
Abstract
Morquio syndrome is one of the rare storage disorders associated with excessive deposition of keratin sulfate and chondroitin-6-sulfate in bones, cartilages, heart valves, and cornea. Although most individuals with this syndrome appear normal at birth; skeletal abnormalities often develop within the first year of life. Restricted breathing, joint stiffness, and cardiac abnormalities are also common. The multisystem involvement in these patients poses unique anesthestic challenges and there is a paucity of literature regarding the anesthetic management of patients with this condition. We report a successful management of a rare case of 34 years old male with Morquio syndrome who presented an association of acromegaly and was planned for surgical resection of the tumor under general anesthesia. Such rare disorders primarily require thorough knowledge about the disease, its presentation and management strategies for a better outcome. Keeping in mind the multisystem involvement a proper teamwork and coordination of various specialities becomes an utmost importance.
Take home message
Morquio syndrome is a rare storage disorder associated with skeletal, respiratory, and cardiac abnormalities. The multisystem involvement in these patients makes a multidisciplinary approach mandatory for better patient outcomes.
Introduction
Morquio syndrome (mucopolysaccharidosis type IV [MPS IV] or Morquio–Brailsford syndrome) is a rare lysosomal storage disease (LSD) with an autosomal-recessive inheritance. A unique skeletal dysplasia characterizes it with excessive accumulation of glycosaminoglycans, keratin sulfate (KS), and/or chondroitin-6-sulfate (C6S) in bones, cartilages, heart valves, and cornea. 1 Skeletal abnormalities include a bell-shaped chest, a flattened curvature of the spine, shortened long bones, and dysplasia of the hips, knees, ankles, and wrists. Unique anesthetic concerns include distortion of upper airway anatomy secondary to infiltration of respiratory tissues with KS causing difficult airway and alterations in cardiorespiratory function. 2 Infiltration of the cervical spine with odontoid hypoplasia places these patients at risk for atlantoaxial subluxation.
We report an unusual case of Morquio syndrome who presented with features of acromegaly. This case posed unique challenges as it involved the management of airway and systemic complications specifically.
Case Report
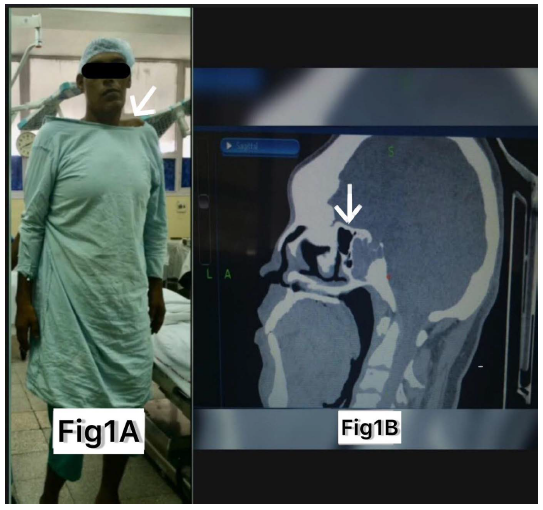
A 34 years old male, a known case of MPS IV-A, weighing 110 kg, was admitted with a history of headaches and gradual loss of vision. He had a tall stature (7 feet 5 inches) (Figure 1a), coarse facial features, a short neck, pectus excavatum with prominent costal margins, with overgrown hands and feet. Detailed radiological and endocrinological workup revealed functional pituitary macroadenoma (26 × 21 × 30 mm), i.e., acromegaly.
(a) A Patient of Morquio Syndrome. (b) CT Scan Depicting Thickened Sellar Floor.
The neurosurgery team planned endoscopic transnasal transsphenoidal surgical resection of the tumor under general anesthesia. Baseline vitals were within normal limits. The plan of anesthesia was general anesthesia (GA) with endotracheal tube (ET) intubation with a video laryngoscope (VL). Smooth intravenous induction was done with propofol and fentanyl (2−4 mics/kg) titrated to loss of consciousness followed by propofol infusion at a rate of 50−100 µg/kg/min. After a check laryngoscopy which revealed a Cormack-Lehane Grade IIb view followed by vecuronium 0.1 mg/kg, the trachea was intubated using a size 8.5 mm cuffed ET with stylet using a VL. After putting the throat pack, arterial and central lines were inserted in anticipation of any hemodynamic instability and to counter any adverse event. The patient was maintained on propofol infusion with oxygen: nitrous oxide 1:1 and dexmedetomidine infusion. The patient’s head was fixed in four pin head holder.
After positioning the abnormally thickened (Figure 1b) and rigid sellar floor needed extensive and labor-intensive drilling due to bone dysplasia associated with Morquio syndrome compounded with bony changes of acromegaly. It generated extensive heat and mechanical failures of sudden breakage of the drill bit can cause inadvertent injury to the nearby vital structures, i.e., carotid and cranial nerves. It may also exacerbate the risk of venous air embolism in these cases. In this case, the patient remained hemodynamically stable and received paracetamol plus diclofenac for intraoperative analgesia. Emergence from anesthesia was slow and gentle. Extubation was performed when the patient was fully awake with adequate muscle power and generated adequate tidal volume. The absence of obstructive sleep apnea (OSA), uneventful intubation at the start, and visibility of full glottis on check VL led us to extubate this patient. He was then moved into the recovery room in an upright position. The postoperative course remained uneventful.
Discussion
Morquio syndrome is a progressive disorder of connective tissue. Accumulation of KS and C6S in connective tissue, skeletal system, brain, heart, liver, spleen, and tracheobronchial tree leads to characteristic physical appearance. Anesthetic implications of Morquio syndrome relate to the end-organ dysfunction and anatomical distortions associated with KS’s intracellular accumulation. 2
This case was particularly challenging because of the accompanying systemic sequelae of acromegaly, i.e., cardiovascular effects, respiratory effects, osteoarthropathy, metabolic complications (insulin resistance, hyperglycemia, and hyperlipidemia), and hypopituitarism.
Morquio and acromegaly can be thought to be contradictory in terms of skeletal dysplasia and stunted growth with the former and unregulated hypersecretion of growth hormone with the latter. On the other hand, airway-related issues and cardiorespiratory complications associated with both of these can be compounded. Hence, a thorough preoperative assessment is imperative.
Morquio syndrome is characterized by odontoid hypoplasia, atlantoaxial instability, and distorted upper airway anatomy. Acromegaly, by causing macroglossia, hypertrophy of epiglottis, tonsils, larynx, and prognathic jaw, magnifies airway difficulty. The mucosal hypertrophy with acromegaly creates a restricted airway and operative corridor. Mallampatti grade may not project an accurate picture of the airway, and a combination of bedside tests is warranted. 3 The functional clinical testing and radiographic examination may not adequately exclude cervical spine instability. 1 In such cases, preoperative multidetector computed tomography can be ordered apart from indirect laryngoscopy and X-ray soft tissue neck to delineate airway anatomy and assist in decision‑making regarding intubation and extubation. Ultrasound for assessment of airway anatomy and preoperative radiographic measurements of tongue size has also been suggested. 4
Awake fiberoptic intubation under dexmedetomidine infusion is considered optimal. 5 Loss of muscular tone and floppy soft tissues after administration of muscle relaxants may make fiberoptic intubation after induction of anesthesia even more difficult.
Though the intellect is normal in these patients, behavioral abnormalities like anxiety and depression are common. 6 OSA in these patients places them at risk of postoperative airway obstruction. A thorough airway examination to evaluate possible risks is the key. MPS IV-induced thoracic cage deformity, kyphoscoliosis, may reduce the long volumes and cause a ventilation-perfusion mismatch. 6 Likewise, in acromegaly, large lung volume and comparatively normal diffusion capacity lead to ventilation-perfusion mismatch. Also, OSA, kyphoscoliosis, and recurrent pulmonary infections lead to the restrictive lung. Attention to maximizing respiratory function preoperatively is essential to avoid postoperative respiratory failure. In Morquios syndrome, cardiac infiltration with mucopolysaccharides may lead to myocardial dysfunction. Aortic regurgitation is the most commonly observed valvular abnormality in these patients. Acromegaly is associated with hyperlipidemia, hyperglycemia, impaired glucose tolerance (IGT), and hypertension (HTN). Diastolic dysfunction occurs early with biventricular concentric hypertrophy. 7 Additionally, valvular disease, arrhythmias and cerebrovascular disease have been described.
Conclusion
A multidisciplinary approach involving various specialities is mandatory. Paramount in the anesthetic care of such patients is proper preoperative evaluation and preparation of the airway in addition to cardiac, respiratory, and neurological dysfunction along with definite plans for the intra-operative period. The sudden breaking of the drill bit might increase the risk of unwitting injury to the nearby vital structures by the surgeon, i.e., carotid and cranial nerves and has not been announced previously in the literature. Cognizance about this allows us to anticipate and detect, keeps us vigil and subsequently refrains such rare complications during the procedure.
Footnotes
Authors’ Contribution
NS and RS: These authors helped with concept, design, writing, editing RC: This author helped with design, literature search, writing, manuscript review and editing.
MT and SK: These authors helped with manuscript preparation and editing.
Statement of Ethics
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.