
Abstract
Background
Spontaneous intracerebral haemorrhage (SICH) is the most severe form of all stroke types. Stratification of SICH severity is important for group comparisons and treatment decisions. The existing prognostic scores for clinical prediction in SICH have not been specifically validated in the very old (≥75 years). Therefore, we aimed to evaluate the accuracy of different SICH vital prognostic scores in the very old.
Purpose
To compare the short-term accuracy of three vital prognostic scores: Functional Outcome in Patients with Primary Intracerebral Haemorrhage (FUNC), Modified Emergency Department Intracerebral Haemorrhage (mEDICH) and the Intracerebral Haemorrhage Score (‘ICH score’) in patients aged 75 or older.
Methods
Comparison of the discriminative performance of three SICH prognostic scores in a consecutive case series of patients ≥75 years. The prognostic discrimination was assessed using the area under the receiver operating characteristic curve (AUROC). Additionally, a binary logistic regression was conducted to determine independent prognostic factors associated with mortality.
Results
The case-fatality was 40.6%. The AUROC and Younden index for the three scores was as it follows: ‘ICH score’ 0.882 and 0.648; mEDICH 0.867 and 0.571; FUNC 0.802 and 0.519. The main independent risk factors of death were presence of intraventricular extension (OR = 4.000,95% CI= 1.933–8.276), INR value (OR = 2.173, 95% CI = 1.146–4.117), haemorrhage volume (OR = 1.881, 95% CI = 1.029–3.440) and GCS (OR = 0.119, 95% CI = 0.060–0.236) for mEDICH. Haemorrhage volume (OR = 3.020, 95% CI = 1.806–5.050) and GCS (OR = 0.043, 95% CI = 0.013–0.151) for FUNC. Haemorrhage volume (OR = 4.950, 95% CI = 2.249–10.897) and intraventricular haemorrhage (OR = 3.811, 95% CI = 1.833–7.924) for ‘ICH score’.
Conclusion
The three scores (‘ICH score’, FUNC and mEDICH) showed an excellent capability of discriminating the group of elderly patients at risk of short-term death. Age per se may not be crucial for accurate discrimination of death in the group of elderly. Instead, the inclusion of available physiological markers of fragility would be more scientifically meaningful than age.
Introduction
Spontaneous intracerebral haemorrhage (SICH) is the most severe form among all stroke subtypes with 40% short-term case-fatality. 1 The risk of SICH is highest among older individuals. 2 In the developed world, the life expectancy has been increasing at a rapid rate. In addition, as secondary prevention improves, the usage of antithrombotic becomes also more frequent. 3 Indeed, despite the reduction of SICH incidence, the total number of cases in elderlies continues to grow in some parts of Europe and the United States. 3 In contrast to acute ischemic stroke, there are no treatments or interventions for patients with SICH that can dramatically modify outcomes or reduce long-term disability and mortality. 4 Despite being disproportionately affected, there are few studies that address the short-term prognosis after SICH in the very elderly. 5 Assessing the effectiveness of decisions made during the acute phase, conducting reliable comparisons of outcomes between different cohorts, and analysing temporal trends in mortality in the same clinical settings requires significant or adequate group stratification of the SICH severity.6–8 There are different clinical scores and prognostic tools for survival and functional prediction in patients with SICH. These scores use different laboratory, neurological, radiological, and clinical parameters. 9 Surprisingly, the prognostic accuracy of these scores has never been compared in the fastest and most severely affected SICH age subgroup, the elderly population. We sought to determine the contribution of three different SICH prognostic scores, the Intracerebral Haemorrhage Score (‘ICH Score’), Functional Outcome in Patients with Primary Intracerebral Haemorrhage (FUNC) and Modified Emergency Department Intracerebral Haemorrhage (mEDICH) to the short-term prediction of mortality in very old patients with SICH.
Methods
Population
A retrospective analysis was conducted on prospectively collected data from a single-centre community representative cohort population of SICH in the Algarve region in southern Portugal. 2 As in similar previous studies patients with ≥75 years were considered very old.3, 5 A total of 256 consecutive cases series of SICH patients (January 2009 to December 2016) with ≥75 years (46.6% of the total cases) were included in the study. The original database included patients meeting the following criteria: (a) hospitalisation with a primary diagnosis of SICH according to World Health Organization (WHO) criteria—‘rapidly developed clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than of vascular origin’, 10 and documented with brain computed tomography (CT) or magnetic resonance (MRI). Exclusion criteria encompassed non-SICH (traumatic, structural lesions, and haemorrhagic transformation) as well as non-residents of the region. 11
Prognostic Scales
In a systematic review, the ‘ICH score’, ‘Intracerebral haemorrhage grading score’, ‘modified Intracerebral Haemorrhage Score,’ and FUNC score were identified as the four most extensively validated vital prognostic scores of SICH. 12 After this revision, another score, the mEDICH was published. 13 For this study, the ‘ICH score,’ FUNC and mEDICH scales were selected based on the availability of the following variables: demographics (age, gender), Glasgow coma score (GCS) at admission, medical history prior to intracerebral haemorrhage (including dementia and acute hydrocephalus), neuroimaging variables (intracerebral haemorrhage volume which was measured using the ABC/2 method, presence of intraventricular haemorrhage, hematoma location) and admission international normalised ratio (INR). The outcome of interest was death in the first 30 days after SICH onset representing short-term mortality.
Statistical Analysis
The statistical analysis was performed using IBM SPSS statistics for windows, version 28.0 (IBM corp. Armonk, NY, USA). A comparison of baseline characteristics between 30-day survivors and deceased patients was performed.
Binary logistic regression analysis was utilised to evaluate the independent contribution of each factor in each prognostic scales. Receiver operating characteristic (ROC) analysis was used to compare vital prognostic accuracy among the three scales. For ROC analysis, the FUNC score was inverted, with the lower grades indicating the best outcomes (referred to as the inverted FUNC scale), similar to the ‘ICH score’ and the mEDICH score.
Ethical Approval
The Institutional Ethical Committee approved the study (UAIF 031/2021). This was a strictly observational study and there was no patient contact involved in its implementation. The need for a written consent from patients for this database and the use of the information for research was waived by the institutional ethics committee.
Results
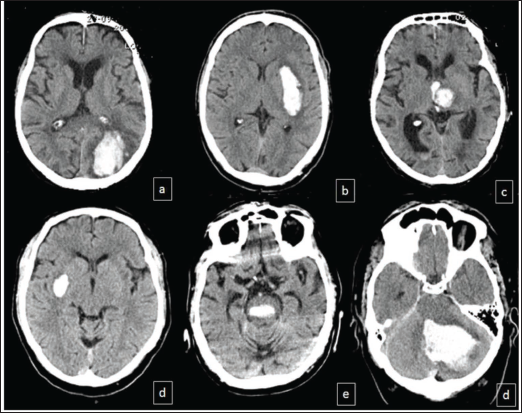
The majority of patients (167/65, 2%) were males. The mean age was 82.1 ± 5 years. The most frequent location of intracerebral haemorrhage was lobar (87 cases, 34%) and basal ganglia (82 cases, 32%). The median hematoma volume was 12.8 cc/cm3 with an interquartile range of 30.8 cc/cm3. Representative images of SICH patients are shown in Figure 1.
Examples of Lobar SICH (a); Deep SICH (b–d): Basal Ganglia (b,d), Thalamic with Intraventricular Haemorrhage (c); Infratentorial (e,d): Brainstem (e) and Cerebellar (d).
The 30-day case-fatality was 40.6%. Table 1 presents the demographic and clinical characteristics and the comparison between the group of living and deceased elderly.
Comparison of Demographic, Clinical, Laboratory and Image Characteristics Between Survivors and Deceased Elderly Patients with SICH.
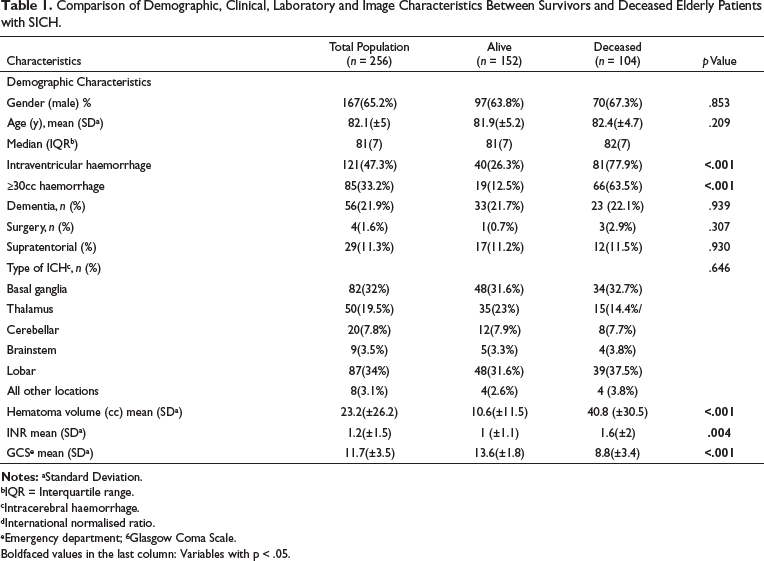
bIQR = Interquartile range.
cIntracerebral haemorrhage.
dInternational normalised ratio.
eEmergency department; 6 Glasgow Coma Scale.
Boldfaced values in the last column: Variables with p < .05.
The results of the regression analysis based on the variables included in each prognostic scores are summed in Table 2.
Logistic Regression Analysis Considering Specific Variables of Each of the Three Models.
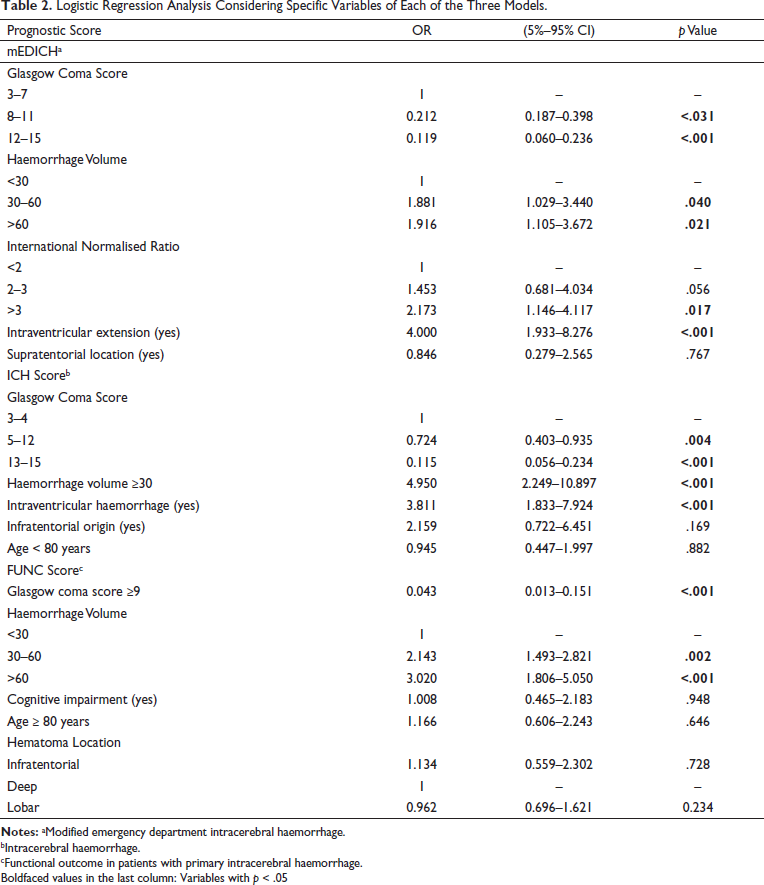
bIntracerebral haemorrhage.
cFunctional outcome in patients with primary intracerebral haemorrhage.
Boldfaced values in the last column: Variables with p < .05
The hematoma location and age did not occur as predictors of death in all scores. Cognitive impairment (FUNC score) also did not occur. The following variables known to predict short-term death after SICH were identified (Table 2): level of consciousness, with patients with higher GCS having reduced likelihood of death in all scores; hematoma volume with higher volume increasing the risk of death in all scores. The presence of intraventricular dissection (‘ICH score,’ mEDICH) and coagulopathy (mEDICH) were also strong predictors of death. The group of deceased patients had higher scores (p < .001) in the vital prognostic scores: 8 versus 6 for FUNC score, and for both mEDICH and ‘ICH score,’ 4 versus 1.
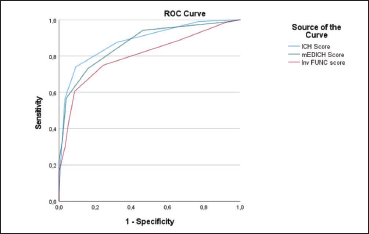
Table 3 shows the results of the ROC analysis. The three prognostic scores demonstrated good discriminative capability, with area under the curve (AUC) values of 0.882, 0.867, and 0.802 for the ‘ICH score,’ mEDICH and FUNC score, respectively. The sensitivity/specificity at maximum Youden index (0.648 for ‘ICH score’; 0.571 for mEDICH; and 0.519 for FUNC score) was: 92.1%/89.6% (‘ICH score’), 90.7%/88.3% (mEDICH) and 89%/92.6% (FUNC score).
Area Under the Curve of Three Vital Prognostic Scores for Spontaneous Intracerebral Haemorrhage in the Very Old.
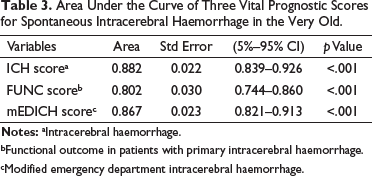
bFunctional outcome in patients with primary intracerebral haemorrhage.
cModified emergency department intracerebral haemorrhage.
Figure 2 presents a graphical comparison of the three curves representing the three prognostic scores.
Discussion
One of the most important aspects when using predictive models is determining their validity and suitability for specific groups. 14 To the best of our knowledge, this is the first study specifically designed to compare the discriminative capacity of different short-term vital prognostics scores in very old patients with SICH. Previous studies evaluated the performance of SICH grading scores in mixed aged populations. In a study by Masotti et al. 15 the ‘ICH score,’ ICH-GS, FUNC and mEDICH scores were compared, and all showed good performance predicting early mortality, with the mEDICH score being the best. 15 In our study, we demonstrated that these three relatively easy to compute vital prognostic SICH scores had excellent discriminative capability in this specific population. These scores use similar SICH severity factors (hematoma volume, location, level of consciousness, age) and other specific factors, including intraventricular haemorrhage (‘ICH Score’ and mEDICH), cognitive impairment (FUNC score) and INR (mEDICH). The ‘ICH score’ had slight better predictive power for mortality at discharge in our study, which aligns with previous studies conducted on non-age selective population that reached similar conclusions.12, 16 The FUNC score showed the lowest discrimination capability in our study. This is somehow expected because the FUNC score was originally designed to assess functional outcomes, not mortality. Additionally, cognitive impairment in our study was only considered in patients with a prior diagnosis of dementia or mild cognitive impairment. Notably, age did not emerge as a predictor of short-term death in this selected group of elderlies, consistent with the results of other studies exclusively focused on very old patients.17–20 This raises the possibility that current prognostic scores that include age are mainly comparing younger with older patients. In a disease affecting mostly elderly people, including age in prognostic scores is questionable at best. Indeed, elderly patients are known to suffer greater early care limitations which reduces survivorship. 21
It is worthwhile to highlight that despite having different variables incorporated, the three validated vital prognostic scales performed well in our specific population. This suggest that their use for investigation and group comparisons is scientifically meaningfully. However, the accuracy is far from perfection, which means that at individual level, the scales should not be used in isolation to predict short-term vital prognosis. Importantly age and hematoma location did not contribute significantly to the prognosis in patients aged ≥75 years with SICH. Given the growing importance of this demographic group, it is time to build specific prognostic scales, with possible incorporation other prognostic factors, for instance functional status, frailty, or specific blood-based biomarkers.
There are some study limitations that are worthwhile mentioning. The sample size was relatively small, and the data was collected from a single centre. This carries the risk of lack of power to demonstrate statically significant differences in some variables and limits the generalisation of the study results. In addition, important variables such as admission NIHSS (national institutes of health stroke score) that would be useful to compare other scores, for instance the modified ‘ICH score’, ICH-FOS (Functional outcome score) and ICH-GS (grading score) that showed good outcome prediction in previous studies were not available.12, 16
Conclusion
In conclusion, we demonstrated that three readily available vital prognostic scores, the ‘ICH score’, FUNC and mEDICH, have excellent capability of discriminating the group of elderly patients at risk of short-term death. Age per se may not be crucial for accurately discriminating death in this elderly population. Instead, the inclusion of available physiological markers of fragility would be more scientifically meaningful than age.
Footnotes
Authors’ Contribution
Conceptualisation: RB, AM; methodology: RB, HN and AM; validation: RB, MP, HB and DC; investigation: RB, MP, HB, DC and AM; resources: RB, MP, HB, DC and AM; writing – original draft preparation: RB, AM and HN; writing – review & editing: RB, HN and AM. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethics
The researchers were the only ones with exclusive access to this database. The data was stored in electronic format and encrypted by the principal investigator. No direct patient contact was included in this study. The scientific use of the data was approved by the local ethics committee and administration board at the Algarve University Hospital Centre (CHUA).