
Abstract
Background
Myasthenia gravis is an autoimmune neuromuscular disease primarily caused by autoantibodies against nicotinic acetylcholine receptors (AChRs) at the neuromuscular junction. However, extrathymic malignancies need to be considered in the elderly population.
Purpose
Although thymic malignancy is the most common tumour association, several extrathymic malignancies complicated with myasthenia gravis have been reported. During the review of the literature, there are only a few reports of myasthenia occurring as a paraneoplastic manifestation of renal cell carcinoma.
Methods
We present a 64-year-old elderly gentleman with progressive weakness. The patient underwent routine blood investigations, AChR antibody testing repetitive nerve stimulation test (RNST), contrast-enhanced computed tomography of the abdomen and radical nephrectomy with histopathological analysis.
Results
The patient improved significantly with immune modulatory therapies and underwent surgical intervention. He also later started on adjuvant chemotherapy based on histopathological reports and analysis. This case highlights the need for evaluation of extrathymic malignancy in late-onset myasthenia gravis.
Conclusion
Our case highlights the need for screening for extrathymic malignancies in patients presenting with late-onset myasthenia gravis, which had good outcomes if identified early initiation of treatment.
Keywords
Introduction
Myasthenia gravis (MG), Lambert–Eaton myasthenic syndrome and neuromyotonia are neuromuscular transmission disorders occurring with or without associated malignancy. Tumours of the genitourinary system are a heterogeneous group of malignancies affecting people of all ages. The most common malignancies of the genitourinary system include prostate cancer, renal cell carcinoma (RCC), bladder cancer and testicular cancer. Neurogenic complications are an important cause of morbidity and mortality in the patient population. With the advent of more effective treatments, these patients are living longer with an incidence of central nervous system relapse and treatment-related neurologic sequelae. Paraneoplastic syndrome develops in approximately 10%–40% of patients with RCC. Neuromuscular disorders, such as paraneoplastic syndrome related to RCC, are extremely rare.
Case Presentation
A 64-year-old gentleman with slurring of speech, drooping of eyes and dysphagia for both solids and liquids of 3 days duration was presented. His speech became unintelligible when he spoke for a longer duration, and there was a worsening of his symptoms towards evening.
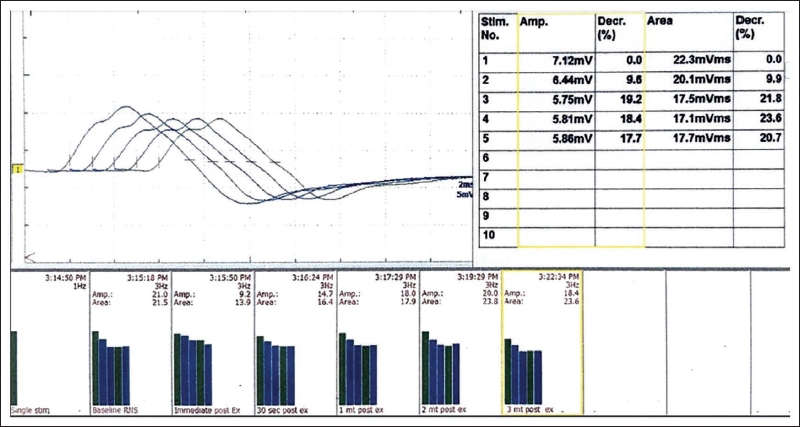
On examination, there was asymmetric drooping of the eyelids with bilateral facial, pharyngeal and tongue muscle weakness. Extraocular movements were normal. The patient had a head drop with weakness of neck flexors more than neck extensors. In lower limbs, there was proximal weakness (medical research council grade 4/5) with upper limb involvement restricted to the mild asymmetric weakness of the triceps. Deep tendon reflexes and sensory system examination were normal. Examination of other systems was unremarkable. Routine haematology and biochemistry, including thyroid profile and serum creatine kinase levels, were normal. His serum acetylcholine receptors (AChR) antibody and anti-muscle specific kinase (MUSK) antibody were negative. Repetitive nerve stimulation study at 3 Hz showed significant decremental response (Figure 1).
Repeated Nerve Stimulation Test is Consistent with Post-synaptic Neuromuscular Junction Disorder.
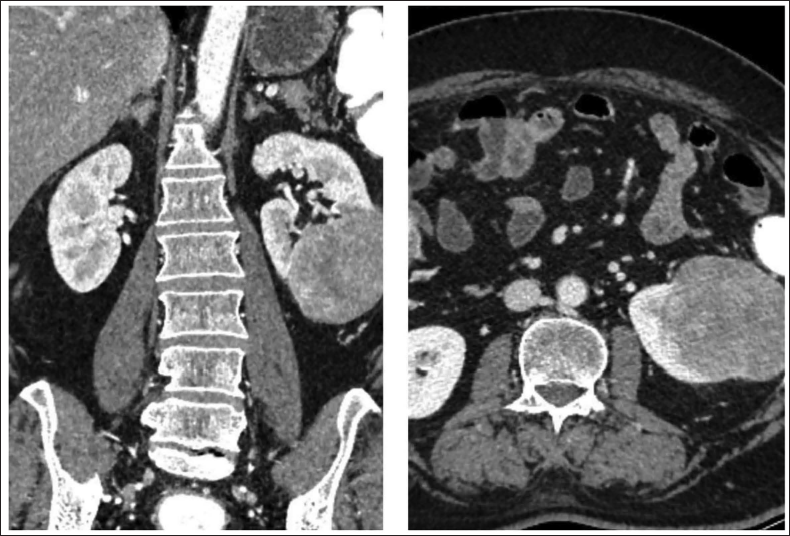
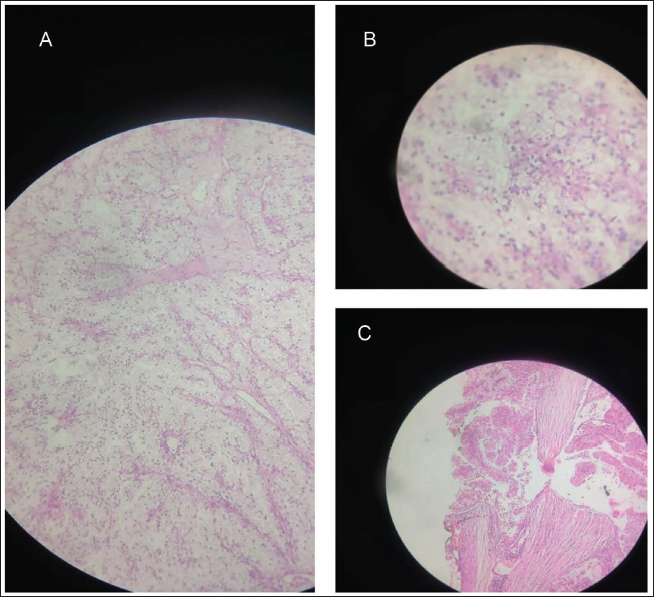
He was diagnosed to have MG myasthenia gravis foundation of America (MGFA) stage 3B. Computed tomography (CT) of the thorax showed no evidence of any thymic abnormalities. However, the lower sections of the CT captured a partially exophytic, soft tissue density lesion arising from the lower pole of the left kidney, showing heterogeneous enhancement suggestive of RCC (Figure 2). He was managed with plasmapheresis, cholinesterase inhibitors and oral steroids followed by azathioprine. A radical nephrectomy was done. The biopsy of lesion was suggestive of clear cell RCC of International society of urological pathology (ISUP) grade 2, unifocal, pathological tumour node metastasis (pTNM) grade pT3aNxMx. Since malignancy was seen infiltrating the capsule and perinephric fat, adjuvant chemotherapy with sunitinib maleate was also started. The patient had significant improvement on treatment; later he was able to taper off the medication and maintain on low-dose steroids.
(A) Clear Neoplastic Cells Separated by Thin Fibrous Septae. (B) Higher Power of Neoplastic Cells Showing Clear Cytoplasmic, Vesicular Nuclei, Nucleoli. (C) Capsule Invasion by Neoplastic Cell.
Discussion
MG is the most common autoimmune neuromuscular junction disorder affecting both the young and elderly. The relationship between autoimmunity and cancer is bidirectional, with cancer increasing the risk of autoimmunity and vice versa. Myasthenia may occur in association with malignancy in about 10–15% of cases, either as a paraneoplastic manifestation or as a complication of treatment, particularly with immune checkpoint inhibitors. 1 The malignancy that is most commonly associated with myasthenia is thymic carcinoma, predictably due to the central role of the thymus in autoimmunity associated with myasthenia. However, other malignancies may occur in association with MG at times, along with thymic malignancy. 2 In a Swedish registry of 2,812 patients with MG, as many as 630 patients (22.4%) had extrathymic malignancy. 3 The most common malignancies observed in this cohort included cancer involving the skin, genital organs, digestive organs and breast. However, register-based data have their own inherent weaknesses, as pointed out by the authors, particularly with regard to the confirmation of myasthenia and the inability to do a multivariate analysis assessing other comorbidities that may have predisposed these patients to malignancy. 3 RCC is less commonly associated with MG. RCC may be manifested with the paraneoplastic syndrome in approximately 10%–40% of patients with RCC, 4 which is mainly divided into endocrine and nonendocrine. Systemic hypertension (40%), non-metastatic hepatic dysfunction and hypercalcaemia are the common manifestations. Neuromuscular disorders, such as MG related to RCC, are rare. 2 In a retrospective study of 283 patients diagnosed with MG, Zheng et al. 5 noted that six patients also had RCC. All these patients were positive for the anti-AChR autoantibody. Of these patients, RCC was diagnosed within 2 years of the diagnosis of myasthenia in four cases. In one of them, RCC was detected accidentally while screening for malignancy at the onset of myasthenia, as in our case. In a population-based retrospective case-control study consisting of 3,671 patients with myasthenia, the most common malignancies were lymphoid malignancies, breast cancer and lung cancer. 6 There are also few reports on patients who were on immune checkpoint inhibitors like pembrolizumab for RCC and who developed seronegative MG while on treatment. 7
The mechanism of neurological paraneoplastic syndromes is primarily immunologic, associated with antibody and T cell-mediated responses to antigens shared between the tumour and neural tissue. The thymus has two sources of AChR determinants, including myoid cells and medullary thymic epithelial cells that produce only unfolded subunits or fragments of AChR. Neurological paraneoplastic syndromes are rare events in RCC. Unlike in the case of thymoma, the pathophysiological basis of the development of myasthenia in extrathymic malignancies is not clearly elucidated. 8 Peripheral neuropathy can also be a neurological manifestation of RCC. 9 Unlike other reports, our patient with RCC had a seronegative MG. This also makes a mechanism similar to thymic malignancy-associated MG less likely in our case.
Conclusion
Extrathymic malignancies are increasingly recognised as related to MG. However, the exact relationship as to whether these are causes or consequences of malignancy and their pathophysiological basis is not clearly delineated. Hence, especially in late-onset MG, neoplastic screening should extend beyond the thymus, which may uncover potentially treatable cancers such as RCC.
Authors’ Contribution
Reji Thomas: Substantial contribution to the concept, design of article.
Vijyalekshmi S: Substantial contribution to the concept and design collecting patient data and writing up.
Jeethu thampi: Collection data, figures and tables, editing.
All authors approved the final version of the article to be published.
Statement of Ethics
The ethical clearance has been obtained from Institutional Ethical Committee.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Ethical Approval
The ethical clearance has been obtained from Institutional Ethical Committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.