
Abstract
Background
The burden of stroke is increasing in India, but there is limited understanding of the distribution of reported risk factors in the Indian setting. It is vital to generate robust data on these modifiable risk factors to scale up appropriate strategies for the prevention of cerebrovascular diseases in this setting.
Summary
The objective of this study is to estimate the overall proportion of life style risk factors of patients with stroke in the Indian setting. We searched PubMed and Google Scholar and relevant studies published till February 2022 were included. The risk of bias assessment was considered for the study selection criterion in the meta-analysis. The publication bias was evaluated by funnel plots and Egger’s test. We identified 61 studies in the systematic review and after quality assessment, 36 studies were included for meta-analysis. Random effect model was used due to the significant inconsistency among the included studies (I2 > 97%). The mean age of the participants was 53.84±9.3 years and patients with stroke were predominantly males (64%). Hypertension (56.69%; 95% CI: - 48.45 – 64.58), obesity (36.61%; 95% CI: - 19.31 – 58.23), dyslipidemia (30.6%; 95% CI: - 22 – 40.81) and diabetes mellitus (23.8%; 95% CI: - 18.79 – 29.83) are the leading intermediate conditions associated with stroke. The Physical inactivity - 29.9% (95% CI: - 22.9 – 37.1), history of tobacco use (28.59 %; 95% CI: - 22.22 – 32.94) and alcohol use (28.15 %; 95% CI: - 20.49 – 37.33) were reported as the behavioral risk factors for stroke in this setting.
Key Messages
The current meta-analysis provides robust estimates of the life style related risk-factor of stroke in India based on the observational studies conducted from 1994 to 2019. Estimating the pooled analysis of stroke risk factors is crucial to predict the imposed burden of the illness and ascertain the treatment and prevention strategies for controlling the modifiable risk factors in this setting.
Introduction
Cardiovascular diseases accounted for the majority of deaths globally [18·6 million (17·1–19·7)] in both sexes combined in 2019, amongst which stroke is the second leading cause of death, 3·33 million (3·04–3·62) stroke deaths in males and 3·22 million (2·86–3·54) deaths in females. 1 Disability-adjusted life years (DALYs) for cardiovascular diseases were 393 million (95% UI 368–417) and 143 million (95% UI 133–153) for stroke, making stroke the third-leading cause of disease burden. 2 In India, cardiovascular diseases attributed the highest percent of total death for all ages in which stroke was the fifth leading cause of death in the year 2016, with a mean percent change in the number of DALYs of 52.9% (40.4–66.7) between 1990 and 2016. 3 Within India, a wide variation in the burden of stroke was observed across the states. To cite, a recent meta-analysis reported a one-month case fatality rate of stroke varied from 41.08% to 42.06% in the urban population and 18% to 46.3%.in the rural population. 4 This wide variation could be because of the variability in the distribution of risk factors in the population, effectiveness of health services in preventive, curative, and rehabilitative services, and data availability. 5
The available empirical data reported the risk factors for stroke, such as sociodemographic, behavioral, anthropometric, clinical, and biochemical, from multiple settings in India.6, 7 The significant lifestyle-related risk factors include hypertension, diabetes, hyperlipidemia, obesity, smoking, heart disorders, congestive cardiac failure, atrial fibrillation, left ventricular hypertrophy), and so on, and the burden of each risk factor remains unknown. 8 The global burden of disease study (1990–2016) reported a gross variation in the risk factors for cardiovascular disease across the states of India. 9 It is also evident that South Asians, including Indians, are highly vulnerable to cardiovascular disease because of their cardiometabolic risk profile and ethnically mediated cardiometabolic dysfunction. 10
The burden of stroke is increasing in India, but there is scanty evidence on the systematic understanding of the distribution of its lifestyle risk factors in the Indian setting. It is vital to generate robust data on these risk factors to scale-up appropriate strategies for preventing cerebrovascular diseases in this setting.
Objective
The objective of this study was to estimate the overall proportion of lifestyle risk factors of patients with stroke in the Indian setting.
Materials and Methods
Search Strategy and Selection Criteria
This systematic review is reported following the PRISMA checklist. 11 We searched PubMed and Google Scholar, and relevant studies published till February 2022 were included. We used the combination of Medical Subject Headings (MeSH) and keywords of the following search concepts: “stroke,” “risk factors,” “patients,” and “India.” The details of the search strategy in PubMed are given as supplementary material 1. The data search was carried out by two investigators (BPV and MD). The archives of relevant Indian journals were reviewed for maximum inclusion of available studies. No attempts are made to acquire grey/unpublished literature considering the inherent conflict of interest, which might increase the risk of bias. The screening was performed by two investigators (RK and SS) who further appraised the full texts of appropriated records to reach a common consensus regarding the inclusion and exclusion of individual studies.
Inclusion and Exclusion Criteria
Observational studies, both hospital and community-based stroke registry studies, conducted in the Indian setting reporting the risk factors of various types of strokes and published in the English language were included. Stroke registries are observational databases focusing on the clinical information and outcomes of stroke patients. Stroke is a chronic disease with an acute event, so the hospitalization rate is high. As we were not estimating any incidence or prevalence of stroke, we also included hospital-based clinical studies recognizing its limitations and inherent biases.
Studies were included if participants had a confirmed history of stroke as defined by the World Health Organization (WHO) 12 or as defined according to clinical criteria or confirmed by imaging. Global or Indian studies that exclusively estimated the prevalence, incidence, and mortality data among patients with stroke were excluded. Besides, studies with inadequate data, published as editorials or letters to the editor, conference abstracts, expert opinion, or suggestions were excluded. The lifestyle risk factors for stroke were operationally defined as the conditions and behaviors that increases the chances of an individual to have, develop, or be adversely affected by a disease process. In this study, this was categorized into behavioral risk factors and intermediate conditions. The data on the nonmodifiable risk factors of stroke, such as age, previous history of stroke, and family history of stroke, were not estimated.
Data Extraction
The data extraction was done based on the following study characteristics: author (year of publication)/study region, period of study (year), types of stroke, mean age, gender, sample size, and risk factors (hypertension, diabetes mellitus, tobacco use, alcohol use, dyslipidemia, and others). Three investigators (BPV, JJ, and AV) were involved in the data extraction after reading and discussing the full-text version of the shortlisted publications based on the eligibility criteria. The extracted data were cross-verified by the author VLN and SD. A mutual consensus resolved disagreements between the authors (BV, JJ, AV, VLN, and SD).
Quality Assessment
The Joanna Briggs Institute (JBI) critical appraisal checklist was used for the risk of bias assessment (available from
Statistical Analysis
The R software was used to perform this meta-analysis, and the pooled estimate of the distribution of lifestyle risk factors of stroke was estimated using inverse variance weighting methods. Assuming the significant inconsistency among the studies, a random-effects meta-analysis model was used, and I2 statistics were calculated to measure heterogeneity among studies. The heterogeneity was considered mild, moderate, or high when the I2 values were from 25% to 50%, 51% to 75%, and >75%, respectively. The funnel plot and Egger’s test were used to assess the potential publication bias.
Results
Identification of Studies
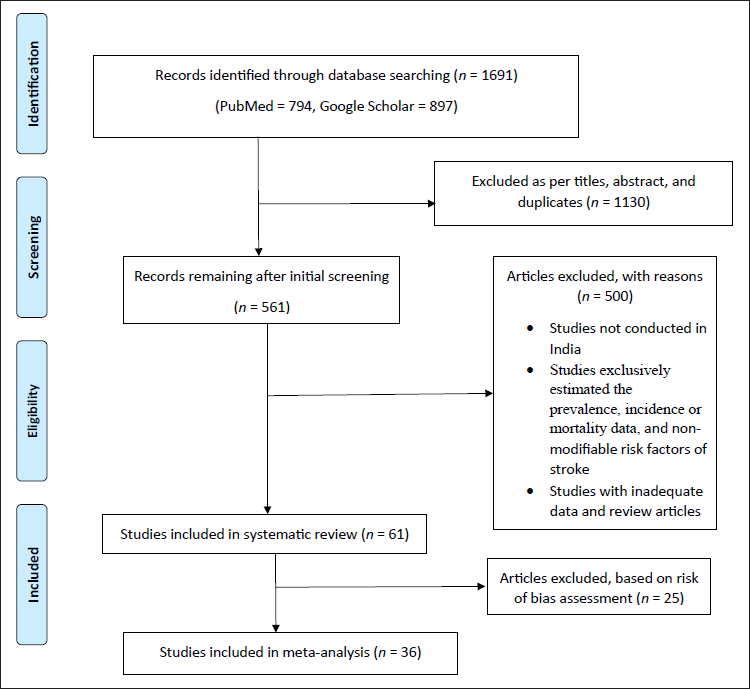
The database search identified 1691 reports: 1130 were excluded based on title and abstract screening, and after eliminating duplicates, 561 articles were retrieved for detailed evaluation, and 500 were excluded for the reasons summarized in Figure 1. Finally, 61 eligible articles were identified after applying the inclusion and exclusion criteria and included in the systematic review, out of which 36 were included in the meta-analysis based on the risk of bias assessment.
Flowchart of Search Strategy and Selection Process.
Characteristics of the Studies Included in the Systematic Review
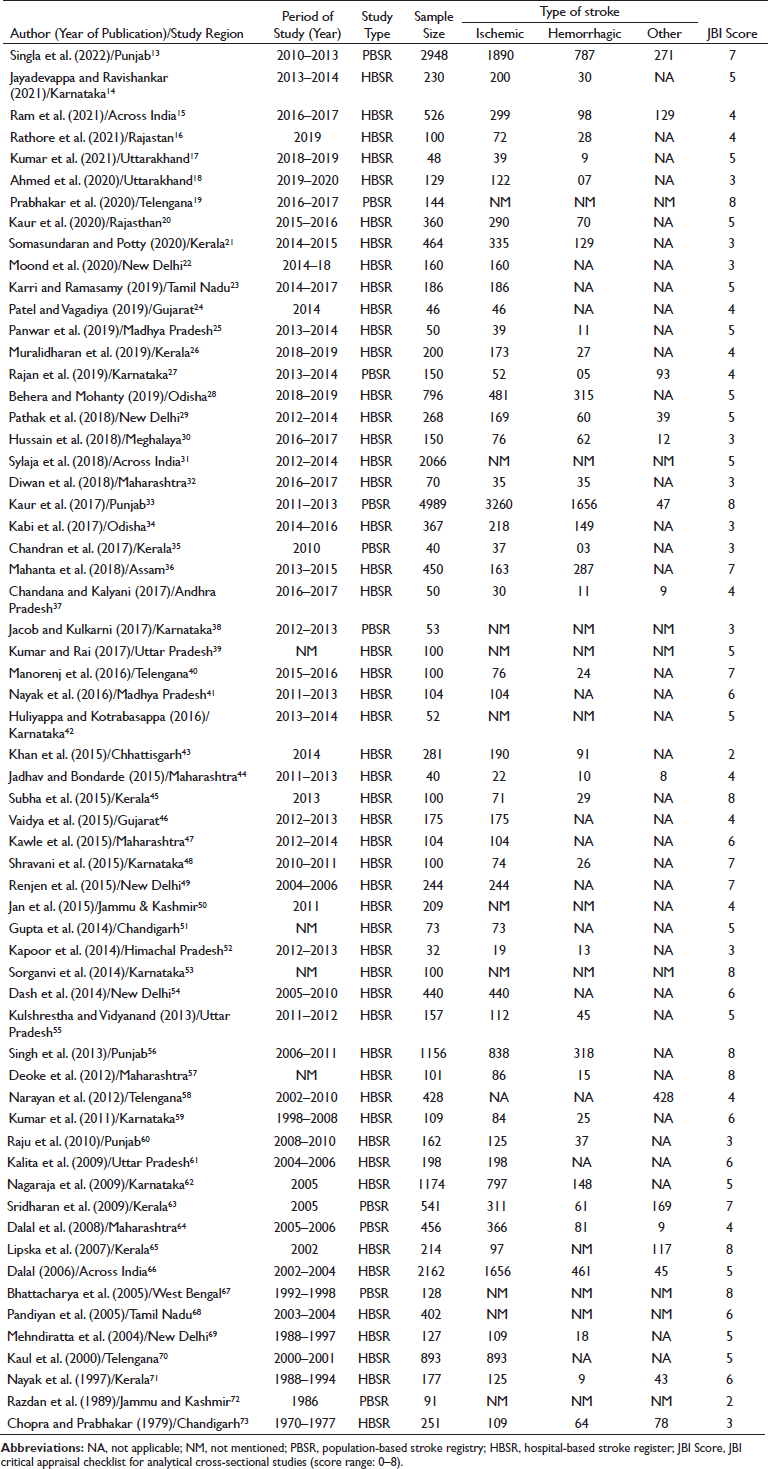
We have included 61 studies in our systematic review, conducted across various states in India, estimating the various lifestyle risk factors for stroke (Table 1).13–73 Out of 61, 56 studies were conducted and 58 were published after 2000. In 51 studies, patients were enrolled from the hospital-based stroke registries (HBSR) maintained in various treatment settings across India, while in 10 studies, the enrollment was using population-based stroke registries (PBSR). The sample size of included studies varied from 32 to 4989. The number of patients with ischemic stroke and hemorrhagic stroke in the included studies ranged from 19 to 3260 and 3 to 1656, respectively. Other types of strokes reported in a few studies varied from 8 to 271.
Characteristics of the Included Studies in the Systematic Review (N = 61).
Description of Studies Included the Meta-Analysis
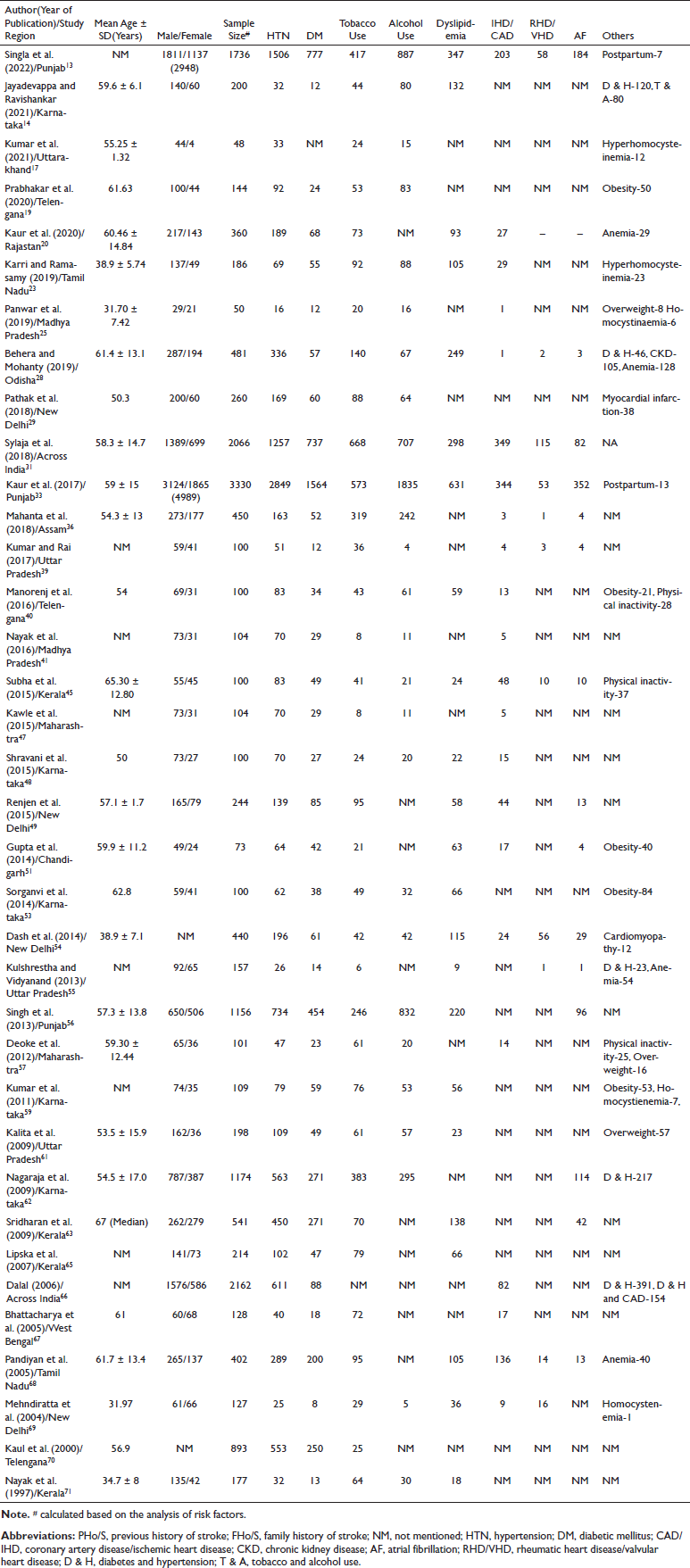
The characteristics of the studies included in the meta-analysis are summarized in Table 2. The meta-analysis included 36 studies, out of which two studies31, 66 were multicentric and the remaining included data from various states of the Indian subcontinent (North: 13,13, 17, 20, 29, 33, 39, 49, 51, 54–56, 69, 61 South: 14,14, 19, 23, 40, 45, 48, 53, 59, 62, 63, 65, 68, 70, 71 East: 3,28, 36, 6 West: 2,47, 57 and Central: 225, 41). The majority of the studies were published in the past decade.13, 14, 17, 19, 20, 23, 25, 28, 29, 31, 36, 39–41, 45, 47–49, 51, 53–57, 59 Overall, 18,315 stroke patients were included, in which the predominant proportion of subjects were males (64%) compared to females (36%). The mean age of the participants was 53.84 ± 9.3 years.
Lifestyle-Related Risk Factors of Stroke Based on the Included Studies in the Meta-Analysis (N = 36).
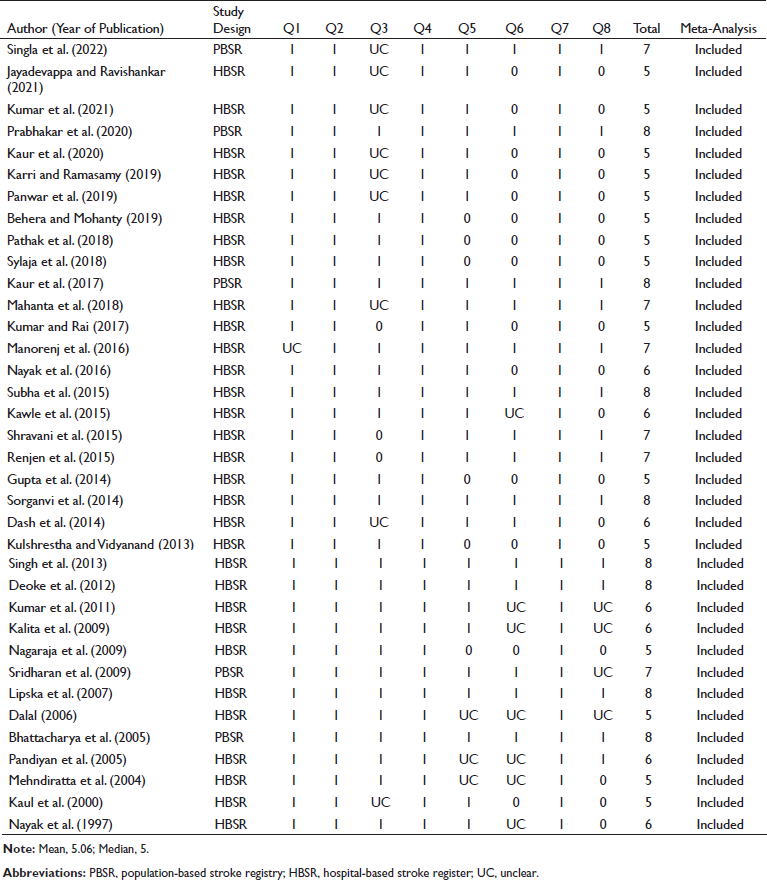
The total score of risk of bias assessment according to the JBI critical appraisal checklist for analytical cross-sectional studies is eight, and the individual scores of the included studies in the systematic review ranged from two to eight. We took an arbitrary cutoff based on the mean and the median scores as there is no specified cutoff for the classification of studies for risk of bias. The mean score of the 38 studies was 5.06, and the median score was five. We considered five as a cutoff point. Finally, 36 studies were included in the meta-analysis. Most studies had credible information about the eligibility criteria, study population, setting, and outcome measures. The reporting structure of the measurement of risk factors for stroke and the influence of confounding variables was poorly followed in more than half of the studies. The details of the quality assessment of the studies using the JBI checklist are described in Table 3.
Risk of Bias Assessment of Included Studies.
Lifestyle Risk Factors for Stroke
Stroke being an end-stage disease, we distributed the risk factors for stroke as behavioral risk factors and intermediate conditions (Figure 2). Hypertension (56.69%; 95% CI [48.45, 64.58]; n = 36 studies), obesity (36.61%; 95% CI [19.31, 58.23]; n = 8 studies), dyslipidemia (30.6%; 95% CI [22, 40.81]; n = 23 studies), and diabetes mellitus (23.8%; 95% CI [18.79, 29.83]; n = 35 studies) were identified as the leading intermediate conditions associated with stroke. The presence of various forms of anemia was associated with 13.3% (95% CI [7.0, 21.2]; n = 9 studies) of the patients with stroke. The occurrence of ischemic heart disease or coronary artery diseases was reported in 8.46% (95% CI [5.07, 13.80]; n = 22 studies) of the study subjects, and 2.82% (95% CI [1.19, 6.54]; n = 11 studies) of the participants had rheumatic heart disease or valvular heart disease. An ECG diagnosis of atrial fibrillation was identified for 4.66% (95% CI [2.87, 7.46]; n = 15 studies) of patients. Approximately 4% (3.94%; 95% CI [2.0, 6.0]) of the patients experienced an episode of stroke during postpartum period.
The Distribution of Lifestyle Risk Factors Among Patients with Stroke in India.
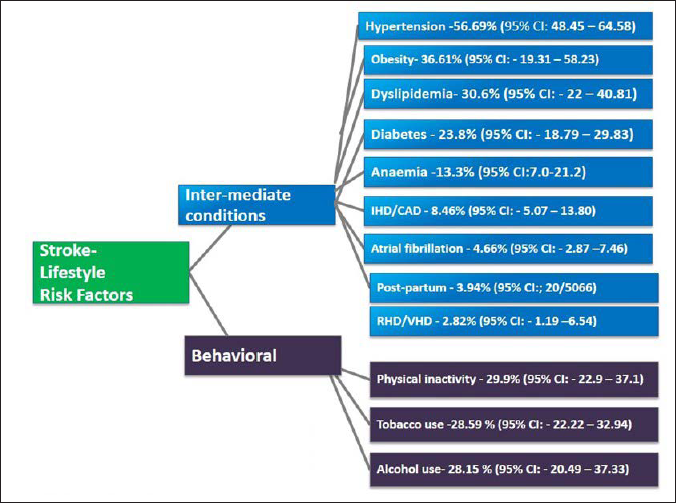
The physical inactivity–29.9% (95% CI [22.9, 37.1]), history of tobacco use, both smoking and smokeless forms (28.59%; 95% CI [22.22, 32.94]), and alcohol use (28.15%; 95% CI [20.49, 37.33]) were the behavioral risk factors for stroke in this setting.
We used the DerSimonian and Laird method of random-effects models to calculate the pooled estimates as there was a significant heterogeneity in the outcome measures (hypertension–I2 = 98.8%, tau squared = 0.92, Q = 2932.05, P < .001; diabetes–I2 = 97.9%, tau squared = 0.74, Q = 1641.78, P < .001; dyslipidemia–I2 = 97.6%, tau squared = 1.03, Q = 909.22, P < .001; atrial fibrillation–I2 = 90.9%, tau squared = 0.70, Q = 154.50, P < .001; tobacco–I2 = 97.3%, tau squared = 0.09, Q = 1238.27, P < .001; alcohol–I2 = 98.2%, tau squared = 1.02, Q = 1422.63, P < .001; IHD/CAD–I2 = 96%, tau squared = 1.40, Q = 525.33, P < .001; RHD/VHD–I2 = 94.5%, tau squared = 1.50, Q = 182.64, P < .001; obesity–I2 = 94.3%, tau squared = 1.04, Q = 122.53, P < .001; previous history of stroke–I2 = 96%, tau squared = 0.61, Q = 447.43, P < .001; family history of stroke–I2 = 92.6%, tau squared = 0.70, Q = 162.83, P < .001). The pooled analysis of the proportion of individual risk factors and heterogeneity are depicted in supplementary materials (Figure S1.1–S1.9)
With the exception of the proportion of studies that estimated diabetes (P = .01), dyslipidemia (P = .02), alcohol (P = .01), and atrial fibrillation (P = .01), Egger’s test revealed no publication bias in the outcome measures (hypertension: P = .53; tobacco: P = .39; RHD/VHD: P = .52; IHD/CAD: P = .39; previous history of stroke P = .12; family history of stroke P = .44). The funnel plot regarding the publication bias of individual risk factors based on the included studies is presented in supplementary materials (Figure S2.1–S2.9).
Discussion
Reducing the burden of stroke in the Indian population requires the identification of modifiable risk factors, and the current meta-analysis provides an aggregate of the distribution of various lifestyle-related risk factors for patients with stroke in the Indian setting. We identified that hypertension (56.69%), obesity (36.61%), dyslipidemia (30.6%), and diabetes mellitus (23.8%) are the leading intermediate conditions associated with stroke. However, physical inactivity (29.9%), history of tobacco use (28.59%), and alcohol use (28.15%) were reported as the behavioral risk factors for stroke in this setting. Referring to some previous studies, there are conflicting results regarding pooled estimates of the risk factors for stroke across Asian countries. 74 Hypertension remains the most common vascular risk factor for stroke in the Asian population74–76 which is consistent with current study findings.
However, the comparisons of the aggregate estimate of the lifestyle risk factors of stroke in this setting should be interpreted based on several contextual factors. First, the high or low frequencies of the occurrence of the risk factors for the noncommunicable disease of a country need to be considered while estimating the specific risk factors for stroke in other countries. For example, a high prevalence of hypertension is seen in Mongolia and Pakistan, which is low in Korea and Singapore. 74 Therefore, a countrywide comparison would be made based on the magnitude of the risk factors predisposing stroke. Second, most of the information on the risk factors among stroke patients was derived from HBSR studies in which data were collected at differing time points with varying definitions limiting its generalization for the estimation of risk factors across countries.77, 78 It is worth noting that estimating stroke risk based on valid risk scoring systems is of pivotal importance for better understanding risk factors to maximize the efficacy of risk reduction efforts. 79
Currently, the burden of stroke is increasing in India, 80 and the findings of this meta-analysis reflect a comprehensive report on the trends of risk factors for stroke in India over a long period. Although several HBSR and PBSR studies were conducted in different parts of India, there is a dearth of evidence of a systematic summary of the risk factor profile of stroke in this setting. This study provides robust estimates of the lifestyle risk factor of stroke in India from 1994 to 2019. The mean age of the participants was 53.84 ± 9.3 years, and a predominant proportion of subjects were males (64%). In contrast to our findings, earlier epidemiological studies in India have found hypertension, diabetes, and cigarette smoking as the leading lifestyle risk factors for stroke. 81 One of the reasons for this change in the risk factor profile for stroke might be because of the varied epidemiological transition among the different states of India. 82 The current findings emphasize that, although the proportion of risk factors for stroke varied considerably across the states of India, the prevalence of hypertension remains the pivotal risk factor across all state groups since 1994. The burden of stroke in the developing world is likely to increase substantially, partly because of ongoing demographic changes, including the aging of the population and health transitions in these countries. 83
The current meta-analysis indicates an urgent need for controlling the vascular and lifestyle risk factors of stroke by focusing more on the public campaign to build the protective factors against cerebrovascular diseases in this setting. There was a significant inconsistency among the included studies as the level of heterogeneity was high (I2 > 94%). The risk of bias assessment of the included studies has implications for the generalization of our findings. Therefore, we exclusively selected stroke epidemiological studies with a low risk of bias conducted in the Indian setting. The current findings provide an evidence base to successfully meet the challenges while devising appropriate strategies to curtail the strategies targeted for risk factor modification.
Strength and Limitations
The primary uniqueness of this study is the novelty of a meta-analysis reflecting the pooled estimate of the proportion of various risk factors of stroke from an Indian perspective. There are certain limitations to generalizing our findings. The results are purely based on observational studies with methodological limitations, such as sampling bias and respondent bias. The level of heterogeneity of the included studies was high because of differences in the study contexts. There might be a chance of contamination of the study subjects, as our estimation is based on the pooled analysis of both hospital and population-based studies, including stroke register studies. The data on clustering risk factors for stroke were not estimated as it was poorly reported in most studies. Despite the limitations, the current meta-analysis provides robust estimates of the lifestyle-related risk factor of stroke in India based on the observational studies conducted from 1994 to 2019.
Conclusion
The present meta-analysis elucidates the overall estimates of lifestyle risk factors for patients with stroke in India. Estimating the pooled analysis of stroke risk factors is crucial to predict the imposed burden of the illness and ascertain the treatment and prevention strategies for controlling the modifiable risk factors in this setting.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for The Distribution of Lifestyle Risk Factors Among Patients with Stroke in the Indian Setting: Systematic Review and Meta-Analysis by Biji P. Varkey, Jaison Joseph, Abin Varghese, Suresh K. Sharma, Elezebeth Mathews, Manju Dhandapani, Venkata Lakshmi Narasimha, Radha Kuttan, Saleena Shah, Surekha Dabla and Sivashanmugam Dhandapani, in Annals of Neurosciences
Footnotes
Acknowledgement
Elezebeth Mathews would like to thank DBT, India for the Clinical and Public Health Early Career Fellowship (grant number IA/CPHE/17/1/503345).
Authors’ Contribution
BPV: conceptualization, data search, data extraction; JJ: data extraction, risk of bias assessment and manuscript drafting; AV: data extraction; EM: risk of bias assessment and intellectual revision including manuscript drafting; MD: data search and editing; RK and SS: screening of the potential references according to the inclusion and exclusion criteria; VLN and SD: cross-verification of data extraction; SKS: risk of bias assessment; SSD: risk of bias assessment (third independent reviewer).
Statement of Ethics
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Elezebeth Mathews is supported by a Clinical and Public Health Early Career Fellowship (grant number IA/CPHE/17/1/503345) from the DBT India Alliance/Welcome Trust-Department of Biotechnology, India Alliance (2018–2023).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.