
Abstract
Background
The global prevalence of diabetes mellitus has been increasing, leading to a rise in morbidity associated with the disease. While diabetic nephropathy, retinopathy and neuropathy are routinely screened in diabetic patients, the cognitive decline associated with diabetes is often overlooked.
Purpose
The purpose of this study is to investigate the prevalence of cognitive impairment and its associated risk factors among patients with type 2 diabetes mellitus (T2DM).
Methods
An observational cross-sectional study was conducted for two months. The Montreal Cognitive Assessment (MoCA) test, which consists of 30 questions, was used to assess cognitive function. In-depth clinical history along with glycaemic parameters were collected. The chi-square test was used to find out the association between categorical variables and cognitive impairment. Pearson’s correlation test was performed to determine the correlation between glycaemic parameters and cognitive impairment.
Results
A total of 96 patients participated in the study. The mean HbA1c (%) was 9.08 ± 1.73, and the mean MoCA score was 25.14 ± 1.63. Mild cognitive impairment (MCI) was noted in 56% patients. Attention was the most common cognitive domain defect found in all MCI patients—100%. Delayed recall and memory were the second most common cognitive domain defect found—92.5%. Higher HbA1c, high FBS and higher PPBS were found to be statistically associated with MCI. A negative correlation was found between glycaemic parameters (HbA1c, FBS and PPBS levels) and MoCA scores.
Conclusion
More than half of our study participants reported mild cognitive impairment. It highlights the need for the implementation of routine cognitive testing for diabetes patients. There is a strong negative correlation between MoCA scores and parameters of glycaemic control; higher levels of HbA1c, FBS, and PPBS are seen in people with a lower MoCA score, indicating mild cognitive impairment. Further studies are needed to evaluate whether improving glucose levels helps in improving cognition or not.
Keywords
Introduction
Diabetes mellitus is a chronic metabolic disease with multiple aetiologies that disrupt the metabolism of carbohydrates, fats and proteins, resulting in hyperglycaemia. Type 2 diabetes is characterised by high blood sugar levels, which result from either the pancreas producing insufficient insulin or the body’s inability to properly utilise insulin. 1 The global prevalence of diabetes mellitus has been increasing, leading to a rise in morbidity associated with the disease. While diabetic nephropathy, retinopathy and neuropathy are routinely screened in diabetic patients, the cognitive decline associated with diabetes is often overlooked. 2 Cognitive impairment can lead to neurocognitive disorders, which can further exacerbate the impact of diabetes on the health of affected individuals. Given the increasing prevalence of diabetes, the prevalence of cognitive impairment among diabetic patients is likely to increase as well. Therefore, routine screening for cognitive decline should be considered as part of diabetes management. 3
A few studies have reported a link between diabetes mellitus and cognitive decline in the Indian population.4, 5 Moreover, to the best of the authors’ knowledge, very limited research studies have been conducted in our state or region to evaluate the association between cognitive impairment and type 2 diabetes mellitus (T2DM). Understanding the prevalence and risk factors associated with cognitive impairment among T2DM patients in our region could help inform the development of targeted interventions to prevent and manage cognitive decline in this population.
The present study aims to investigate the prevalence of cognitive impairment and its associated risk factors in patients diagnosed with T2DM. We also evaluated the correlation between HbA1c levels, a widely used marker of long-term blood glucose control, and cognitive impairment among T2DM patients.
Methods
Sampling Method and Sample Size
According to a research study conducted in Kerala, India, the prevalence of cognitive impairment in patients with diabetes was reported to be 54.29%. 5 The sample size (n) is calculated according to the formula: n = z 2 × p × (1 − p)/e 2 . So, finally, a sample size of n = 96 was obtained.
Study Tool
In order to screen the participants for cognitive impairment, the Telugu version of the Montreal Cognitive Assessment (MoCA) tool was used.6, 7 ‘This test consists of 30 questions and is designed to evaluate various cognitive domains, including orientation, short-term memory, executive function, language abilities, abstraction, animal naming, attention, and clock-drawing ability.’ ‘The scores on the MoCA range from 0 to 30, with a score of 26 or higher generally considered to be within the normal range. A total score below 26 is indicative of cognitive dysfunction.’
Data Collection and Other Related Details
The questionnaire was asked in Telugu, which is the local mother tongue. Initially, socio-demographic and background information (age, gender, state, educational status and occupation) was collected, followed by a study tool. In-depth clinical history along with body mass index (BMI) and glycaemic parameters (HbA1c levels, duration of diabetes, fasting and postprandial blood sugar levels) were also collected.
Statistical Analysis
Data analysis was conducted using Microsoft Excel 2019 and the Statistical Package for Social Sciences (SPSS) version 24.0. Descriptive statistics, including mean and standard deviation, were utilised to present continuous variables, while categorical variables were presented using percentages. Tables, graphs and charts were included as necessary to effectively illustrate the study findings. The chi-square test was used to find out the association between categorical variables and cognitive impairment. Pearson’s correlation test was performed to determine the correlation between glycaemic parameters and cognitive impairment.
Ethical Considerations
The present study was approved by the Institutional Ethical Committee (IEC) of Rangaraya Medical College, Kakinada, India (Reference No.: IEC/RMC/2022/759). Informed consent was taken from all study participants after explaining the purpose of the research study.
Results
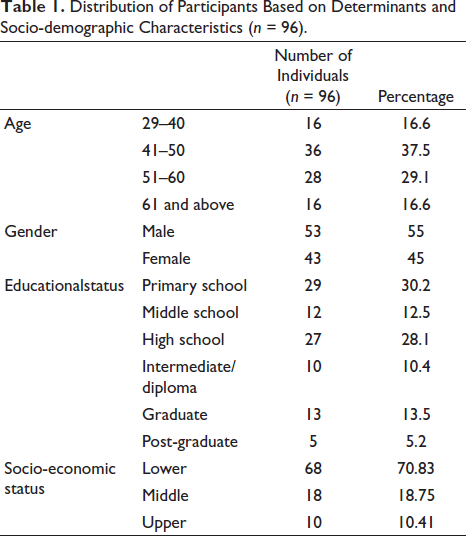
Ninety-six diabetic patients were enrolled in the study. The mean age of the study participants was 50.57 ± 10.067 years. A majority (37.5%) of the study participants were in the age group of 41–50 years. Of the total study population, 55% (53) were male and 45% (43) were female. A significant proportion of participants had completed primary (30.2%) or high (28.1%) school, while a majority of participants belonged to the lower income group (70.8%) (Table 1). Regarding marital status, a majority of participants (87.5%) were married, with a small proportion being widowed (7.3%) or divorced/separated (5.2%). A majority of participants were non-smokers (83%) and non-alcoholics (82%). More than half of the participants (59%, 57) were physically active. In terms of BMI, 37.5% (36) of the study participants were classified as obese, while 23% (22) were classified as overweight.
Distribution of Participants Based on Determinants and Socio-demographic Characteristics (n = 96).
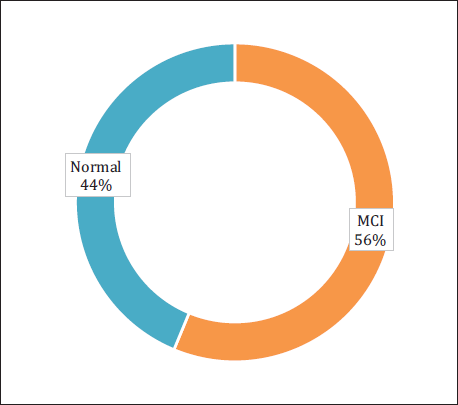
The average duration of diabetes among the study participants was 5.48 ± 4.7 years. The mean HbA1c (%) was 9.08 ± 1.73%. The mean fasting blood sugar (FBS) was 156.25 ± 16.96 mg/dL. The mean post-prandial blood sugar (PPBS) was 251.08 ± 25.31 mg/dL. Fifty-four study participants (56%) had mild cognitive impairment (MCI), and 42 study participants (44%) had normal cognitive function (Figure 1). A majority of patients with MCI had a score of 24, followed by 25 and 23. A majority of patients with normal cognitive function had a score of 26, followed by 27. The mean total MoCA score was 25.14 ± 1.63. A majority of people with MCI belonged to the age group 51–60 (22 out of 54, 40.7%). No significant difference in MCI was observed between males and females.
Status of Cognitive Impairment Among Study Participants (n = 96).
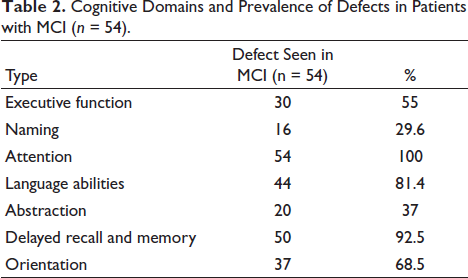
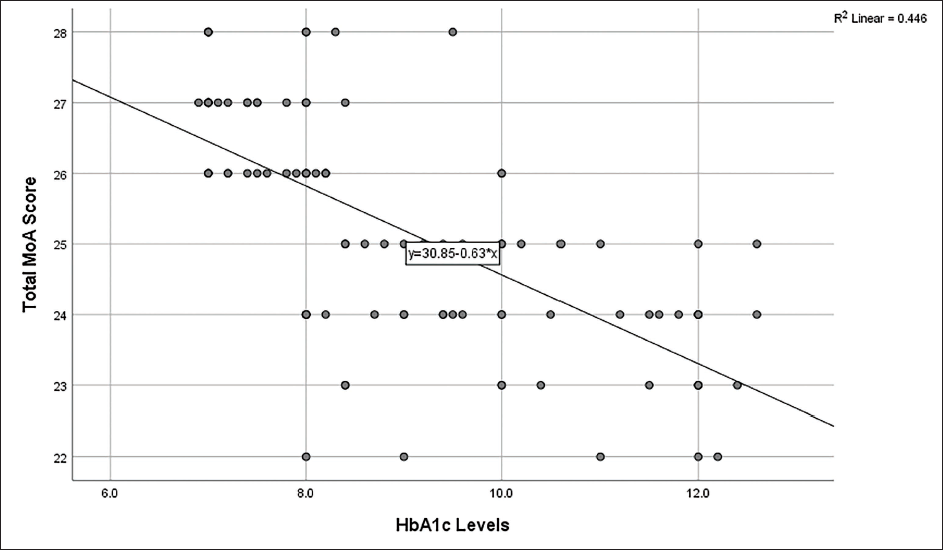
The cognitive domains and prevalence of defects in patients with MCI are presented in (Table 2). Attention was the most common cognitive domain defect found in all patients with MCI, that is, 100%. Delayed recall and memory were the second most common cognitive domain defects found in 92.5% of patients with MCI. Also, 81.4% of patients with MCI had a defect in their language abilities in the cognitive domain. Higher HbA1c, higher FBS and higher PPBS were found to be statistically associated with MCI (Table 3). A negative correlation was found between HbA1c, FBS and PPBS levels and MoCA scores (Table 4). Pearson correlation tests and scatter plots reported a negative correlation between HbA1c levels and MoCA score (Figure 2).
Cognitive Domains and Prevalence of Defects in Patients with MCI (n = 54).
Comparison of Mean Values and p Values Between the MCI and NC Groups.

Correlations Between Glycaemic Parameters and MoCA Scores.
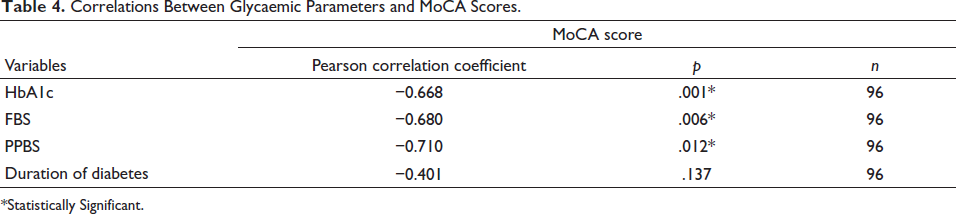
*Statistically Significant.
Scatter Plot Showing a Negative Correlation Between HbA1c Levels and MoCA Score (Pearson Correlation Coefficient Is −0.668).
Discussion
Cognitive impairment is a term used to describe a decline in cognitive abilities. This can manifest in different ways, including forgetfulness and problems with attention and executive function. 8 The American Diabetes Association (ADA) reported that individuals with diabetes are at a greater risk for cognitive problems, such as dementia, Alzheimer’s disease and vascular dementia. 9 Specifically, adults with T2DM exhibit greater impairments in executive function, processing speed and verbal memory. 10 Xue et al. reported that individuals with diabetes had an increased risk of cognitive decline, particularly in the areas of executive function and memory. 11 These findings underscore the importance of regular cognitive screening and early intervention for individuals with diabetes.
This study aimed to assess the prevalence and risk factors associated with cognitive impairment among patients with T2DM. The study included 96 participants, and the findings revealed that 56% of participants had MCI. Age was found to have a significant impact on the MoCA scores, with older individuals exhibiting higher levels of cognitive impairment. Moreover, the results demonstrated a strong negative correlation between HbA1c, FBS and PPBS levels and MoCA scores. Higher HbA1c, FBS and PPBS levels were significantly associated with MCI (p < .05). It is worth noting that previous studies on the relationship between T2DM and cognitive impairment in India have used different questionnaires or study tools to report their findings.
Lalithambika et al. also conducted a similar study in Kerala with 72 participants using the same cognitive assessment tool as our study, the MoCA test. 5 In their study, they found that 54.29% of participants reported MCI, which is similar to our finding of 56% of participants with MCI. Both studies found that patients with MCI had higher HbA1c, FBS and PPBS levels compared to patients with normal cognition and identified attention, delayed recall and memory and language abilities as the cognitive domains that were affected. Another study conducted in Punjab by Khullar et al. included a larger sample of 516 participants and used the Mini Mental Scale Examination (MMSE) and Trail Making Tests—A and B (TMT-A and TMT-B) to test the cognitive impairment. 4 In their study, only 33.73% of participants had cognitive impairment, which is lower than the prevalence found in our study. They identified gender, sedentary lifestyle, duration of diabetes and BMI as independent risk factors for cognitive impairment, whereas we did not find any significant association or correlation between these factors and cognitive impairment.
In a case-control study conducted in Kerala, Addenbrooke’s Cognitive Examination III was used to assess cognitive impairment among 800 participants, which is eight times the sample size of our study. 12 The results showed that cognitive impairment was present in 63.8% of diabetics, which is higher than our study. Interestingly, attention, memory, language and visuospatial were common cognitive domains that were significantly lower in both studies. 12 In a community-based study on cognitive impairment among older adults with diabetes mellitus in Puducherry, 240 older diabetic participants were assessed for cognitive function using the Hindi Mental State Examination (HMSE) tool, which is different from the tool used in our study. The study found that only 30% of study participants had cognitive impairment, which is less than that reported in our study. 13
The present study has certain limitations, such as the fact that the sample size of our study is relatively small, and studies with larger sample sizes are expected to provide more reliable conclusions. The study sample was drawn from a single centre, potentially limiting the generalisability of the findings to other populations, and the reliance on self-reported data for certain variables may have introduced reporting bias. Additionally, the inclusion of only literate diabetic patients in the study limits the generalisability of our findings to illiterate patients, and further research should consider assessing cognitive function among illiterate diabetic patients as well. Furthermore, since we have performed a cross-sectional study, it may be limited in its ability to draw causal inferences. Conducting a case-control study with non-diabetic individuals could strengthen the methodology and provide more accurate results, leading to better conclusions being drawn from the data.
Conclusion
In summary, our study demonstrates a high prevalence of MCI among patients with T2DM, that is, more than half of the study participants reported to having MCI. This highlights the importance of routine cognitive screening for diabetes patients. We found a significant negative association between MoCA scores and glycaemic control parameters such as HbA1c, FBS and PPBS. Further studies are required to determine if improving glycaemic control can lead to improved cognitive function. Our findings suggest the need for further research to better understand the relationship between diabetes and cognitive impairment and to develop appropriate interventions to prevent or manage cognitive impairment in diabetic patients.
Footnotes
Abbreviations
T2DM: Type 2 diabetes mellitus; MoCA: Montreal Cognitive Assessment test; MCI: Mild cognitive impairment; BMI :Body mass index; FBS: Fasting blood sugar; PPBS: Post-prandial blood sugar; ADA: American Diabetes Association; MMSE: Mini Mental Scale Examination.
Acknowledgements
The authors would like to express their gratitude to the Indian Council of Medical Research (ICMR) for supporting this study under the short-term studentship (ICMR STS-2022) programme, which encourages aspiring medical students to get involved in research. The authors express their gratitude to all the study participants for their cooperation. Sincere thanks to the administration of RMC, HOD and faculty in the Department of General Medicine, RMC, for their constant support. The authors are grateful to the Rangaraya Student Research Society (RSRS) for their support and guidance for the research project. A big thanks to all my research mentors, my family and dear friends for their unconditional love and support during my research journey.
Authors’ Contribution
Suvvari TK: conceptualisation, methodology, formal analysis, data curation and writing: original draft, writing: review and editing. Kali CS: conceptualisation, methodology, writing: original draft, writing: review and editing, supervision.
Data Availability
The data of this project is available and can be provided on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was taken from all study participants after explaining the purpose of the research study.
Statement of Ethics
The present study was approved by the Institutional Ethical Committee (IEC) of Rangaraya Medical College, Kakinada, India (Reference No – IEC/RMC/2022/759).