
Abstract
Background
A smartphone is an essential part of our daily existence. Smartphones are used by about 5.26 billion people.
Purpose
The purpose of this study was to determine how the duration of smartphone use influenced brainstem auditory evoked potentials (BAEPs).
Methods
BAEPs were measured using BERAGRAPH in 41 young healthy persons in an observational cross-sectional study.
Results
When daily smartphone calling time is 60 minutes, there is a statistically insignificant difference in smartphone usage length (5 years and >5 years) between the two groups among BAEPs.
Conclusion
Despite the P-value being insignificant, there is a positive relationship between smartphone use in years and absolute wave latencies and interpeak latencies of brainstem evoked potentials.
Keywords
Introduction
It is unnecessary to describe the benefits of using a smartphone or why it is so popular today. A smartphone provides more than just the ability to call and text; it also provides social connection when we need to talk to someone, gaming features when we want to have fun, music and video features, and one of the most sophisticated browsing features that allow users to do, buy and order almost anything at the touch of a button. I imagine that if I had told somebody even 40 years ago about all of this, they would have believed it was a miracle.
One is an addiction to excessive phone use because it becomes a wonderful buddy to humans. Much research has been done to assess the harmful consequences on human bodies, particularly the central nervous system (CNS) and cardiovascular system (CVS). As assessment tools, autonomic nervous system (ANS) testing, visual evoked potential and auditory evoked potential have been used. So, for CNS evaluation, we use brainstem-evoked response audiometry.
The brainstem-elicited response BERA evaluates hearing thresholds and makes diagnoses of retrocochlear abnormalities.
The auditory nerve generates waves I and II, which are followed by the superior olivary complex wave III, the nucleus of the lateral lemniscus wave IV, the inferior colliculus wave V and the thalamus wave VI.
The medial geniculate body generates wave VI, while the cerebral cortex generates wave VII. The graphs show that electrical stimulation of these locations induces delayed responses. When electrical responses are timed, it is possible to establish whether anatomical structures are complete. Electrical impulses pass in milliseconds from anatomical structure to anatomical structure and reactions are ‘time-locked’. 15
The American Electroencephalographic Society (AEEGS) recommends masking white noise at 60 dB pp SPL (1992). The recordings are made with scalp electrodes placed at the midvertex (Cz), the left ear lobule (Al) and the right ear lobule (Ar) (A2). Two-channel recordings are often obtained by originating from the vertex-ipsilateral (Cz-Ai) and vertex-contralateral (Cz-Ac) ears.11–15
Seven waves (I–VII) are typically identified during the first 10 milliseconds of the stimuli. Normal adults undergo Waves I, II, III, IV and V. Waves VI and VII were accurately detected by only 84% and 43% of stimulated ears, respectively. The most noticeable BAEP waves are IV and V.12, 13
In general, BAEPs are analysed for the presence of waves I, Ill and V. Even in healthy patients, the other BAEP components, notably waves Il, IV and VI are inconsistent and unsuitable for clinical interpretation. The following are examples of typical measurements: latency (l) (peak latencies of I, III and V, and I–III, III–V and I–V IPLs).13–15
Materials and Methods
The Department of Physiology at the Institute of Medical Sciences at Banaras Hindu University conducted the current cross-sectional observational study. 41 IMS BHU medical first-year students were involved in this study.
Subjects who were taking psychotropic medications—including antidepressants, antipsychotics and benzodiazepines—or had any concurrent neurological or psychiatric disorders, hypertension, diabetes mellitus or another chronic disease that could cause neuropathy were excluded from this study. Additionally, individuals with hearing disorders, a history of drug abuse or any other types of addiction, such as alcoholism or smoking, were excluded from this study.
Tools Used
A semi-structured Performa was the tool that was utilized to learn more specifically about how individuals used their smartphones.
The institute’s ethics committee gave this study their approval (Dean/2021/EC/2954). The participants gave their informed consent for the data collection. The replies’ confidentiality was guaranteed. Patients were given the assurance that the information would only be utilized for research.
Procedure
The cross-sectional case-control study, which was conducted between October 2021 and October 2022 was approved by the Institute Ethics Committee. As for the subjects for this study, apparently healthy MBBS students from IMS BHU, about 41 of them, were taken, and their BAEP waves and inter-peak latencies were analysed. It was based on the statistical data available that the sample size was chosen.
Subjects must meet the following requirements in order to be included: First-year medical students in the age range of 17–25.
Exclusion criteria:
Existence of diabetes, hypertension or other co-morbid diseases that cause neuropathies Patients with neurological disorders, such as Parkinson’s illness and Alzheimer’s disease Those who have hearing loss or a family history of it Taking sedative and ototoxic medications (e.g., antipsychotics, antidepressants, phenytoin, methyldopa and reserpine) Diagnosis of a mental health conditions Histories of Strokes, serious head traumas and patients with peripheral neuropathy
Many tests were carried out to rule out peripheral neuropathy. Proprioceptive testing is another option to the pencil-back pressure test (sense of the position of joints, both proximal and distal, was tested by asking the subject to keep his eyes closed, followed by rotating a limb in various directions, allowing it to stay in that particular direction and then finally asking the subject to place the other limb in the same position without actually seeing the position of the former limb). Other examinations included a pinprick and tendon pinch pain test, tactile localization and discrimination testing, and temperature tests using warm and cold objects.
The participants’ body height was measured by having them stand firmly against the wall while it was registered on a measuring scale attached to the same wall, after which a flat object was lowered down to the subject’s head.
A computerized device was used to measure the weight. By dividing the participants’ height in square meters by their weight in kilos, the body mass index (BMI) of each subject was calculated. The respiratory rate was gauged. Using the radial arteries, the pulse was counted bilaterally and all results were recorded. With a sphygmomanometer, blood pressure was measured. In normal conditions, BAEP was carried out with the proper BAEP equipment (Medicaid System, 389, Industrial area, Phase-II, Chandigarh). The forehead and mastoid skin were made grease-free after instructing the subjects to feel at ease. The participant was requested to remove any jewellery, cell phones or other objects that would obstruct the procedure. The ground electrode was placed over the forehead, the reference electrode was placed over the mastoid and the active electrode was positioned on the vertex. The wave pattern was observed using brief click monoaural stimuli at an intensity of 80 dB 2000 times (11 per second).
If the perception of sound is not noise, the normal range of sound perception for an apparently healthy person is between 20 dB and 80 dB with small individual variances. Since 80 dB is within this advantageous range, it has been chosen to prevent subjective bias. All waves were captured under the rarefaction setting. The space was silent. In order to ensure that the waveform could be reproduced, at least two readings from each ear were obtained. The absolute latencies of waves I to V as well as the inter-peak latencies I–III, I–V and III–V were recorded, along with the V/I ratio percentage (V/I%). After obtaining the subject’s informed consent, the complete procedure is carried out. During the BAEPs study, the following parameters were recorded.11–15
Wave I: Acoustic nerve (1.4–1.8 ms)
Wave II: The cochlea (2.8 ms)
Wave III: The superior olivary nucleus (3.6–4.1 ms)
Wave IV: Lateral lemniscus’s central nucleus (5.1 ms)
Wave V: Sublateral colliculus (5.5–6.0 ms)
Wave VI: Medial geniculate body
Between the medial geniculate body and the auditory complex, Wave VII begins. 5
Inter-peak latency I–III: 1.6–2.6 ms
I–V inter-peak latency: 3.5–4.5 ms
Inter-peak latency III–V: 1.4–2.4 ms
50–300% is the normal V/I%.
Statistical analysis was done using the SPSS 2021 software pro version by the chi-square test.
Table 1 shows the comparison of absolute and inter-peak latencies of BERA waves (I, III, V, I–III, I–V and III–V) in the two smartphone user groups. These differences were found statistically insignificant.
Comparison of BERA Wave Latencies between Groups of the Duration of ≤5 Years and >5 Years When the Time Spent on a Smartphone on Call Each Day Is ≤60 Min.
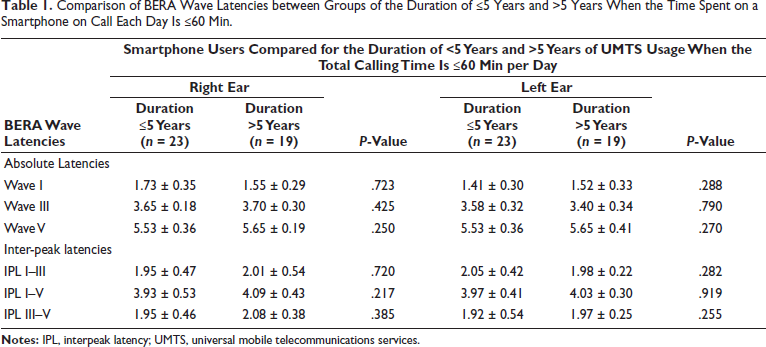
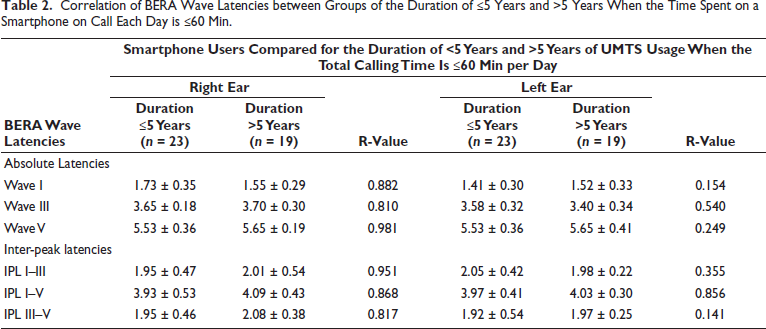
Table 2 shows the correlation of absolute and inter-peak latencies of BERA waves (I, III, V, I–III, I–V and III–V) to the duration of use of a Smartphone. These differences were found to be positively correlated.
Correlation of BERA Wave Latencies between Groups of the Duration of ≤5 Years and >5 Years When the Time Spent on a Smartphone on Call Each Day is ≤60 Min.
Discussion
BERA is the most crucial test used in clinical settings to evaluate changes in hearing threshold, determine the kind of hearing loss and find alterations in the central nervous system. Since it depends on the physical properties of the stimulus (intensity, frequency, inter-stimulus period, etc.) rather than on information from people, its sensitivity for detecting all circumstances has been deemed an objective and non-invasive method.
The current study explains changes in BAEPs in smartphone users who have had less than or equivalent to 5 years or more of calling time of 60 minutes per day.
According to the procedure, at least two BERA recordings were made for each individual to see how the reaction varied.
The results of the current study indicate that there are positive correlations between years of use of smartphones and different wave latencies and IPL although there is no statistically significant difference in the absolute wave latencies of the right and left ears, suggesting that daily usage of UMTS devices for calls lasting up to 60 minutes may not be detrimental acutely, but suggests that it may be harmful chronically with use. Additionally, brainstem transmission time, also known as interpeak latency, is the term used to describe the time delay between the most noteworthy wave I and wave V. In the current investigation, we compared brainstem transmission time (BTT)/ interpeak latency (IPL) between the two groups and discovered that it was insignificant.11, 12 BTT is not impacted by these multiple stimulus factors.11, 12
The likelihood of long-term mobile phone users developing audiological difficulties was investigated in a study by Gupta et al. conducted in India that was remarkably similar to ours (GSM phones). 112 patients who had used mobile phones for a long time (more than a year), as well as 50 controls, underwent a variety of audiological tests. For each of the tested audiological features, there was no appreciable difference between the users and the controls. Yet they got to the conclusion that using a cell phone for a long time and at a loud volume can harm the inner ear. 3
These results are in line with the double-blind study of Parazzini et al, 9 which also found no discernible group difference.8–10
The current investigation, which found no significant immediate effects on the delay of auditory brainstem waves I, III or V following a single 10-minute exposure to 900MHz EMF generated by a commercial mobile phone, is supported by Stefanics et al. 5 According to Bak et al., typical mobile phones have no impact on how electrical inputs travel down the auditory nerve to the auditory brainstem centres. 4
A study conducted on animal models by Kaprana et al. found a significant impact of EMF on the auditory system.6, 7 In research by Dousary et al., a case of a 42-year-old man who had sensorineural hearing loss owing to the Global System for Mobile Phone Use is documented. 1
According to research by Panda et al., prolonged usage of a mobile phone can harm both the auditory cortex and the cochlea. 2
Conclusion
In this present study, a positive correlation is found between the duration of use of Smartphones and absolute latencies, which suggests harmful effects may occur if the duration of use of Smartphones increases, and with the daily increase in usage of smartphones there may be an increase in dysfunction of the auditory system as the auditory system was the most near to the smartphone when we are attending a call, although no statistically significant data were found on independent t-test. Data are limited because the use of smartphones at this extensiveness does not exceed 10 years of use and smartphones are not only used for calling purposes as implicated in our study design.
Future Prospects
In our study, we found that the safe limit of smartphone use per day can be said to be less than one hour per day. More research needs to be done for defining a much more definite calling time limit not only to see its effects on the auditory system but also on other central system effects. It can also be collaborated with screen time to get a much better understanding.
Footnotes
Acknowledgments
A gift of appreciation would be offered to the Institute of Medical Sciences at Banaras Hindu University and its ethics committee for their support and blessing. The authors owe a debt of gratitude to each and every participant for their participation, which was absolutely essential.
Authors’ Contribution
Ayushi Seth: Data collection, paper writing, formatting; Samir Kumar Singh: Conceptualization, review, proof-reading, correspondence; Anita Gupta: Data collection; Hanjabam Barun Sharma: Data analysis.
Participants’ Consent
Full and detailed consent from the participant has been taken. The participant’s identity has been adequately anonymised. If anything related to the participant’s identity is shown, adequate consent has been taken from the participant. The journal will not be responsible for any medico-legal issues arising out of the issues of the patient’s identity or any other issues arising from the public display of information.
Declaration of Conflicting Interests
None.
Disclosure
The authors hereby certify that the work shown here is genuine, original and not submitted anywhere, either in part or full. All necessary permission from the participants and institution has been taken.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
The institute’s ethics committee gave this study their approval (Dean/2021/EC/2954). The participants gave their informed consent for the data collection.