
Abstract
Background
Taylor and Palmer introduced an angiosome (vascular) concept in reconstructive plastic surgery in 1987. The angiosome is considered a segment of a nerve (cranial or peripheral nerve) supplied by a primary source of blood vessels.
Purpose
To observe the arteries supplying the vestibulocochlear nerves (VIII) from the brainstem till their termination. To analyse the neurovascular relationship of the vestibulocochlear nerve.
Methods
In total, 45 formalin-fixed cadaveric heads with the base of the skull were studied by dissection and histological methods.
Results
At the level of the pontomedullary junction, it is supplied by the anterior inferior cerebellar artery; within the internal acoustic canal, the cochlear nerve is provided by the cochlear artery, the vestibular nerve is supplied by a vestibular artery, which is the fine branch of the labyrinthine artery.
Conclusion
Their vascular supply influences the functioning of nerves. The labyrinthine artery is a thin, slender end artery, making it more vulnerable to circulatory disturbances.
Introduction
An angiosome (vascular) is a segment of a cranial nerve supplied by a specific artery. In 1987, Taylor and Palmer introduced the angiosome concept, revolutionising the understanding of vascular anatomy. They identified 13 angiosome territories in the head and neck region. Three angiosome territories are located within the skull base but not in contact with the neck. 1
A thorough understanding of cranial nerves and their arterial supply is crucial for neurosurgeons and neurophysicians. This knowledge is essential for surgeons, as it ensures that grafts have a sufficient section of nerve with proper arterial supply, thereby optimising surgical outcomes. 2 The vestibulocochlear nerve is functionally and anatomically divided into two parts: the vestibular nerve, responsible for maintaining equilibrium and balance, and the cochlear nerve, responsible for hearing. This nerve belongs to the particular somatic afferent column. 3
The arterial supply of specific cranial nerves, including the vestibulocochlear nerve, has specialised features that hold significant clinical importance. The vascularisation of the auditory nerve, particularly its cochlear division, has been extensively studied. 4 Lesions of the cochlear nerve and temporal lobe can result in hearing loss, while injuries to the vestibular nerve can cause giddiness (vertigo) and nystagmus. 5
Understanding the vascularisation of the vestibulocochlear nerve complex is crucial for grasping vascular ischemic syndromes. 6 Notably, the labyrinthine artery is a thin, slender artery with no collateral circulation. 7 During facial development, the thickening of specialised ectoderm forms ectodermal placodes, which appear during the third week of gestation. The vestibular and cochlear apparatus develops from otic placodes, and neural crest cells from the rhombencephalon invaginate the ganglion of vestibular and cochlear components of the vestibulocochlear nerve. 8 Vestibular neuritis or neuritis (VN) is a clinical syndrome characterised by spontaneous, prolonged vertigo resulting from sudden unilateral disruption of the peripheral vestibular system. The clinical syndrome is called labyrinthitis when hearing loss is also present. 9
Given the significance of the vestibulocochlear nerve and its vascular supply, this study aims to describe the arterial supply of the vestibulocochlear nerves from origin to their termination, highlighting the critical blood vessels involved and their relationships with the nerve fibres and to study the microscopic structure of the vestibulocochlear nerves along with its blood supply.
Methods
This study utilised 45 formalin-fixed human heads obtained from the Department of Anatomy, Mamata Medical College, Khammam. In total, 45 embalmed cadaveric specimens, along with the base of the skull, were dissected for the study of the arterial supply of the vestibulocochlear nerve. A histological study was also conducted on segments of nerves along with blood vessels.
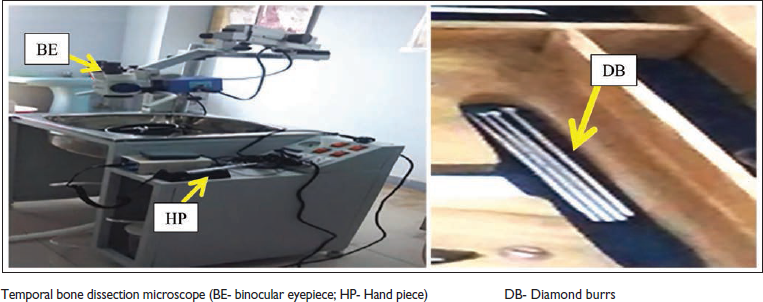
Temporal Bone Dissection and Examination
The brain was carefully removed, leaving the brain stem intact while preserving the vestibulocochlear nerve and labyrinthine artery. Subsequently, bilateral temporal bones were removed from five cadavers. The temporal bone specimens were examined under an ENT operating microscope with 4×–6× magnification in the ENT department. Drilling of the petrous part of the temporal bone was performed using diamond burrs of varying sizes (4-3-2-1 mm). Digital photographs were taken to document the process.
Nerve Sample Collection Sites
Nerve samples were collected for histological examination from three specific locations. A 1-cm nerve sample, including accompanying vessels, was taken from each site. The first location was at the level of the pontomedullary junction. The second location was at the level of the bony cochlea, where the spiral ganglion is situated. The third location was the fundus of the internal acoustic meatus, where the vestibular ganglion is located.
Results and Observations
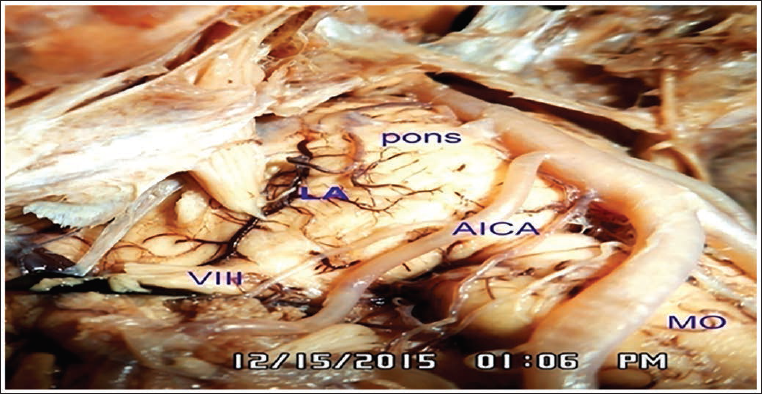
The vestibulocochlear nerve can be divided into two segments for descriptive purposes. The cisternal segment along with the facial nerve emerges from the pontomedullary junction and extends to the entry of the internal acoustic meatus. In contrast, the intrapetrous segment runs from the fundus of the internal acoustic meatus to its termination in the petrous part of the temporal bone. Notably, our study found that the (Table 1) cisternal segment of the vestibulocochlear nerve, along with the facial nerve, was supplied by the anterior inferior cerebellar artery (AICA) in 76 specimens, with 38 specimens on the right side and 38 specimens on the left side (Figure 1).
Arterial Supply of Vestibulo Cochlear Nerve.

Blood Supply of the Intrapetrous Segment of the Vestibulocochlear Nerve
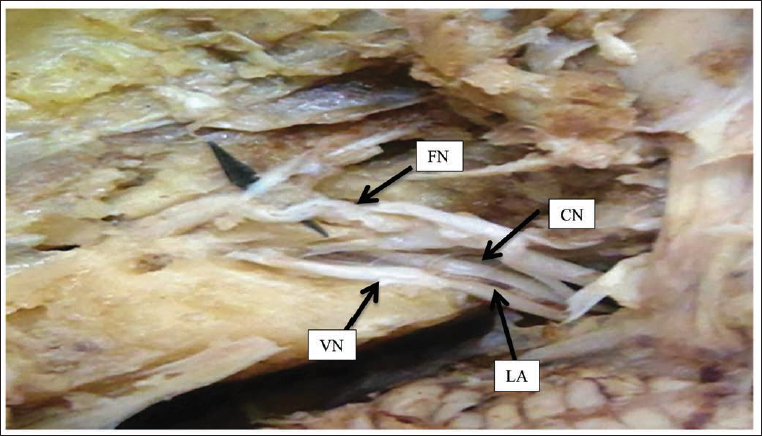
To investigate the blood supply of the VIII cranial nerve within the petrous part of the temporal bone, we dissected 10 temporal bones using an ENT operating microscope. Our dissection revealed that the arterial supply to the intrapetrous segment of the VIII nerve was only traceable in one out of the 10 specimens, and it originated from the labyrinthine artery, which in turn arose from the basilar artery (Figures 2 and 3).

Histological Observations of the Vestibulocochlear Nerve
Thin sections (5µ) of various segments of the vestibulocochlear nerve, including the cisternal and intrapetrous segments and the vestibular and spiral ganglions, were stained with hematoxylin and eosin.
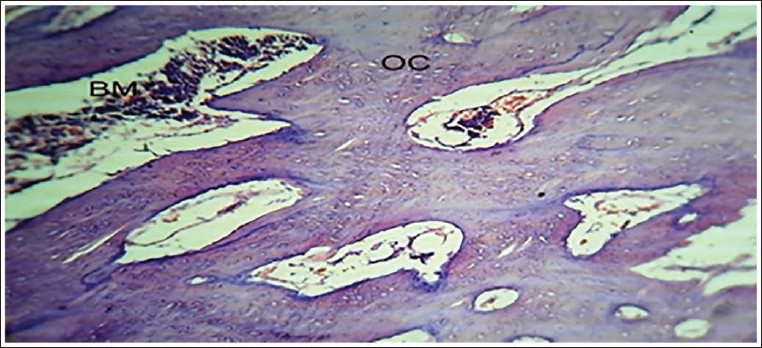
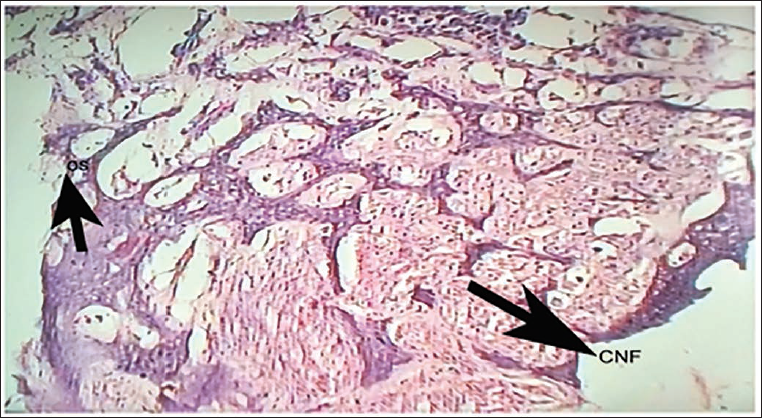
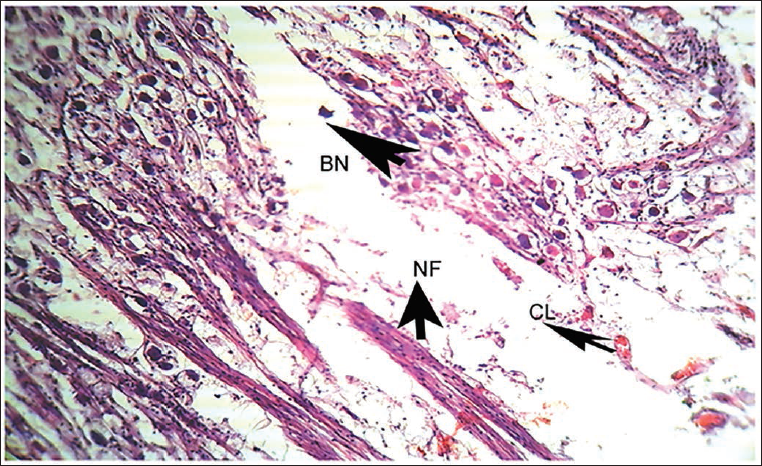
In addition, sections of nerves were taken along with blood vessels. All sections were studied under a light microscope at 10× and 40× magnification. Our observations revealed that the diameter of the lumen of vessels increased towards the periphery compared to the centre at all levels. The vestibular ganglion showed bipolar neurons, neuronal processes and capillaries. The LS of the cisternal segment of the vestibular nerve exhibited ganglionic cells and nerve fibres in bundles, with ganglionic cells discretely distributed among nerve fibres and a moderate number of capillaries (Figure 4). The spiral ganglion displayed cell bodies of bipolar neurons with nuclei and satellite cells surrounding the bipolar neurons, accompanied by tiny capillaries (Figure 5). Finally, the bony cochlea showed the osseous spiral lamina and bone, although a complete section of the bony cochlea could not be obtained to examine the stria vascularis (Figures 6 and 7).
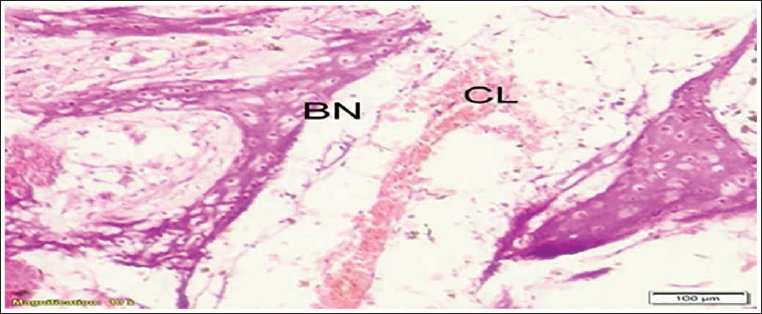
Bipolar Neurons (BN), Nerve Fibres (NF) and Capillary (CL) in Spiral Ganglion.
Statistical Data
There is a significant association between the arterial supply of two segments of vestibulocochlear (VIII) nerve segments (Table 2).
The Association Between the Arterial Supply of Different Segments of Vestibulocochlear (VIII) Nerve in Human.

Discussion
The labyrinthine artery and its differentiation from the subarcuate artery are crucial when performing various skull base approaches that involve exposure to the cerebellopontine angle. A thorough anatomical knowledge is critical for preventing inadvertent damage in this region, which can be approached from the middle cranial fossa, trans labyrinthine, retro labyrinthine or retro sigmoid. 9 This is particularly important because the inner ear is supplied by only one end artery, the labyrinthine artery derived from the AICA. 10 Schwalbe 8 was the first to systematically describe the circulation of the human cochlea, followed by Eichler 9 , Siebenmann and Nabeya 10 , who used intravascular dye injections.
The anatomy of the AICA is often variable, which can further complicate the surgical approach. The AICA originates from the basilar artery, typically arising from the junction between the middle and lower thirds of the basilar artery. 10 However, it can also occur from the lower one-third of the basilar artery in approximately 52% of cases, the middle third in approximately 46%, and the upper one-third in approximately 2% of cases. 9 This variability highlights the need for a thorough understanding of the anatomy of the AICA and its relationship to the labyrinthine artery.
In our study, 45 temporal bones were dissected, and only one fresh temporal bone traced the labyrinthine and vestibulocochlear arteries by microdissection technique. Our observations revealed that the spiral ganglion consists of cell bodies of bipolar neurons, prominent nucleoli, surrounded by a layer of satellite cells and tiny capillaries (Figure 7). Furthermore, we found that the labyrinthine artery runs between the cochlear and vestibular nerves in the internal auditory canal, which is consistent with previous studies. 9 However, we could not trace the subarcuate artery, an inconstant artery that ends in the dura mater around the subarcuate fossa in 35% of cases. 9
Our findings also align with previous studies that have shown the origin of the labyrinthine artery to be inferomedial to the vestibulocochlear nerve in most cases (71.4%). In contrast, the subarcuate artery was usually lateral (70%). 9 Our study provides further evidence for understanding the anatomy of the labyrinthine and subarcuate arteries in the internal auditory canal.
Conclusion
Our study underscores the critical role of vascular supply in maintaining the proper functioning of peripheral nerves. Specifically, the labyrinthine, a delicate and slender end artery, plays a vital role. Our findings confirm that the labyrinthine artery is typically situated inferomedially to the vestibulocochlear nerve at both its distal and proximal aspects. In contrast, the subarcuate artery is located laterally at its distal aspect. Notably, the labyrinthine artery’s vulnerability to circulatory constriction is a concern, as it lacks collateral circulation, making it more susceptible to damage. The petrous part of the temporal bone provides a protective environment for the delicate structures it houses, including the cochlea, vestibular nerves and organ of Corti. Furthermore, our study highlights the importance of using fresh specimens for tracing the labyrinthine artery, as this approach allows for more accurate and detailed observations.
Footnotes
Acknowledgement
I express special thanks to Dr S. S. Saradadevi, Dr Suseelamma D, and Dr Subhadradevi V for their wholehearted co-operation and encouragement in the completion of this research work My sincere thanks to Dr Muniruddin Prof and HOD of ENT for having led me with confidence during the dissection of vestibulo cochlear nerve arterial supply.
Authors’ Contribution
Myself Dr S. Deepthi, the manuscript is a part of my PhD project work. I have done this work with the collaboration of the ENT department because this study is relevant to the inner ear. Dr K. C. Haritha has helped me in writing the manuscript, given suggestions to practical approach while carrying out the work. She is research-oriented. Dr M. Upendra, my junior colleague, has helped in the dissection part and taking photographs while doing the dissection. In every step, he used to help in the histological part.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
Not applicable.