
Abstract
Background
Polycystic ovarian syndrome (PCOS) has been shown to affect the psychological and cognitive status of a woman. However, amidst various conflicting reports in this regard, very few studies attempted to assess these aspects objectively using electroencephalography (EEG) and event-related potential (ERP).
Purpose
To assess changes in neurocognitive and psychological parameters of PCOS women without any other comorbidities.
Methods
PCOS women aged 18 years to 35 years, diagnosed from obstetrics and gynecology OPD who are otherwise free of any other comorbidities, were assessed for psychological status (anxiety and depression using the State-Trait Anxiety Inventory and Beck Depression Inventory, respectively). Thereafter, a cognitive assessment was done subjectively by the Montreal Cognitive Assessment (MoCA) questionnaire and objectively by using EEG [absolute and relative power of alpha, beta, and theta waves along with theta/beta ratios (TBR) and theta/alpha ratio (TAR)] and P300 amplitude and latency of ERP during a visual oddball paradigm task in control (n = 30) and PCOS (n = 37) subjects.
Results
PCOS women showed significantly higher anxiety and depression scores along with low MoCA scores. Significantly reduced absolute alpha, increased frontal beta, and markedly increased theta (relative) power with increased TAR in the PCOS group were seen. Also, a significant reduction in P300 amplitude with prolonged latency during the visual oddball paradigm task was evident in them.
Conclusion
Reduced alpha and higher theta activity with increased TAR are indicative of poor neural processing ability. Reduced P300 amplitude with more latency also suggests a cognitive decline, which is corroborated by reduced MoCA scores. Our study objectively indicates the presence of subclinical cognitive impairment in PCOS patients even without any comorbidities.
Keywords
Introduction
Polycystic ovarian syndrome (PCOS), presenting with a manifestation of complex symptoms, such as irregular menses, metabolic disturbances, and hyperandrogenism leading to infertility, is essentially a hormonal disorder. Its prevalence is about 3% to 10% among women of the reproductive age group. 1 Besides, increased rates of anxiety, depression, and cognitive dysfunction were reported in PCOS women. 2 Many studies suggested a widespread decline in cognitive performance, which is reflected in terms of episodic memory, executive, and attentional function in PCOS. 3 When women with PCOS underwent diffusion tensor magnetic resonance imaging (MRI) and assessment of cognitive function, the cognitive performance of PCOS subjects was less than that of the controls despite the same educational status when their executive function and episodic memory were assessed. 3 In contrast, in another study, the mental rotation task exhibited significantly higher scores in PCOS women than in control healthy women, which was found to be positively correlated with the increased level of testosterone. 4 Another study reported poor performance on visuospatial working memory, verbal memory, and verbal fluency tasks by PCOS women having higher levels of free testosterone than control women. 5 However, reduction in testosterone levels by antiandrogen therapy in these women did not yield any improvement in cognitive task performance, suggesting thereby no significant effect of testosterone on cognitive performance. 6 Thus, conflicting reports regarding the cognitive performance of PCOS patients exist.
Besides, very few studies, so far, have attempted to address the cognitive aspect of the disease objectively. There are few reports that use robust and objective techniques, such as electroencephalography (EEG) and event-related potential (ERP), to substantiate the cognitive alteration in PCOS. Most of the studies are focused on the subjective assessment methods using cognitive tools, for example, questionnaires or reaction time measurement to given tasks, that too in PCOS women with other associated comorbidities, that is, diabetes, and hypertension. Moreover, the existing research findings are conflicting mainly with reference to confounding factors and the selection of control groups. Early identification of cognitive impairment can help in enhancing the outcomes of the target population. Therefore, the present study aims to assess objectively as well as subjectively the functional changes in neural, cognitive, and psychological aspects in PCOS patients who have not yet developed any associated comorbidities.
Methods
This case-controlled observational study, conducted in the EEG laboratory in the Department of Physiology, was started after obtaining Institute Ethical Committee approval. Informed written consent was obtained from all the volunteers before the conduction of the study. Thirty-seven patients with PCOS attending the OPD of obstetrics and gynecology with the following inclusion criteria 7 were recruited for the study: (a) women aged 18 years to 35 years who are diagnosed with PCOS as per PCOS criteria; (b) presence of oligo and/or anovulation (intermenstrual interval ≥35 days and/or presence of ≤8 cycles per year); (c) Clinical signs of biochemical evidence of hyperandrogenism (obesity, hirsutism, acne, seborrhea, loss of hair, and elevated testosterone levels); and/or (d) polycystic ovary in ultrasonography. Pregnant or lactating women, women with physical and/or cognitive limitations that may affect their ability to answer the questionnaire, women with any history of drug intake, for example, oral contraceptives, androgens, steroids, antiepileptics/antipsychotic drugs, or drugs interfering with glucose/lipid metabolism, and women with diabetes, hypertension, or chronic illness/endocrinological/psychiatric/neurological disorders were excluded from the study. Age-matched normal healthy women (n = 30) with a body mass index (BMI) of 19 to 24 were taken as controls.
All baseline anthropometric and physiological variables, including waist to hip ratio, height, weight, BMI, blood pressure, resting heart rate, and respiratory rate, were recorded. Psychological variables such as anxiety and depression were assessed by asking the subjects to fill in the prescribed questionnaire. Spielberg’s standard self-rating Form Y of State-Trait Anxiety Inventory (STAI) Scale 8 was administered to calculate the state and trait anxiety scores. Beck Depression Inventory (BDI) 9 was used to assess the depression status of each subject. Thereafter, a subjective cognitive assessment was conducted by the examiner by administering Montreal Cognitive Assessment (MoCA) form. Different cognitive domains such as attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculation, and orientation, as well as total scores by the MoCA questionnaire, were calculated. 10
Thereafter, the cognitive profile of the subjects was assessed objectively using the following EEG and ERP tests.
Electroencephalogram (EEG): EEG was recorded with the help of a 64-channel Brain Electro Scan System (B.E.S.S.) machine from Axxonet System Technologies Private Limited, Bengaluru, Karnataka, India. Thirty electrode saline head cap (following 10–20 systems of electrode placement) with a sampling rate of 1,000 Hz and impedance < 20 kΩ was used with midpoint between Fz and Fpz (AFZ) as ground and electrode placed at the vertex (Cz) was used as reference. After 15 min of rest, the recording was started while the subject remained in awake and relaxed conditions with the eyes closed for 20 min. Thereafter, re-referencing of EEG data was done offline, followed by visual inspection for eye-blink and gross movement artifacts. For this, a rejection criterion of ±75 µV was used with the help of the 6.9_1 version of the B.E.S.S. software. The high-pass, low-pass, and notch filter frequencies were 1 Hz, 70 Hz, and 50 Hz, respectively. Then, a fast Fourier transformation was done to decompose the EEG waveform (15 min of artifact-free epochs, i.e., at least 450 epochs of two sec/subject) into the respective frequencies of sine wave components. The absolute power (10 log10µV2/Hz) of alpha (8–12 Hz), beta (13–35 Hz), and theta (4–7 Hz) waves was then computed, and their calculated ratios, namely theta/alpha ratio (TAR) and theta/beta ratios (TBR) along with relative power of alpha, beta, and theta waves from frontal (Fz) and parietal (Pz) electrode sites with Cz used as a reference, were measured.
11
Event-Related Potential (ERP): The B.E.S.S. EEG/ERP system was used to record ERP by administering a visual oddball paradigm (V-OP).
12
In this protocol, the subject sat at a distance of approximately 1 m from a computer screen in a darkened room while two types of visual stimuli were presented on the screen: one frequent (image of the square) with an 80% occurrence rate and one rare (circle) with 20% occurrence. In Block 1, the subject was asked to press a key on the number pad after the presentation of the rare image. In Block 2, the instructions were reversed, and the subject was asked to press the key when they saw the image of a square (rare stimulus).
After offline re-referencing, ERP waveforms were converted into epochs, time-locked to the frequent and rare images using “B.E.S.S.” software (version 6.9_1). P300 components of ERP (latency: from the onset of the stimulus to the positive peak in milliseconds and amplitude: from baseline to the highest point of the positive peak in µV) were calculated from different brain regions (Fz, Cz, and Pz) by averaging subjects’ responses to 240 presentations in each block of the recording setup. 11
Statistical Analysis
The analysis was done using SPSS (version 24, 2009) software. For normally distributed variables, within-group comparison was done using a paired, independent sample t-test, whereas, for non-normally distributed variables, the Wilcoxon signed-rank test was done. On the other hand, the intergroup analysis (PCOS versus control) was done by unpaired t-test and Mann–Whitney U-test for normally distributed and non-normally distributed variables, respectively. Two-way and three-way ANOVA were employed to evaluate the effects of different factors. Then, the means of variables among the studied groups were compared by post hoc Duncan’s multiple range test.
Results
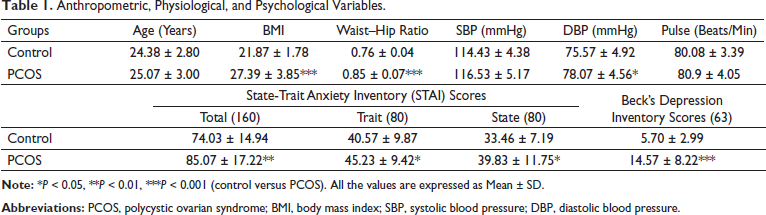
Anthropometric, Physiological, and Psychological Variables.
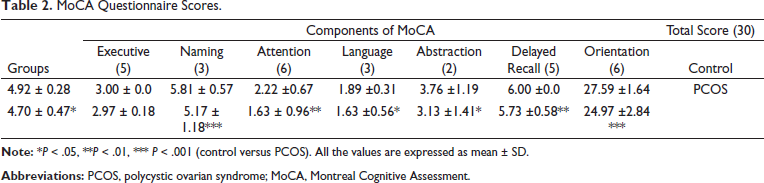
MoCA Questionnaire Scores.
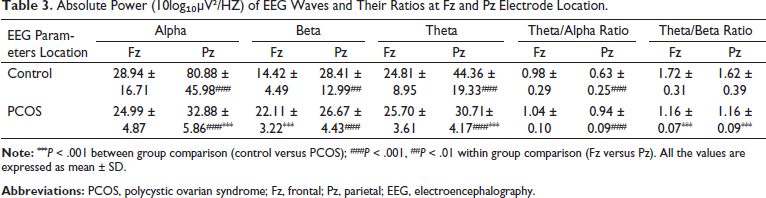
Absolute spectral power of resting alpha and theta at the Pz site was significantly lower (P < .001) and resting beta at the Fz site was higher in comparison to the control group (Table 3). TBR was found to be significantly less at both Fz and Pz sites compared to control subjects (Table 3). A highly significant effect of cortical recording sites (i.e., Fz and Pz) on all the EEG activities for both the groups, except for TBR (Supplementary Table 1), was evident from the two-way ANOVA test. The location versus group comparison also showed a highly significant (P < .001) effect on all EEG activities except TBR (Table 3). The post hoc analysis revealed no difference in the alpha activity at Fz and Pz but was significantly lower when compared to the control group (Figure 1a). The beta activity in both the groups was similar and significantly higher posteriorly (Figure 1b), whereas a significant decrease in TBR at both Fz and Pz locations was obtained in PCOS compared to healthy controls (Figure 1e).
Absolute Power (10log₁₀µV²/HZ) of EEG Waves and Their Ratios at Fz and Pz Electrode Location.

Post hoc analysis at the level of p < 0.05, for absolute power of Alpha (1a), Beta (1b), Theta (1c), Theta/Alpha ratio (1d) and Theta/Beta Ratio (1e) at Fz and Pz, depicted by alphabets. Highest and lowest means are indicated by ‘a’ and ‘b’ alphabets, where same alphabet denotes non-significant difference among the groups. The Power Spectral Density map shows resting EEG waveforms in control (A) and PCOS (B) subjects.
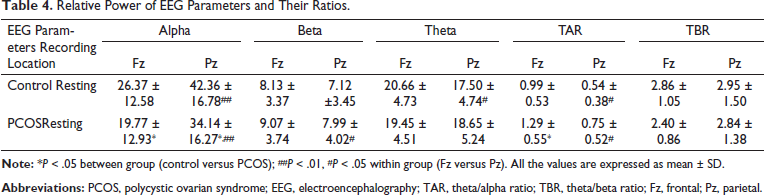
Relative Power of EEG Parameters and Their Ratios.
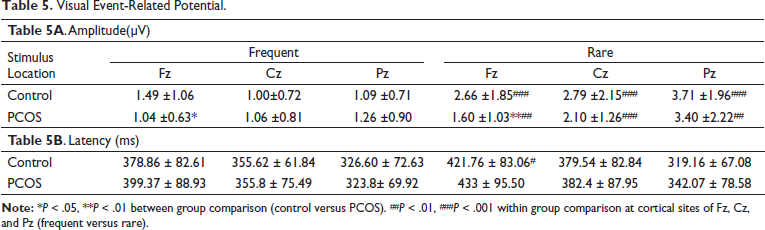
During V-OP, PCOS subjects showed a significantly higher amplitude of P300 for rare stimuli at all the recorded cortical sites (Fz, Cz, and Pz) compared to frequent stimuli (Figure 2a). However, a lower amplitude was seen in the PCOS subjects than in the controls at all the cortical sites (Fz, Pz, and Cz) for rare stimuli and at Fz for frequent stimuli. A significant effect of the location (Fz, Cz, and Pz, P < .001), type of stimuli (frequent and rare, P < .001), and groups (control and PCOS, P < .01) on the P300 amplitude of VERP (Supplementary Table 2) was also present, as revealed by three-way ANOVA. Rare stimuli showed a markedly higher P300 latency compared to frequent stimuli in PCOS subjects at Fz, Cz, and Pz, although none of them was statistically significant (Table 5). A clear trend of higher latency in PCOS subjects for rare stimuli at all three recording sites and frequent stimuli at Fz and Cz was observed when compared with control subjects, although none of them was statistically significant (Figure 2b). Three-way ANOVA revealed that P300 latency was significantly affected by the location (electrode sites) and the type of stimuli (frequent or rare) but not by the study groups (Supplementary Table 2).
Post hoc analysis (at the level of p < 0.05) shown as alphabets for P300 amplitude (2a) and latency (2b) of VERP for frequent and rare stimulus at different cortical sites (Fz, Cz, Pz) in control and PCOS groups. Highest to lowest means are indicated by ‘a’ to ‘e’ alphabets, where same alphabet denotes non-significant difference among the groups. The left panel shows grand average of P300 waveform for Frequent (A) and Rare (B) stimulus in control and PCOS subjects.
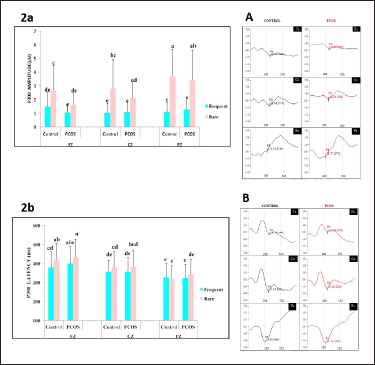
Visual Event-Related Potential.
Discussion
In our study, it was ensured that all the recruited PCOS patients were not suffering from any frank comorbidities such as diabetes, hypertension, or any other systemic/autonomic/endocrinological diseases. This was done to see if these patients, who are yet free of these associated comorbidities with PCOS, show evidence of any neurocognitive changes. Also, the age group of the subjects was kept between 18 years and 35 years so that the disturbed/altered physiological and endocrinological changes in relation to menarche and menopause could be avoided. PCOS patients had significantly higher BMI than the control subjects, which corroborates the fact that more than 50% of women with PCOS are overweight or obese. 12 The waist to hip ratio was also significantly higher in PCOS compared to controls. Although in the present study, we did not consider the hormonal profile of the subject, a high waist to hip ratio may be considered a morphological sign of hyperandrogenism and may serve as an appropriate parameter in assessing the incidence of insulin resistance and cardiovascular events in PCOS patients. 13 It may be added here that we followed strict inclusion and exclusion criteria and only normotensive PCOS women were included in this study. Still an increased diastolic blood pressure (BP) in them (although within physiological limits) as compared to healthy controls suggests the potential of developing hypertension in the future.
Psychological Status: STAI evaluation showed significantly higher state as well as trait anxiety in PCOS patients. 14 In this context, it may be mentioned here that the trait anxiety is known to represent subjects’ general vulnerability to emotional distress and psychological disorders as they are highly associated with psychological disorders in terms of subjective feelings of well-being, physical wellness and ailments, social and occupational afflictions, and relationship quality and happiness. 15 Thus, a significantly higher trait anxiety score (45.23 ± 9.42), as seen in our study group also, indicates their increased vulnerability to emotional distress. People with high trait anxiety tend to assume various circumstances as harmful and frightening, thereby becoming more prone to stress and, therefore, exhibiting heightened state anxiety more often. 15 As reported earlier, a cutoff score of 39 to 40 for state anxiety indicates the presence of clinically significant symptoms, and thus, PCOS patients in our study exhibited significant state anxiety with a score of 39.83 ± 11.75. 14
On the other hand, significantly more depression was also found in PCOS women than in their healthy counterparts. The BDI questionnaire used in our study to assess depression status has been analyzed based on the following cutoff guidelines: score range of 0 to 13, 14 to 19, 20 to 28, and 29 to 63 for no depression, mild depression, moderate depression, and severe depression, respectively. 9 Therefore, our PCOS patients with a BDI score of 14.57 ± 8.22 falls into the category of mild depression.
The higher prevalence of anxiety and depression in PCOS women is for multiple reasons, such as external features of hirsutism, cystic acne, seborrhea, and alopecia, along with the associated social stigma because of its various consequences, for example, irregular menstrual cycles, infertility, and obesity; thus, PCOS is rightly termed as the “thief of womanhood.” 16 The anxiety and depression in PCOS women are in turn associated with a poor quality of life. It is suggested that this psychiatric morbidity is the mediator of a poorer quality of life (QoL) in patients with PCOS. 17 Although clinically significant psychiatric distress is present in only a proportion of patients, subclinical levels of distress are very common in PCOS patients and can have profound effects on QoL. 17
This supports the fact that even in the absence of any frank comorbidities, PCOS patients show evidence of a psychologically disturbed state, which can be either because of the external features, social stigma, and infertility 16 or because of the underlying reproductive and metabolic abnormalities, for example, hyperandrogenism and insulin resistance 18 associated with PCOS.
Cognitive Assessment:
MoCA Test: The subjective cognitive profile of PCOS patients had a total MoCA score of less than 26 in our study, which can be labeled as mild cognitive impairment.
19
Besides, concomitant reduction in all its components like execution (visuospatial), attention, language, abstraction, and memory (working memory) and orientation to time and place
10
in the PCOS women also indicates global impairment in cognition to a certain degree. Previous studies utilizing such subjective measures have also shown a cognitive decline in women with PCOS.
19
Resting EEG: The objective assessment of the cognitive profile by the resting EEG analysis exhibited some interesting features. We observed a significant topographical difference in the spectral power of resting EEG in the control group and PCOS group. The alpha activity is linked to both basic cognitive features like memory and attention,
20
as well as with complex cognitive performances, for example, contrasting thinking and creative ideation,
21
whereas its presence in the posterior location is positively linked to the individuals’ cognitive profile.
22
Alpha activity showed a marked decrease in the frontal location and, significantly, the posterior location in PCOS compared with the controls. However, the absolute beta power activity was significantly increased in the PCOS group in the Fz location, which was apparent in their relative power too. Increased beta rhythm activity, mainly in the frontal cortex, was also reported in another study done on patients with anxiety,
23
whereas reduced alpha rhythm was reported in patients with chronic anxiety.
24
This can be correlated to our present study where PCOS patients who showed increased beta activity in resting EEG also had high scores of traits as well as state anxiety. With regard to theta activity, the PCOS group as compared to control subjects in our study manifested a significantly decreased posterior resting absolute theta power. Cognitive impairment has been linked to increased theta and decreased alpha power in adults with Alzheimer’s disease.
25
However, we found significantly decreased spectral power of theta posteriorly in the PCOS area, and alpha power decreased in both frontal and posterior areas. However, on further analysis of the relative power of these waveforms, theta power showed a slight increase in both Fz and Pz areas, although insignificantly with relative alpha showing a decrease. Therefore, it may be said that the observed small increase in relative theta power is suggestive of early signs of reduced cognitive status in PCOS patients. The findings of alpha and beta activity in PCOS indicate heightened anxiety. PCOS women showed markedly high resting TAR than their control counterparts in both frontal and parietal areas. Several studies have shown that high values of TAR indicated worse neuropsychological test performance in several cognitive domains.
26
So, a higher TAR (though nonsignificant) recorded in our study in PCOS women suggests early/mild cognitive changes in them. However, resting TBR in the PCOS subjects did not show a significant change from their healthy counterparts. TBR has an inverse relation to cognitive processing efficiency and is used as a marker for the assessment of cognitive control of the executive and attentional domains in healthy individuals,
27
but early/mild cognitive alteration in PCOS subjects with no other comorbidities at the time of recording might not be reflected in TBR. P300 Amplitude and Latency of Visual-ERP: As expected, P300 amplitude was larger during rare stimuli presentation because of the requirement of highly complex neural processing.
28
In contrast, significantly lower P300 amplitude in the PCOS subjects frontally (Fz) during both frequent and rare stimuli and centrally (Cz) and parietally (Pz) during rare stimuli is a clear indication of slower and poorer processing of stimuli in these subjects. The P300 amplitude is more connected to the processing of cortical activity during working memory.
29
This becomes more important because of the reduction seen in Cz and Pz sites of our PCOS subjects, as the largest P300 is usually seen in centroparietal scalp areas.
30
Rare stimuli normally require more complex neuronal processing.
28
Thus, lower cognition in PCOS is reflected in both reduced P300 amplitude and also the subjective MoCA scores in our study.
At the same time, the P300 latency was markedly increased in the PCOS group for rare stimuli at all locations and Fz for frequent stimuli. Several reports have shown that P300 latency is negatively correlated with mental function. 29 It represents the processing time needed to generate a response. Thus, a longer latency indicates slowing of cognitive function 31 and has been used as a biomarker of mild cognitive impairment. 32
Conclusion
Our study objectively demonstrates evidence of subclinical cognitive impairment even in those PCOS women who do not have any comorbidities and indications of any frank impairment in terms of cognitive aspects. A similar recent report by Velusami et al. also suggested subclinical cognitive impairment in adolescent girls diagnosed with PCOS. 33 With respect to psychological disturbances, most of the earlier studies have documented significant depression and other behavioral changes in all PCOS women. In contrast to that, our study demonstrates the presence of high anxiety and mild depression in PCOS women who were relatively free of any clinical manifestations of the disease in terms of diabetes, hypertension, etc., at the time of the study. Hence, the study warrants early interventions in these patients to improve quality of life through psychological counseling and maintaining a healthy, active physical and mental lifestyle. Such timely interventions may prevent/reduce the chance of future frank cognitive disabilities and significant clinical impairment in the cognitive aspects of these individuals.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for EEG-ERP Correlates of Cognitive Dysfunction in Polycystic Ovarian Syndrome by Neethu Showkath, Meenakshi Sinha, Jayshri R. Ghate, Sarita Agrawal, Sucharita Mandal and Ramanjan Sinha, in Annals of Neurosciences
Footnotes
Acknowledgement
We gratefully acknowledge the contribution of all the subjects who participated in the study.
Authors’ Contribution
NS: Manuscript preparation, data collection, and analysis. MS: Conception of the study, manuscript preparation, and editing. JRG: Conception of the study, manuscript preparation, and editing. SA: Data collection, manuscript preparation, and editing. SM: Data collection, manuscript preparation, and editing. RS: Conception of the study, critically revised the manuscript, and editing.
Statement of Ethics
This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki complying with the guidelines for human studies. The study was started after obtaining approval from Institute Ethical Committee. Informed written consent was obtained from all the volunteers before the conduction of the study.
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.