
Abstract
Background
The COVID-19 pandemic has led to a range of long-term health issues in recovered patients, collectively known as "post-COVID syndrome."
Purpose
This study aimed to investigate the effects of combined pranayama techniques, specifically Sheetali and Bhramari, on pulmonary function and heart rate variability in post-COVID patients.
Methods
A randomised controlled trial was conducted with 90 post-COVID patients (aged 19-40). Participants were divided into three groups of 30 each: control, Bhramari Pranayama and Sheetali Pranayama. The intervention groups practiced their respective pranayama techniques for 15 minutes twice daily for 6 months. Outcome measures included Pulmonary Function Tests (PFT) and Heart Rate Variability (HRV), assessed at baseline, 3 months and 6 months.
Results
At 3 months, both pranayama groups showed moderate improvements in pulmonary function and HRV compared to baseline. By 6 months, these improvements were significantly enhanced. The Bhramari group showed increased FVC from 3.2 ± 0.5 L to 3.5 ± 0.4 L at 3 months, and to 3.7 ± 0.4 L at 6 months (P < .001). Similarly, the Sheetali group reflected improved FVC from 3.3 ± 0.4 L to 3.5 ± 0.3 L at 3 months, reaching 3.7 ± 0.3 L at 6 months (P < .001). HRV measures showed a similar trend, with SDNN and RMSSD in the Bhramari group and Sheetali pranayama group.
Conclusion
This study provides novel insights into the combined effects of Bhramari and Sheetali Pranayama on post-COVID patients. The findings suggest significant improvements in respiratory function and autonomic nervous system balance.
Introduction
The COVID-19 outbreak became a serious global health disaster, affecting millions of people worldwide. 1 The fallout of COVID-19 introduced a fresh set of issues, even though the first phase of the disease was severe and had caused breathing difficulties and other complications. 2 Many individuals who recovered from the initial illness continued to have symptoms known as "long COVID" or "post-COVID syndrome," which affected many of them. 3 There were various symptoms of this disease, such as weariness, memory loss, muscular and joint pain and emotional suffering. Post-COVID syndrome is a significant condition characterised by a complex interplay of immune, endocrine and neurological system interactions. 4 The persistent stress response in these people was generally reflected in the high levels of stress biomarkers, including oxidative stress markers, inflammatory cytokines and cortisol. 5 Insights into the underlying processes of stress and the efficacy of different therapies were possible by comprehending the regulation of these biomarkers and gene expressions. One of the yogic practices is pranayama, which is a regulated or synchronised breathing that has drawn attention towards good health, especially for respiratory issues and stress reduction. 6 Through a series of yogic practices, pranayama controls the body’s prana, or life energy, to enhance the body’s own healing. 7 Among these, Bhramari and Sheetali are unique breathing techniques that help cool the body, calm the mind and reduce stress. 8 Bhramari Pranayama has the feature of imitating the buzzing sound created by a bee during exhalation. This method has well-known mind-and-body-calming effects. Through the activation of the parasympathetic nervous system, the stress response is reduced, and relaxation is improved. 9 Previous studies indicated Bhramari Pranayama may reduce blood pressure, heart rate and anxiety levels, thereby helping to manage physiological stress. To generate a cooling feeling, practice Sheetali Pranayama by breathing through your mouth with your tongue curled. This technique is used for relaxing the mind and body by lowering body temperature, reducing tension and promoting calmness. 10 The cooling effect of Sheetali Pranayama is believed to lessen inflammation and oxidative stress, which are common in post-COVID conditions. Examined in the framework of post-COVID recovery, Bhramari and Sheetali Pranayama combined conventional methods with scientific analysis. 11 The purpose of this study was to investigate the effects of Bhramari and Sheetali Pranayama techniques on pulmonary function test and heart rate variability in post-COVID patients.
Methods
Study Design and Setting
This is a randomised controlled trial (RCT) study designed to examine the combined effects of Bhramari and Sheetali Pranayama in post-COVID-19 patients. This study included 90 post-COVID-19 patients, both male and female, aged 19 to 40. Participants had been diagnosed with and recovered from COVID-19, provided informed consent and completed a study questionnaire. Exclusion criteria were patients with Cardiovascular disorders, Renal and hepatic failures, Dyspnea, Neuropathy, recent surgeries and also healthy individuals without a COVID-19 history.
Intervention
Group A served as the control group and did not engage in any specific intervention. Group B practiced Bhramari Pranayama, a breathing technique characterised by slow, deep breathing with a humming sound made during exhalation, which is believed to promote relaxation, reduce stress and enhance vagal tone. 13 During each Bhramari session, participants sat comfortably, closed their eyes and focused on deep breaths, inhaling through the nose and exhaling while producing a soft humming sound, typically with eyes closed and ears partially covered with fingers to amplify the internal vibrations and enhance concentration.11, 14 Group C practiced Sheetali Pranayama, a cooling breath technique thought to reduce body temperature, calm the mind and lower blood pressure. 15 In Sheetali, participants curled their tongues to form a "straw," inhaled through the rolled tongue and then closed their mouths, holding their breath briefly before exhaling slowly through the nose. 12 Both pranayama practices were performed daily for 30-minute sessions under the guidance of certified yoga trainers to ensure consistency, correct technique and participant safety. Each session included a few minutes of preparatory breathing to relax the participants, followed by 20–25 minutes of focused pranayama practice and a brief period of relaxation or meditation to conclude (see suppl file.1).
Outcome Measures
Pulmonary Function Tests (PFTs) were conducted to assess respiratory function using a spirometer, specifically the RMS Helios 407, a widely used and reliable device for respiratory measurements. Standardisation of the instrument was ensured by calibrating the spirometer according to the manufacturer’s guidelines before each session, ensuring accurate and consistent readings. PFT measures included Forced Vital Capacity (FVC), Forced Expiratory Volume in one second (FEV1) and Peak Expiratory Flow Rate (PEFR), all of which provide valuable insights into lung capacity, airway function and respiratory muscle strength. The PFTs were administered by a trained and experienced pulmonology technician with 10 years of experience in conducting respiratory assessments, ensuring adherence to testing protocols and participant comfort throughout the procedure.
Heart Rate Variability (HRV) was assessed by recording a five-minute ECG of participants in a supine position, using a portable ECG device connected to a simple Analog-to-Digital (AD) converter.16,17 The time of day for each HRV recording was standardised, typically conducted in the morning to minimise the effects of circadian variations on HRV values, which are known to fluctuate based on physiological rhythms. During data collection, the AD converter sampled the analogue ECG signal at a high frequency (8000 Hz), ensuring that even small variations in the heart rate could be accurately captured by detecting R-wave peaks in the waveform. This digitised signal was processed to determine NN (Normal-to-Normal) intervals, representing the time between successive heartbeats. Using these NN intervals, specific time-domain measures such as SDNN (Standard Deviation of NN intervals) and RMSSD (Root Mean Square of Successive Differences) were calculated to assess autonomic nervous system function by the Kubios HRV software.
Ethical Considerations
The study was approved by the Institutional Ethics Committee (Ref: SRM MCH & RI: 2931/IEC/2021). All participants gave their informed consent, with consent forms available in both in English and the local language.
Statistical Analysis
Statistical analysis was performed using SPSS version 20. Descriptive statistics were calculated for all variables. Comparisons between groups were made using analysis of variance (ANOVA) for normally distributed data and Kruskal-Wallis test for non-normally distributed data. Paired t-tests or Wilcoxon signed-rank tests were used to compare pre- and post-intervention results within the groups. A P value < .05 was considered statistically significant.
Results
Baseline Characteristics
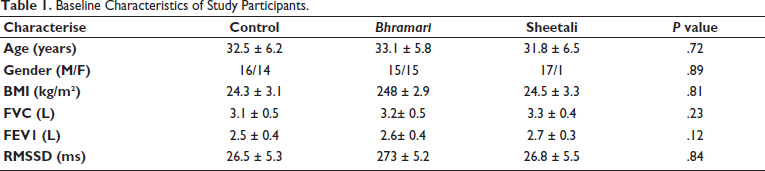
A total of 90 participants were initially enrolled in the study. Baseline characteristics were similar across all three groups, with no statistically significant differences (Table 1).
Baseline Characteristics of Study Participants.
Drop-Out Details
During the study period, three participants dropped out: one from the control group due to relocation and two from the Bhramari group (one due to personal reasons and one lost to follow-up). The final analysis included 29 participants in the control group, 28 in the Bhramari group and 30 in the Sheetali group.
Group-Wise Comparison of Outcomes
Pulmonary Function Tests
Both pranayama groups showed significant improvements in pulmonary function compared to the control group (Figure 1).
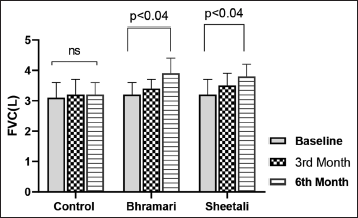
Changes in the FVC After Intervention Between the Groups.
The Bhramari group showed the largest improvement in FVC (mean difference 0.5 L, P < .04), followed closely by the Sheetali group (mean difference 0.4 L, P < .04). Both intervention groups demonstrated similar improvements (Figure 2) in FEV1 (mean difference 0.3 L, P < .01 for both) and PEFR (Figure 3, mean difference 1.3 L/sec, P < .05 for both).
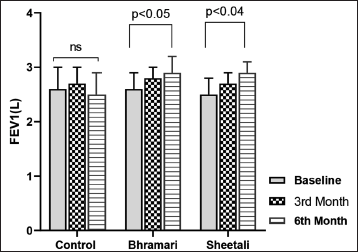
Changes in the FEV1 After Intervention Between the Groups.
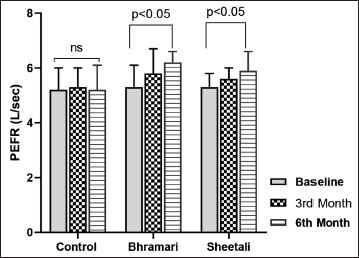
Changes in the PEFR After Intervention Between the Groups.
Heart Rate Variability
HRV measures, particularly SDNN and RMSSD, showed significant improvements in both pranayama groups compared to the control group (Figures 4 and 5).
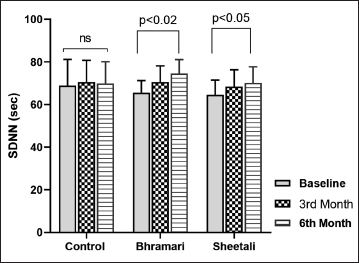
Changes in the SDNN After Intervention Between the Groups.
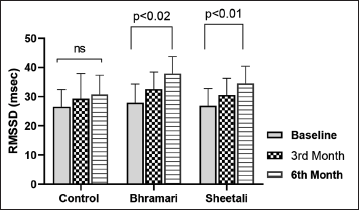
Changes in the RMSSD After Intervention Between the Groups.
The Bhramari group showed the largest (table Figure 3) increase in RMSSD (mean difference 5.5 ms, P < .01), indicating enhanced parasympathetic activity. The Sheetali group also demonstrated significant improvement (mean difference 4.8 ms, P < .02).
Between-Group Comparisons
One-way ANOVA with post-hoc Tukey’s test revealed that both Bhramari and Sheetali groups had significantly greater improvements in FVC, FEV1 and RMSSD compared to the control group (all P < .01). The differences between Bhramari and Sheetali groups were not statistically significant for any outcome measure (all P > .05).
Discussion
This study was the first ever to examine the combined effects of Bhramari and Sheetali Pranayama in post-COVID patients. Previous studies have shown that pranayama can significantly enhance respiratory function 18 and reduce stress, 13 but no studies had examined its effects specifically on post-COVID patients.
A quasi-randomised clinical trial provides preliminary evidence that a 28-day Pranayama intervention may significantly reduce the risk of COVID-19 infection among frontline Health Care Professionals (HCPs). They observed 89% reduction in infection risk in the intervention group, which suggests that Pranayama could be a potentially effective, low-cost and easily implementable strategy for enhancing protection against COVID-19 in high-risk populations. 19 The 15-day Bhramari Pranayama intervention demonstrated significant efficacy in reducing psychological distress and improving sleep quality among asymptomatic COVID-19 patients in home isolation. These findings suggest that Bhramari Pranayama could be a valuable, non-invasive complementary therapy to support mental health during infectious disease outbreaks. 11
The potential role of Nitric Oxide (NO) in managing COVID-19 is supported by its demonstrated effectiveness during the 2004 SARS-CoV pandemic, where it improved pulmonary hypertension, severe hypoxia and patient outcomes. Bhramari Pranayama, a yogic breathing technique involving humming, has been shown to increase endogenous NO production by up to 15-fold, suggesting it could be a non-invasive method to boost NO levels in COVID-19 patients. Additionally, the extended exhalation in Bhramari may induce a mild hypoxic hypercapnic state with alkaline pH, potentially preventing coagulopathies associated with COVID-19 and reducing morbidity, though further clinical studies are needed to confirm these hypothesised benefits. 20
Another study demonstrates the potential benefits of Yogic breathing techniques for COVID-19 patients, recovered individuals and healthcare workers. Notably, D-dimer levels, a key marker of thrombosis risk, remained below the severity cutoff of 0.50 µg/mL in the COVID-positive yoga group and significantly decreased in the COVID-recovered (P = .002) and healthcare worker (P = .01) yoga groups. Exercise capacity improved, with significant increases in the 6-minute walk test distance for COVID-positive patients (P = .01) and healthcare workers (P = .002). 21
Systematic review reported that Bhramari Pranayama enhances relaxation through the activation of the parasympathetic nervous system via humming breath sounds, 22 while Sheetali Pranayama increases the cooling effect on the body, which reduces inflammation and reactive oxygen species production9, 23, 24. Additionally, a study on Sheetali Pranayama practiced for hypertension (HTN) showed significant reductions in blood pressure and improved HRV parameters, indicative of parasympathetic dominance. 15
Our findings align with and extend upon these previous studies. The significant improvements in pulmonary function tests (PFT) and heart rate variability (HRV) observed in both the Bhramari and Sheetali Pranayama groups suggest that these techniques may be particularly beneficial for post-COVID patients. The increase in forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) indicates improved lung function, which is crucial for patients recovering from COVID-19-related respiratory issues.
The improvements in HRV measures, particularly the increase in RMSSD, suggest enhanced parasympathetic activity. This is consistent with the stress-reducing effects of pranayama reported in previous studies and may be particularly beneficial for post-COVID patients who often experience prolonged stress and anxiety.
The combined use of Bhramari and Sheetali Pranayama in our study appears to offer complementary benefits. While Bhramari may increase nitric oxide production and induce relaxation, Sheetali induced cooling effect may help reduce inflammation. This synergistic effect could explain the substantial improvements observed in both respiratory function and autonomic balance.
However, our study has limitations. The sample size was relatively small, and the study was conducted at a single centre. Future multi-centre trials with larger sample sizes are needed to confirm these findings. Additionally, long-term follow-up studies would be valuable to assess the durability of the observed benefits.
Conclusion
This study provides evidence that a combined Bhramari and Sheetali Pranayama intervention can significantly improve pulmonary function and heart rate variability in post-COVID patients. These findings suggest that these pranayama techniques could be a valuable, non-pharmacological approach to support recovery in post-COVID syndrome. The improvements in both physiological measures and subjective well-being indicate a holistic benefit of this intervention.
Footnotes
Acknowledgements
We would like to thank the participants for their time and cooperation in this study. We also express our gratitude to Host institution for providing the facilities to conduct this research.
Authors’ Contribution
R.P.: Conceptualisation, Methodology, Investigation, Data curation, Writing - original draft.
A.S.: Supervision, Validation, Writing - review & editing.
K.M.: Formal analysis, Data curation, Visualisation, Writing - review & editing.
K.T.S.: Investigation, Resources, Project administration.
P.K.P.: Methodology, Investigation, Data collection.
V.P.: Conceptualisation, Supervision, Writing - review & editing.
All authors have read and agreed to the published version of the manuscript.
Statement of Ethics
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of the host institution (Ref: SRM MCH & RI: 2931/IEC/2021).
Declaration of Conflicting Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
ICMJE Statement
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Informed Consent
All participants gave their informed consent, with consent forms available in both in English and the local language.