitive performance showed some domain-specific variations. Simple reaction time and visual pattern recognition scores were largely comparable across groups. However, patients with left SLF gliomas showed relatively better performance. on CRT, digit symbol substitution, concentration tests, and Trail Making Test-B, suggesting potentially preserved or compensatory executive and attentional functions. In contrast, patients with right SLF involvement performed better on the digit span test and Trail Making Test-A, indicating relatively better working memory and psychomotor speed. Although these findings did not reach statistical significance due to sample size constraints, they suggest a possible lateralisation effect consistent with established functional distinctions between the left and right frontoparietal networks.
Discussion
Global Underperformance in the Patient Group
In this study, it is found that the patients operated for LGG in the PFC involving SLF showed consistent underperformance in the battery of neurocognitive tests advocated. The underperformance noted is with both normative data generated by the TMB database as well as the healthy counterparts.
It is also observed that the psychomotor speed and processing speed as tested by Reaction Time showed significant differences between both the patient and healthy control groups and their respective normative data. However, tests for working memory (Matrix Reasoning, Digit Symbol Matching and Digit Span); attention (Gradual Onset Continuous Performance Test, Multiple Object Tracking) and executive function (Trail Making Test) showed significant differences between patient group and their normative reference scores. The scores for the testing domains between healthy control group and their normative reference scores were comparable. These findings suggest that lesions involving SLF have an impact on the domains such as attention, working memory and executive functioning.
When the average scores of the patient group are compared with that of the healthy control group, it is noted that all the tests showed significant differences except for CRT.
The preserved performance in CRT, despite SLF involvement, warrants further interpretation. While this finding may reflect limitations such as a relatively small sample size or variation in age and follow-up intervals, an additional explanation involves neural compensation. CRT, being a more complex reaction task, likely engages broader and more bilateral networks than tasks involving simpler executive functions. When the SLF is compromised, parallel pathways—including contralateral homologous fibres or alternative tracts—may assume a compensatory role, supporting task performance.
Moreover, CRT’s bilateral engagement could allow the unaffected hemisphere to contribute more significantly than in tasks that depend on lateralised attention or working memory, which are more sensitive to focal SLF damage. This observation raises important questions about the brain’s ability to adapt structurally and functionally to white matter injury. Future studies employing functional imaging or tractography-based compensation analysis could further explore the mechanisms of neural plasticity and reorganisation in this context.
Role of the SLF in Cognitive Performance
The current study supports previously reported associations between increased risk of cognitive impairment and SLF involvement as evident from the works of Incekara F et al. 2019, 9 Liu D. et al. in 2020 14 and Cochereau J et al. 2020. 15 The observed cognitive deficits in our cohort align well with the known functional roles of the SLF within the frontoparietal network. The SLF is a major dorsal white matter tract connecting the frontal and parietal lobes and plays a central role in attention, working memory and executive control. This is consistent with the impairments seen in our patients in tasks such as reaction time (choice reaction), digit span, digit symbol substitution, and Trail Making Tests A and B. These tasks are commonly used to assess processing speed, attention and executive function—domains subserved by the SLF and its associated dorsal attention network 16 and working memory circuitry. 17 There is evidence to support that SLF is involved in conditional associative tasks, spatial attention and visual working memory and language articulation. The left SLF connection is proposed to serve speech processing, while the right SLF is proposed to serve visuospatial functioning. 7
Unlike prior studies of Incekara et al. 2019, 9 Nakajima et al. 2018, 11 Vidorreta et al. 2011, 18 involvement of SLF was not correlated to the Picture Naming Test, as Sanvito et al. 2020 19 reported that involvement of SLF alone cannot be attributed to diminished performance in Picture Naming Test.
The SLF is known to be functionally heterogeneous, with lateralised involvement in distinct cognitive domains. The left SLF is more engaged in language and executive functions, whereas the right SLF supports attention, inhibition and working memory. 7 In the current study, although overall cognitive outcomes were comparable across lesion sides, certain domain-specific differences emerged. Patients with left-sided SLF gliomas tended to perform better in tasks requiring rapid choice responses, executive control and symbolic substitution, while those with right-sided lesions performed better in tasks linked to working memory and processing speed. These trends are consistent with known lateralisation patterns but must be interpreted cautiously due to the limited sample size. Future studies with larger, hemisphere-stratified cohorts are needed to further elucidate the cognitive consequences of lesion laterality in SLF-involving gliomas.
Integration of Neurocognitive Tests in Perioperative Monitoring
Neurophysiologists have complementary expertise in managing patients with LGGs with the help of dynamic subcortical mapping in addition to the already existing monitoring modalities for eloquent area neurosurgical procedures. Surgery of gliomas of eloquent areas is challenging for the double aim that it poses to the surgeon. Although its goal should be complete tumour removal, it should avoid neurological deficits to preserve the patient’s quality of life. 1 Taphoorn and Klein also state in their article that cognitive function, alongside survival rates and brain imaging responses, is increasingly recognised as a crucial outcome measure in brain tumour patients. It is also now acknowledged as an independent prognostic factor for the survival of glioma patients. 20 Advances in sub-cortical mapping and neurocognitive assessments have improved surgical precision, while digital platforms offer new opportunities for conducting behavioural experiments and neuropsychological assessments with greater accessibility and control than traditional methods. 21
Over 500 cognitive and psychological performance tests have been documented for neurocognitive evaluation, but there is no consensus on the most appropriate tests for assessing specific cognitive domains, particularly in glioma patients.21–23 Mapping of executive functions and its component psychological processes to distinct regions of the frontal lobe and or their connectivity is the central goal of research in this field. Stuss also related executive functions to specific frontal lobe regions, thus aiding our understanding in component processes in relation to specific regions of the frontal lobe. 24 Alexander et al. reported that performance on all these apparently disparate tasks is due to a failure of “Energization,” that is, the process of initiation and sustaining any response in a series of research over years.25–27
There is research going on actively in centres across the world, which is indicating the use of computerised testing for neuropsychological/neurocognitive assessment.28, 29 This relatively novel assessment method could prove useful in order to perioperative as well as intra-operative period. A clearer mapping of test outcomes to SLF-related functions helps reinforce the neuroanatomical specificity of the cognitive profile observed in SLF-involving gliomas. We believe this nuanced interpretation strengthens the clinical and scientific value of our findings.
Conclusion
To summarise, the present study demonstrated the use of digitalised neuropsychological/neurocognitive tests for the assessment of cognitive deficits in patients with LGGs in the pre-frontal area, especially involving a major white matter tract—SLF. The neuropsychological and neurocognitive tests used in this study have been proven to be validated and can be used to evaluate cognition during the brief window of time available in the operating room during an awake neurosurgical procedure.
While many tests were performed in this study, our experience in the operating room during awake craniotomies suggests that Reaction Time, Digit Symbol Substitution, Multiple Object Tracking and Trail Making Tests are the most practical and beneficial for cognitive evaluation. These should complement traditional motor, sensory and language mapping techniques in brain tumour resections, especially in proximity to eloquent areas.
The neuropsychological tests reveal multiple cognitive processes are affecting patients whose white fibre tracts have been affected as a consequence of glioma and/or neurosurgical procedures. This fits into current understanding that most pre-frontal area functions do not depend on a specific location but rather reflect brain network properties. 30 As the findings from the current study suggest that attention, working memory and executive functions—linked to frontoparietal networks subserved by the SLF—may be particularly vulnerable during resections involving this tract and mitigating cognitive deficits in SLF-involving tumours requires an integrated surgical approach. Thus, preoperative tractography to visualise and preserve the SLF, combined with intraoperative monitoring tailored to cognitive domains (e.g., attention, symbol substitution and reaction time), may help prevent damage. In awake craniotomies, tasks such as multi-object tracking or rapid-response paradigms could provide real-time feedback on functional integrity.
This study may pave a path to dwell into the correlation between tests and then location of the lesion because preservation of white matter connectivity is more important for higher mental functions than maintaining cortical integrity. 30
Additionally, identifying patients at risk for postoperative deficits allows early deployment of neurorehabilitative strategies targeting attention and working memory. These could include cognitive training programs, structured attention therapy and pharmacologic interventions where appropriate. Incorporating these elements into surgical planning and postoperative care can improve quality of life and functional outcomes for glioma patients.
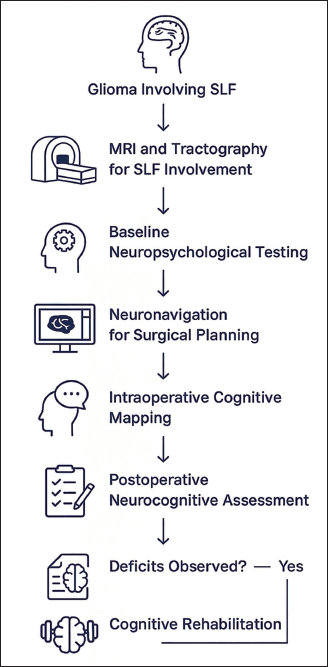
Ultimately, we propose that integrating SLF-focused cognitive assessments into the neurosurgical workflow can enhance both the oncologic and cognitive outcomes of glioma surgery and encourage future prospective studies using tract-guided resection with perioperative cognitive testing to validate and refine these strategies (Figure 2).
We also advocate for a broader adoption of white-matter–sparing neurosurgical techniques and intraoperative cognitive testing to preserve essential cognitive functions—especially in cases where the SLF is at risk.
Limitations of this Study
Though qualitative assessment of involvement of SLF was confirmed, its quantitative parameters were not assessed due to software limitations. However, quantitative data, including FA (Fractional anisotropy) and MD (mean diffusivity) values, will improve our insight into the correlation of SLF and cognitive performance in patients with affected SLF.
A key limitation of the present study is the absence of preoperative neurocognitive assessments, which constrains our ability to disentangle the contributions of tumour-related infiltration versus surgical resection on postoperative cognitive deficits. We encourage future studies to incorporate longitudinal cognitive testing (pre- and post-surgery), combined with diffusion-based tractography and intraoperative tract mapping for a clearer understanding of cognitive outcomes in SLF-involving gliomas.
Another limitation is that the heterogeneity in timing of postoperative cognitive assessment—three weeks to six months. Cognitive deficits assessed shortly after surgery may reflect transient effects such as oedema or fatigue, while later testing may capture partial recovery or compensation. This temporal variability introduces a potential confound when comparing cognitive outcomes across patients. While our current sample size precludes stratified analysis, future studies should control for post-op interval and ideally include serial cognitive assessments to map recovery trajectories.
Abbreviations
SLF: Superior Longitudinal Fasciculus
LGG: Low-Grade Glioma
PFC: Pre-Frontal Cortex
TMB: The Many Brains Project
DTI: Diffusion Tensor Imaging
MRI: Magnetic Resonance Imaging
SRT: Simple Reaction Time
CRT: Choice Reaction Time
VPT: Visual Patterns Test
DSST: Digit Symbol Substitution Test
FDS: Forward Digit Span
BDS: Backward Digit Span
GOCPT: Gradual Onset Continuous Performance Test
MOTT: Multiple Object Tracking Test
TMT: Trail Making Test
IBM: International Business Machines (in context, used for IBM SPSS Statistics)
SPSS: Statistical Package for the Social Sciences
SD: Standard Deviation
Footnotes
Acknowledgements
I extend my heartfelt gratitude to the Heads of the Departments of Physiology, Neurosurgery, and Neuroradiology for their invaluable support in patient recruitment and technical guidance throughout this work. I am deeply thankful to my family for their unwavering support and encouragement, which has been a source of strength during this endeavour.
Authors’ Contributions
Sreya Konusu: This author helped with intellectual content, study design, data collection, writing and editing all sections of manuscript for publication.
Uditi Gupta: This author helped with intellectual content, study design, data collection, writing and editing all sections of manuscript, and approving manuscript for publication.
Tania Talwar: This author helped with study design, data collection, writing and editing all sections of manuscript for publication.
Ashok Kumar Jaryal: This author helped with intellectual content, study design, data collection, writing and editing all sections of manuscript, and approving manuscript for publication.
Sachin Borkar: This author helped with intellectual content, study design and data collection publication.
Gunna Nikhila Reddy: This author helped with intellectual content, study design and data collection publication
Consent to Participate
Informed consent was taken before the start of recording data.
Consent to Publish
Informed consent was taken before the start of recording for scientific publishing of data.
Data Availability
The data underlying this article will be shared on reasonable request to the corresponding author.
Statement of Ethics
Ethical approval from Institute Ethics Committee was taken - (Ref. No.: IECPG-522/23.09.2020, RT-49/21.10.2020). The work described has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
TestMyBrain
It is a resource maintained and aided by The Many Brains Project, Inc. The web-based tasks remain the intellectual property of The Many Brains Project, which retains the copyright for these tasks and the source code. The tests were conducted after receiving license and access to the modules through